
Objective: To review the evidence concerning the effects of postoperative exercise interventions on exercise capacity and health-related quality of life following resection for non-small cell lung cancer, and to review whether different initiation times of exercise produce different effects on exercise capacity.
Data sources: Comprehensive literature search of MEDLINE, Embase, CENTRAL, CINAHL and PEDro.
Study selection: Randomized controlled trials examining the effects of exercise interventions were eligible for inclusion.
Data extraction: Postoperative outcome measurements were extracted and the quality of evidence was graded using Grading of Recommendations Assessment, Development and Evaluation (GRADE) Working Group.
Data synthesis: Four randomized controlled trials were identified involving 262 participants. Short-term follow-up (12–20 weeks) showed significantly higher exercise capacity and physical component of health-related quality of life in the intervention group (standardized mean difference (SMD) 0.48; 95% confidence interval (CI) 0.04–0.93) compared with the control group (SMD 0.50; 95% CI 0.19–0.82). There was no difference between the effect of late- and early-initiated exercise intervention.
Conclusion: Exercise has a small-to-moderate effect at short-term follow-up on exercise capacity and the physical component of health-related quality of life in patients operated for lung cancer. The long-term effects of exercise capacity are unknown. Early-initiated exercise programmes (2 weeks post-operation) did not show an effect on exercise capacity. These findings should be interpreted with caution.
Key words: non-small cell lung cancer; exercise; health-related quality of life.
Accepted Oct 5, 2017; Epub ahead of print Jan 25, 2018
J Rehabil Med 2018; 50: 00–00
Correspondence address: Maja S. Sommer, Copenhagen Centre for Cancer and Health, City of Copenhagen, Norre Allé 45, DK-2200 Copenhagen, Denmark. E-mail: mss@kraeftcenter-kbh.dk; Maja E. B. Staerkind, University Hospitals Centre for Health Research (UCSF), Rigshospitalet, Blegdamsvej 9, DE-2100 Copenhagen, Denmark. E-mail: maja@bohlbro-staerkind.dk
Lung cancer is one of the most common malignancies worldwide, and the leading cause of cancer-related death (1). Pulmonary resection is currently the most effective curative treatment when non-small cell lung cancer (NSCLC), stage I, II, IIIA, is diagnosed. Surgery is performed using either an open approach (thoracotomy) or minimally invasive video-assisted thoracoscopic surgery (VATS) (2). Improvements in earlier preoperative staging, better surgical techniques and more effective adjuvant treatment have enhanced survival (3). Lung cancer surgery is associated with morbidity, functional limitations and decreased quality of life (4).
As a result, evidence-based rehabilitation may be a key component to improve outcome and quality of life in these patients (4, 5). An emerging discipline in rehabilitation of lung cancer survivors, exercise intervention, is associated with benefits that may improve the health of long-term cancer survivors and extend survival (6).
Studies demonstrate lower levels of physical activity among individuals diagnosed with NSCLC compared with healthy individuals, yet the physical activity level decreases further during the first 6 months following diagnosis (7).
The increase in population of lung cancer survivors signifies the need to improve their health. Barriers for participating in rehabilitation and maintaining lifestyle changes are, for example, high symptom burden, such as side-effects to the adjuvant treatment, and high prevalence of comorbidity, especially chronic obstructive pulmonary disease (COPD) (8).
Exercise initiated early in the treatment trajectory is found to be beneficial for operable lung cancer patients (9, 10). In a population diagnosed with myocardial infarction, early-initiated exercise in the acute phase has shown greater benefits on exercise capacity than is the case in exercise interventions initiated in a later treatment phase (11).
Systematic reviews investigating the effects of pre- and post-surgical exercise interventions in patients with NSCLC show that exercise may increase exercise capacity of people following lung resection for NSCLC (6, 12, 13). However, to date, no systematic reviews have been done investigating the effects of post-surgical exercise interventions for patients with NSCLC focusing on high-quality evidence and only post-operative outcomes to eliminate the impact of the surgery (no pre-operative baseline measurements).
Furthermore, no previous reviews have focused on whether the effect would differ due to different initiation times for postoperative exercise in patients with NSCLC. The present review hypothesized that early initiation of exercise (within 2 weeks) following lung resection for NSCLC would increase the effect on exercise capacity compared with later initiation of exercise.
