
From the 1Department of Orthopedics, Fenghua People’s Hospital, Ningbo, Zhejiang, 2Department of Sports Medicine, Shanghai Jiao Tong University Affiliated Sixth People’s Hospital, Shanghai and 3Hand surgery,The first hospital of JiLin University, Changchun China
Objective: To investigate the effect of hyaluronic acid on functional recovery and pain control in patients following knee arthroscopy.
Design: A systematic review and meta-analysis was conducted to explore the efficacy of hyaluronic acid following knee arthroscopy.
Subjects and methods: Randomized controlled trials (RCTs) assessing the effect of hyaluronic acid in knee arthroscopy were included. A meta-analysis was performed using the random-effect model.
Results: Six RCTs involving 310 patients were included in the meta-analysis. Overall, compared with control intervention following knee arthroscopy, hyaluronic acid treatment was found to significantly increase Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) scores (mean difference 11.43; 95% confidence intervals (95% CI) 1.39–21.47; p = 0.03), but had no impact on pain scores at 2 weeks (mean difference –0.16; 95% CI –0.81–0.49; p = 0.63), pain scores at 6 weeks (mean difference 0.01; 95% CI –0.86–0.89; p = 0.98), pain scores at 12 weeks (mean difference –0.51; 95% CI –1.56–0.53; p = 0.34). In addition, pain on motion was significantly reduced after knee arthroscopy (risk ratio (RR) 0.22; 95% CI 0.06–0.79; p = 0.02).
Conclusion: Compared with control intervention after knee arthroscopy, hyaluronic acid treatment was found to significantly improve WOMAC score and decrease pain on motion, but had no substantial influence on pain scores at 2, 6 and 12 weeks after knee arthroscopy.
Key words: hyaluronic acid; knee arthroscopy; WOMAC score; viscosupplementation; meta-analysis.
Accepted May 17, 2018; Epub ahead of print Oct 9, 2018
J Rehabil Med 2018; 50: 00–00
Correspondence address: Xingguang Yang, Department of Sports Medicine, Shanghai Jiao Tong University Affiliated Sixth People’s Hospital, No. 600 Yishan Road, Shanghai, 200233, China. E-mail: hsjj22@sina.com
Hyaluronic acid might be beneficial for patients after knee arthroscopy. However, the results remain controversial. A systematic review and meta-analysis was conducted to explore the efficacy of hyaluronic acid following knee arthroscopy. Randomized controlled trials assessing the effect of hyaluronic acid in knee arthroscopy were included. Compared with control intervention after knee arthroscopy, hyaluronic acid treatment was found to significantly improve Western Ontario and McMaster Universities Osteoarthritis Index scores and decrease pain on motion, but had no substantial influence on pain scores at 2, 6 and 12 weeks after knee arthroscopy.
In the short-term postoperative period after knee arthroscopy patients frequently experience pain, swelling and impaired function (1–3). Knee arthroscopy is widely used for anterior cruciate ligament reconstruction, meniscus tear, and arthroscopic debridement. Currently, several analgesics are used for pain control following arthroscopic knee surgery, resulting in some adverse events (4, 5). During knee arthroscopy, the normal hyperviscous synovial fluid is replaced by irrigation fluid (normal saline), which is further replaced by new, naturally formed synovial fluid after the surgery. The irrigation fluid not only facilitates the removal of harmful debris, but also dilutes the hyaluronic acid layer covering joint tissues (e.g. cartilage). Irrigation fluids have been reported to have a negative effect on the metabolism and structure of the joint cartilage (6–9).
Hyaluronic acid, a complex glycosaminoglycan, is an important component of synovial fluid and cartilage matrix, which lubricates and allows smooth and pain-free joint motion (10–12). Hyaluronic acid could promote homeostasis of the joint environment and serve as a semipermeable barrier to protect the cartilage from the free movement of lytic enzymes, inflammation mediators, and inflammatory cells in the synovial fluid (13–15). In addition, hyaluronic acid has been reported to relieve joint pain and prevent the progression of cartilage degeneration in osteoarthritis (16). Exogenous hyaluronic acid injected into the arthritic joint space has been shown to improve the qualitative and quantitative properties of endogenous hyaluronic acid and therefore improve joint lubrication (17). In a randomized controlled study (RCT), intra-articular hyaluronic acid was reported to improve pain control and swelling after arthroscopic anterior cruciate ligament reconstruction (18).