The primary objective was to systematically review the literature for the effect of postoperative exercise interventions on exercise capacity in patients following lung resection for NSCLC. A secondary aim was to review the effect of exercise interventions on health-related quality of life (HRQoL) and to determine whether different initiation times of exercise either enhanced or decreased exercise capacity in patients following lung resection.
The protocol for this systematic review was registered in the PROSPERO database (registration number CRD42016027412). The Cochrane Handbook for Systematic Reviews of Interventions (14) and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement guidelines (15) were applied during preparation of this review.
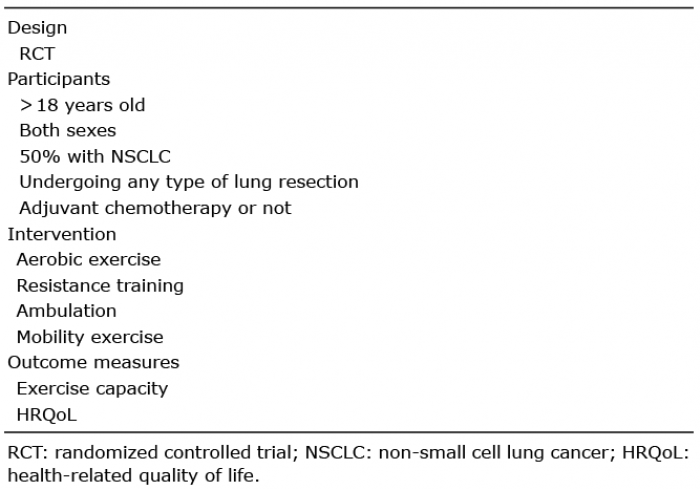
Randomized controlled trials (RCT) assessing the effects of postoperative exercise interventions in patients undergoing resection for NSCLC, in which participants were allocated to receive exercise compared with a control group, were included. Studies and abstracts published in English, one of the Scandinavian languages, or German were eligible for inclusion. Inclusion criteria were trials with participants receiving any type of lung resection performed with VATS or thoracotomy procedures. To avoid comparison of effect measures in different populations, trials were included only if at least 50% of the population had resectable NSCLC. Trials were included if the interventions comprised any type of exercise involving bodily movements produced by skeletal muscles (aerobic exercise, resistance exercise, ambulation or mobility exercise) initiated within 1 year after lung resection.
Supervised and/or unsupervised exercise performed individually or in groups were also eligible intervention criteria. Type, intensity, frequency and duration of the exercise interventions were not a constraint, but were recorded where possible. Control groups were considered eligible if they contained non-intervention control, usual care, waiting list control or add-on treatments.
VO2peak is considered the gold standard for the measurement of cardiorespiratory fitness and 6MWD is often used in pulmonary rehabilitation programmes to quantify exercise capacity, both recommended for use in clinical oncology research (16–19). The primary outcome of the present review was any measure of maximum exercise capacity (16). Exercise capacity measures included peak oxygen consumption (VO2peak) and 6-minute walk distance (6MWD), measured as primary or secondary outcomes in the included studies.
The secondary outcome of interest was HRQoL assessed by 1 of the 3 most commonly used questionnaires for thoracic surgery patients: Generic 36-Item Short Form Health Survey (SF-36) (20), cancer-specific European Organization for Research and Treatment of Cancer Quality of Life Questionnaire (EORTC QLQ C-30) (21), and the disease-specific patient-reported outcome Functional Assessment of Cancer Therapy-Lung (FACT-L) (22). The European Society of Thoracic Surgeons defines these questionnaires as the most appropriate for thoracic surgery patients.
Only postoperative outcome measurements were extracted, in order to examine the effect of postoperative exercise eliminating the impact of surgery and to compare effect sizes across studies. The inclusion criteria are summarized in Table I.
Table I. Inclusion criteria
A Comprehensive literature search of MEDLINE, Embase, CENTRAL, CINAHL and PEDro. The literature search matrix used for MEDLINE (shown in Appendix SI1) was adapted for use in the other databases (search strategies shown in Appendix SV1). The Search strategy focused on 2 overall clusters: NSCLC and rehabilitation, with their associated synonyms, combined with AND, as shown in Appendix SI1. No limitations were used in the electronic searches to avoid unintended exclusion of relevant trials.
In order to identify additional trials all reference lists of all primary studies and review articles were screened. Experts in the field of exercise and NSCLC were contacted in order to identify unpublished research. A search was also carried out of clinicaltrials.gov to identify ongoing, as yet unpublished, trials.