In contrast to this promising finding, however, some RCTs have shown that hyaluronic acid has no influence on Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) scores, and pain scores at 2 and 6 weeks following knee arthroscopy (19–21). Considering these inconsistent effects, we therefore conducted a systematic review and meta-analysis of RCTs to evaluate the effectiveness of hyaluronic acid after knee arthroscopy.
This systematic review and meta-analysis was conducted according to the guidance of the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) statement (22) and the Cochrane Handbook for Systematic Reviews of Interventions (23). All analyses were based on previous published studies, thus ethical approval and patient consent were not required.
PubMed, Embase, Web of Science, EBSCO, and the Cochrane Library were systematically searched from inception to September 2017, with the following key words: hyaluronic acid, and knee arthroscopy. To include additional eligible studies, the reference lists of retrieved studies and relevant reviews were also hand-searched and the process above was performed repeatedly until no further article was identified. Conference abstracts meeting the inclusion criteria were also included.
The inclusion criteria were: study population, patients undergoing knee arthroscopy; intervention, hyaluronic acid injection; control intervention, normal saline or no injection; outcome measure, WOMAC scores; and study design, RCT. Patients receiving local anaesthetic in the control group were excluded.
The following information was extracted for the included RCTs: first author, publication year, sample size, baseline characteristics of patients, hyaluronic acid, control, study design, WOMAC scores, pain scores at 2, 6 and 12 weeks, pain on motion. The author would be contacted to acquire the data when necessary.
The primary outcome was WOMAC score. Secondary outcomes included pain scores at 2, 6 and 12 weeks, pain on motion.
The Jadad scale was used to evaluate the methodological quality of each RCT included in this meta-analysis (24). This scale consisted of 3 evaluation elements: randomization (0–2 points), blinding (0–2 points), dropouts and withdrawals (0–1 points). One point would be allocated to each element if it was mentioned in article, and another 1 point would be given if the methods of randomization and/or blinding had been described appropriately and in detail. If methods of randomization and/or blinding were inappropriate, or dropouts and withdrawals had not been recorded, then 1 point was deducted. The Jadad scale score varied from 0 to 5 points. An article with Jadad score ≤ 2 was considered to be of low quality. If the Jadad score was ≥ 3, the study was thought to be of high quality (25). Two investigators independently assessed the quality of included studies. Any discrepancy should be solved by consensus.
Mean differences (MDs) with 95% confidence intervals (95% CIs) for continuous outcomes (WOMAC scores, pain scores at 2, 6 and 12 weeks) and risk ratios (RRs) with 95% CIs for dichotomous outcomes (pain on motion) were used to estimate the pooled effects. An I2 value greater than 50% indicates significant heterogeneity. The random-effects model with DerSimonian and Laird weights was used in all analyses. Sensitivity analysis was performed to detect the influence of a single study on the overall estimate via omitting 1 study in turn when necessary. Owing to the limited number (< 10) of included studies, publication bias was not assessed. p < 0.05 in 2-tailed tests was considered statistically significant. All statistical analyses were performed with Review Manager Version 5.3 (The Cochrane Collaboration, Software Update, Oxford, UK).