All references identified were imported into the web-based software platform covidence.org. Selection of trials, risk of bias assessment, and extraction of data were managed with this software. Two review authors (MB, MS) independently screened titles and abstracts, after which full-text screening was undertaken using the search strategy to determine eligibility for inclusion. Their decisions were recorded and disagreements were resolved by consensus.
Two review authors (MB, MS) independently extracted data using a predefined form based on the Cochrane Collaboration’s checklist of items to consider in data extraction (14). Data included details of the trials, participant characteristics and results at postoperative time points. Disagreements on extraction of data were resolved by discussion.
Two review authors (MB, MS) independently assessed the risk of bias of all included trials, evaluated as either high, low or unclear risk of bias using the Cochrane Collaboration’s tool for assessing risk of bias (14). High risk of bias indicated that there was a high risk that the results would either overestimate or underestimate the true intervention effect, while low risk of bias indicated the opposite. Unclear risk of bias denoted either a lack of information or uncertainty concerning the potential of bias. Disagreements were resolved by discussion, or when necessary, a third review author (JC) was consulted and agreement reached.
For continuous outcomes standardized mean differences (SMD) and the corresponding 95% confidence intervals (95% CI) were used in the analysis. To calculate the SMDs the mean change scores and the corresponding standard deviations (SDs) were extracted from the included trials when these were reported. Where mean change scores and/or SDs of the mean change scores were not applied, they were calculated based on the baseline and follow-up means and SDs, as recommended in the Cochrane Handbook (14). The calculated SDs of the mean change scores from baseline were estimated by imputing a correlation coefficient in the formula below to allow the use of paired data (23, 24):
Correlation coefficients were used in the calculation of SDs of mean change scores in the following outcomes: VO2peak r = 0.927 (25), 6MWD r = 0.93 (19), SF-36 physical and mental component scores (26) and EORTC QLQ-C30 physical functioning score r = 0.85 (27).
If there was any discrepancy between the reported mean change scores and the stated baseline, and follow-up data were identified in an article, the mean change scores were also calculated based on the above-mentioned formula.
Cohen’s guidelines for interpreting the magnitude of SMD were followed: small SMD = 0.2; medium SMD = 0.5; and large SMD = 0.8 (28).
Authors of the reviewed trials were contacted to provide details of missing data. If the trial authors could not provide the requested information or were unable to comply with the request within 1 month, the review process continued without the information. When baseline and/or follow-up means and SDs were not published, the authors were contacted. Missing individuals from the reported results were recorded, where possible, and results from intention-to-treat analyses were prioritized in the analysis of this review.
Clinical heterogeneity was evaluated by examining diversity in patient populations (e.g. age, resection degree, and comorbidities) and exercise interventions (e.g. type, intensity, frequency, duration) among the trials. In addition, the percentage of the variability in effect estimates due to heterogeneity was evaluated using the I-squared test (I2), which is suitable in this review because it is independent of the numbers of studies. The interpretation of I2 is that a higher percentage indicates statistical heterogeneity, with tentative limits as “low” at 25%, “moderate” at 50% and “high” at 75%, considered substantial heterogeneity above 50% (29). A random-effects model, using the method of DerSimonian & Laird (30), was chosen if the clinical heterogeneity or I2 was evaluated to be high.
The follow-up closest to 12 weeks was designated as short-term and a long follow-up exceeding 6 months was designated as long-term.
A sensitivity analysis was conducted to assess the effect of trials initiating exercise interventions early (within the first 2 weeks after lung resection) compared with the effect of trials initiating exercise interventions later than 2 weeks after lung resection. This analysis was conducted on short-term outcomes. The 2-week time limit was a pragmatic approach based on clinical reflections on tissue healing and when stressing the operation wound by exercising would be safe. The purpose of this sensitivity analysis was to aid in identifying the optimal time-point to initiate postoperative rehabilitation after lung resection in patients with NSCLC. Since no evidence was available to guide this decision, a thoracic surgeon specialist made the assessment. Outcomes included in the “summary of findings” table were exercise capacity and HRQoL domains. Quality of evidence was assessed for each outcome by grading evidence according to the Grade of Recommendation, Assessment, Development and Evaluation Working Group (31).
Statistical analyses and forest plots were generated in StataCorp 2013, Stata Statistical Software: Release 13 (StataCorp LP, College Station, TX, USA). Risk of bias summary and graphs were generated with Review Manager software (RevMan), version 5.3, Copenhagen, Denmark: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014. The summary of findings listed in Table II was conducted with GRADEpro GDT (GRADEpro Guideline Development Tool software, McMaster University, 2015 (developed by Evidence Prime, Inc.)
Table II. Summary of findings for main comparisons
Electronic databases were searched on 17 February 2016 and resulted in a total of 6,191 hits: 1,641 from MEDLINE, 3,291 from Embase, 270 from the Cochrane Central Register of Controlled Trials (CENTRAL), 970 from CINAHL and 19 from PEDro. The number of duplicates was 1,661, resulting in 4,530 unique articles. Based on the title and abstract, 4,464 articles were excluded, resulting in 66 articles read in full text. Of these, 62 studies were excluded as they did not meet the inclusion criteria. The present review included 4 RCTs involving 262 participants (32–35). Three of the studies randomized the participants into 1 of 2 groups: an exercise intervention or a control group (32–34). The fourth study randomized the participants into 1 of 3 groups: exercise intervention 1, exercise intervention 2 or a control group (35).This study was divided into 2 studies in the analyses, in which each intervention group was compared with half the control group (14).
Twelve studies were in a language other than those listed in our criteria and 3 had missing data. The first of the last-mentioned studies was contacted, but it was unable to provide postoperative measurements of exercise capacity (36); the second was a conference article that was insufficient due to low completion of the intervention and a high number of missing data (37); and the third was unable to provide the missing data on exercise capacity and HRQoL (38). Fig. 1 presents a flowchart of the search process based on the PRISMA template (15). Details of the excluded references are shown in Appendix SII1.
Fig. 1. Study flow diagram. RCT: randomized controlled trial; NSCLC: non-small cell lung cancer.
The studies, based in the UK, Denmark, Belgium and Norway, were published in 2011–2015. Two of the studies conducted the interventions in a hospital setting after discharge (33, 35), while participants in one study exercised during admission with subsequent home training (32). In the fourth study the intervention was conducted in local fitness centres after discharge (34).
All 4 studies included mainly participants who had undergone lung resection for NSCLC. Both sexes
were included and the mean age was over 60 years in all study groups. The majority of the participants went through open surgery (range 77–96%), and the lung cancer stages were equally distributed between control and exercise groups, except in one study, where 4 participants with stage IV NSCLC were randomized to the control group and none to the exercise group. For a summary of included studies see Tables III and IV.
Table III. Characteristics of included studies and participants
Table IV. Characteristics of included exercise interventions
Exercise interventions included a component with aerobic exercise and resistance training, except for intervention 2 in the 3-armed RCT, which included exercise and whole-body vibration (35).
The intervention components varied in intensity, frequency and duration across studies. The intensity of the aerobic exercises, which consisted of either walking or biking, varied from 60% to 95% of maximum heart rate. The frequency of training varied from 1 session per week for 10 weeks (33) to 3 times a week for 12 (35) or 20 (34) weeks. The exercise interventions were initiated after 5 days (32), 3 weeks (33), 4–6 weeks (34) or within 8 weeks (35) following lung resection.
Baseline measurements in Arbane et al.’s study (32) were conducted pre-surgery, since the study initiated exercise pre-surgery until day 5 post-surgery. In order to rule-out variance due to operation outcomes we decided in the present study to use the first measurement on day 5 post-surgery as the “baseline” in the present review.
In addition, the results by Arbane et al. (32) showed no statistically or clinically effect of early exercise captured by the day 5 post-surgery measurement, even though the intervention group had a mean distance that was 28 m longer than the control group (measured at day 5 post-operatively). The minimal important difference in the 6MWD in patients with lung cancer is 42 m (39).
The control groups received usual care, consisting of a monthly telephone call from the research team, which provided education (32), 1 h of individual instruction in home exercises (33), no advice beyond general information from the hospitals (34) and even discouraged to improving their exercise tolerance with professional help (35).
Exercise capacity was reported in all 4 studies, 2 of which reported VO2peak (34, 35) and 3 of which reported 6MWD (32, 33, 35). HRQoL was reported in 3 studies, 2 of which reported SF-36 in physical- and mental component scores (33, 34), and 1 of which reported the physical functioning score of the EORTC QLQ-C30 (35). One study did only have one measurements of HRQoL post-surgery, which is why that outcome was not extracted (32). All of the studies had collected a short-term follow-up at completion of their interventions, and 1 study had collected an additional long-term follow-up 1 year after baseline (33).