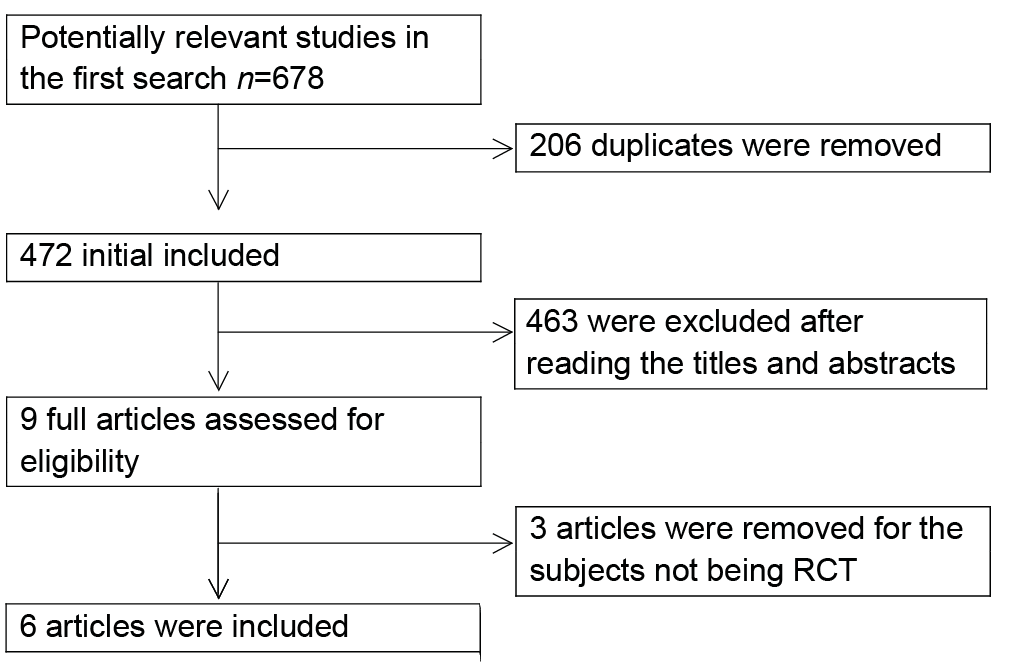
The flow chart for the selection process and detailed identification was presented in Fig. 1. A total of 678 publications were identified through the initial search of databases. Ultimately, 6 RCTs were included in the meta-analysis (18–21, 26, 27).
The baseline characteristics of the 6 eligible RCTs in the meta-analysis were summarized in Table I. The 6 studies were published between 2007 and 2012, and sample sizes ranged from 29 to 80, with a total of 310. There were similar characteristics between the hyaluronic acid group and the control group at baseline. One RCT reported knee arthroscopy for anterior cruciate ligament reconstruction (18), 2 RCTs reported knee arthroscopy for meniscus tear (26, 27), 2 RCTs reported arthroscopic debridement for knee osteoarthritis (19, 21), and 1 RCT reported arthroscopic knee joint lavage, or in combination with cartilage debridement (20).
Fig. 1. Flow diagram of study searching and selection process.
Among the 6 RCTs, 2 studies reported WOMAC scores (19, 21), 2 reported pain scores at 2 weeks (18, 20), 2 reported pain scores at 6 weeks (18, 21), 3 reported pain scores at 12 weeks (18, 21, 27), 2 reported pain on motion (20, 27). Jadad scores of the 6 included studies varied from 3 to 5, all 6 studies were considered to be high-quality ones according to quality assessment.
This outcome data was analysed with a random-effects model, the pooled estimate of the 2 included RCTs suggested that, compared with the control group after knee arthroscopy, hyaluronic acid injection was associated with significantly increased WOMAC scores (mean difference = 11.43; 95% CI = 1.39 to 21.47; p = 0.03), with no heterogeneity among the studies (I2 = 0%, heterogeneity p = 0.73) (Fig. 2).
Fig. 2. Forest plot for the meta-analysis of Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) scores.
No heterogeneity was observed among the included studies for the WOMAC scores. Thus, we did not perform sensitivity analysis by omitting 1 study in turn to detect the source of heterogeneity.
Compared with control intervention following knee arthroscopy, hyaluronic acid had no substantial impact on pain scores at 2 weeks (MD –0.16; 95% CI –0.81–0.49; p = 0.63; Fig. 3a), 6 weeks (MD 0.01; 95% CI –0.86–0.89; p = 0.98; Fig. 3b), or 12 weeks (MD –0.51; 95% CI –1.56–0.53; p=0.34; Fig. 3c), but resulted in significantly reduced pain on motion (RR 0.22; 95% CI 0.06–0.79; p = 0.02; Fig. 4).