The overall assessment of risk of bias across the studies is presented in Fig. 2, while the risk of bias for the individual studies is presented in Appendix SIII1.
Fig. 2. Risk of bias graph: review authors’ assessment of each risk of bias item presented as percentages across all included studies.
All of the studies reviewed were at high risk of performance bias because blinding of participants is difficult in exercise interventions. The majority of studies were at high or unclear risk of detection bias and reporting bias as the outcome assessors were not blinded and the relevant predefined outcomes were not evaluated due to lack of completion of outcome measures or no trial registry. The section called “Summary of included studies” in Appendix SIV1 contains a detailed description of the assessment of risk of bias.
All meta-analyses were conducted using a random-effects model after assessment of clinical heterogeneity between studies, especially in exercise interventions.
VO2peak is considered the gold standard measurement of cardiorespiratory fitness research, therefore when both measurements were available VO2peak was chosen. Results at completion of the intervention periods, stated as short-term, showed a significantly higher exercise capacity in the intervention group compared with the control group (SMD 0.48; 95% CI 0.04–0.93), reflecting a small-to-moderate effect size (Fig. 3). The I2 was 61.6%, suggesting moderate variations between intervention effects. The study with a long-term follow-up showed no effect on exercise capacity after 1 year from baseline (SMD 0.09; 95% CI –0.44 to 0.61), the results are not illustrated.
Fig. 3. Forest plot: effect of exercise capacity in exercise group vs control group (short term). SMD: standardized mean difference; 95% CI: 95% confidence interval.
The SF-36 physical component score was pooled in a meta-analysis with the EORTC QLQ-C30 physical functioning score. The physical component of HRQoL was significantly higher in the intervention group compared with the control group (SMD 0.50; 95% CI 0.19–0.82) in the short-term, reflecting a moderate effect size (Fig. 4). The I2 was 0%, suggesting a small variation between intervention effects.
Fig. 4. Forest plot: effect of the physical component of health-related quality of life (HRQoL) in exercise group vs control group (short term). SMD: standardized mean difference; 95% CI: 95% confidence interval.
According to the one study with long-term follow-up, there was no effect on the physical component of HRQoL in the long-term (SMD –0.27; 95% CI –0.78 to 0.25). The results are not illustrated in the present review. The SF-36 mental component score was reported in 2 studies and pooled in a meta-analysis. There was no effect on the mental component of HRQoL (SMD 0.53; 95% CI –0.78 to 1.83) in the short-term, nor at long-term follow-up (SMD –0.48; 95% CI –1.01 to 0.04). The results are not illustrated.
Only one study initiated exercise intervention early, within 2 weeks after surgery (32). This study showed no effect on exercise capacity in the short-term (SMD 0.09; 95% CI–0.57 to 0.74), as illustrated in Fig. 5. In 3 studies that initiated exercise interventions later (33–35), > 2 weeks after surgery, in contrast, the exercise capacity was significantly higher in the intervention group compared with the control group in the short-term (SMD 0.58; 95% CI 0.07–1.09), reflecting a moderate effect size (Fig. 5). There was no difference between effect of late and early initiated exercise intervention. The I2 for exercise interventions initiated late was 65.6%, suggesting moderate variation between intervention effects.
Fig. 5. Forest plot: early or late initiated exercise interventions in exercise group vs control group (short term). SMD: standardized mean difference; 95% CI: 95% confidence interval.
The main findings and quality of the body of evidence for each result is presented in the summary of findings (Table II).
This meta-analysis showed that exercise improved exercise capacity and the physical component of HRQoL in the short-term, but no beneficial effect was found on the mental component of HRQoL. Only one study evaluated the long-term effects and found no effect on either physical capacity or HRQoL (33). Early-initiated exercise programmes, within 2 weeks after lung resection, did not show an effect on exercise capacity. These findings must be interpreted with caution due to the heterogeneity of exercise programmes, methodological limitations, some significant risks of bias, small samples and the low number of studies included.
As exercise capacity appears to be a valuable prognostic indicator for patients with NSCLC, and the clinical finding that exercise capacity increases during exercise in patients following lung resection is highly important (40). Until now referral for rehabilitation following lung resection has been based on an individual evaluation of rehabilitation needs. Numbers of referrals made is unpublished, but a survey from Australia and New Zealand reports that < 25% of patients are referred to pulmonary rehabilitation after lung resection (41). The inadequate level of referrals is due to the lack of well-designed studies to confirm the role of supervised exercise training in facilitating postoperative recovery in this patient population (41).
The large variations in the exercise programmes, in terms of moderate-to-high intensity ranging from 60% to 90% of heart rate maximum (HRmax), frequency ranging from twice a day to 3 times a week, and duration from 5 min per exercise to a 60-min full session, influence the findings in the present review and limit the clinical applicability.
Differences in physical activity recommendations across the control groups may have influenced the effect sizes. Potential contamination of exercise in some of the control groups may have influenced, and most likely reduced, the effect of the relevant studies.
The present review did not clarify whether early initiation of exercise, within 2 weeks following lung resection, is more effective than exercise initiated later, which was hypothesized a priori. One study initiated exercise intervention within 2 weeks following surgery and therefore this analysis may not illustrate the true effect. Thus, the study contained a home-based non-supervised training programme following discharge, which potentially could have lowered adherence to the intervention, reducing its effect (32).
As a result it is not possible to evaluate whether early-initiated exercise training will improve the effect in exercise capacity and HRQoL.
The recruitment rates were low in 2 out of 6 studies (33, 35), potentially having caused a selected group of participants, e.g. the healthiest, the youngest and the fittest, to participate compared with those uninterested. Characteristics of the populations in the studies are therefore not necessarily consistent with a representative sample of patients with operable NSCLC. Information about eligible patients not interested in participating would be of great clinical interest with regard to applicability.
The quality of evidence provided by the studies included in the analysis has been rated, according to GRADE, as low or very low, mainly because of some serious risks of bias, inconsistency in effect estimates and imprecision, as the small sample sizes caused wide confidence intervals. Consequently, the results must be interpreted with caution.
A strength of this review is the comprehensive literature search by 2 review authors, which optimized sufficient identification of relevant studies, and successfully obtaining missing data.
In addition, the investigative work done to find ongoing, unpublished studies by searching trial registrations and contacting recognized authors in the research field improves the probability that all relevant studies were found. The number of studies excluded due to the language criteria, however, probably limited the inclusion of further studies. The 3 studies excluded due to missing data also represent a limitation, as their effect estimates could have influenced the results of this review.
One of the excluded studies found that 6MWD improved by 35 m from preoperative baseline to post-intervention, the control group showed a decline by 59 m (p = 0.024) (38). Another study found no differences between the intervention group (homebased exercise plus 5 days with exercise in hospital) and the control group (36). What the 2 studies have in common is no post-operative baseline-outcomes to eliminate the impact of surgery; therefore it is difficult to compare the results with the results of this review.
The excluded study by Jacobsen et al. was a conference article that did not report any results (37).
If the pooled data from the various instruments (VO2peak and 6MWD) used to assess exercise capacity did not measure the same outcomes, the results of the review may be biased. A recent study shows a difference in pulmonary oxygen when comparing 6MWD and the cardiopulmonary exercise test in patients with NSCLC following lung resection (17).
Studies on patients diagnosed with either chronic obstructive pulmonary disease or chronic heart failure, in contrast, found no differences in VO2peak obtained using either the pulmonary oxygen uptake test or the 6MWD (42–44).
Including the most commonly used and recommended questionnaires for measuring HRQoL in thoracic surgery patients could represent a strength as well as a limitation. The decision was made to maintain a high level of methodological quality, which is why the 3 questionnaires listed were considered useful for the population, though SF-36 has not been validated for patients with lung cancer. A limitation is the pooled data from the physical component domain of HRQoL, since it was assessed using instruments with different target groups, as one was a generic HRQoL questionnaire (SF-36) and the other a cancer-specific HRQoL questionnaire (EORTC QLQ-C30).
The EORTC QLQ-C30 physical functioning domain has shown a substantial convergent correlation with all of the 4 SF-36 physical summary component subdomains (r > 0.50) (45). The moderate similarity of the 2 instruments may have biased the result of the physical component of HRQoL, presenting the risk of an overestimate or underestimate of real effect.
The use of imported correlation coefficients in the calculation of SDs of mean differences in 2 of the included studies may have had an impact on the results. These SDs are estimates calculated based on changes found in previous studies with similar populations of patients with other cancer diagnoses (26). The SF-36 scores in that study were also reported to be similar to SF-36 scores for patients with chronic diseases, such as chronic obstructive pulmonary disease, hypertension and congestive heart failure (26). This method of estimating the SDs could decrease the reliability of the reported results, due to an element of