Fig. 3. Forest plot for the meta-analysis of pain scores at (a) 2 weeks, (b) 6 weeks and (c) 12 weeks.
Fig. 4. Forest plot for the meta-analysis of pain on motion.
Pain management allowed early mobilization and rehabilitation following knee arthroscopy, and mainly included oral analgesics, femoral nerve block, and intra-articular injections (28–30). Continuous femoral nerve block was revealed to alleviate pain within 48 h, but had no influence on pain management and knee function (28, 31, 32). Intra-articular fentanyl/bupivacaine achieved comparable efficacy in relation to femoral nerve block in the first 24 h (33). Intra-articular injection of tenoxicam could reduce analgesic consumption in the first 3–6 h (34).
Exogenous hyaluronic acid was reported to stimulate de novo synthesis of hyaluronic acid, and inhibit the release of arachidonic acid and interleukin-1α-induced prostaglandin E2 synthesis, which reduced the anti-inflammatory response for pain control (35). One included RCT reported that hyaluronic acid treatment was capable of substantially alleviating pain and symptoms within 2 days after arthroscopic anterior cruciate ligament reconstruction (18). Another RCT also reported that statistically significant pain reduction was found 1 week postoperatively in arthroscopic surgery (26). In our meta-analysis, hyaluronic acid was revealed to significantly reduce pain on motion in knee arthroscopy, but had no influence on pain control 2, 6 and 12 weeks after the arthroscopic surgery. These results support the efficacy of hyaluronic acid treatment for pain control 1 week postoperatively when the inflammatory response after surgery is obvious.
Hyaluronic acid has been reported to result in a more rapid recovery from arthroscopic surgery, with less pain, less effusion, and a lower intake of analgesics (26). One RCT, involving 66 patients with various degrees of chondral damage, showed that post-arthroscopic instillation of hyaluronic acid-based synovial fluid substitute into the joint benefited long-term stabilization of treatment outcome 2 years after surgery (20). Another multicentre, prospective, open study showed that hyaluronic acid could provide effective pain relief, and improve stiffness and physical function at 4–12 weeks after arthroscopic meniscectomy in patients with knee osteoarthritis (36). The current meta-analysis also indicated that hyaluronic acid was associated with significantly increased physical function, as evidenced by the improved WOMAC scores. The incidence of postoperative swelling was reported to be significantly reduced after hyaluronic acid injection following knee arthroscopy (27).
Several study limitations should be taken into account. Firstly, our analysis was based on only 6 RCTs, all of which have a relatively small sample size (n < 100). Overestimation of the treatment effect was more likely in smaller trials compared with larger samples. The detailed methods of knee arthroscopy, and the variation in timing and volume of hyaluronate in the included studies were different. These factors may have an influence on the pooling results. Next, the duration and follow-up time of hyaluronic acid varied from 2 weeks to 2 years. Finally, it was necessary to compare therapeutic effects of hyaluronic acid with femoral nerve block, intra-articular opioids and anti-inflammatory drugs.
Hyaluronic acid treatment showed important abilities to reduce pain on motion in the short-term and to improve physical function in knee arthroscopy.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize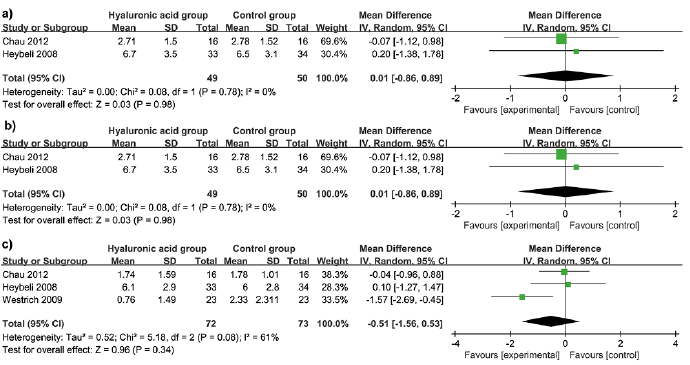 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize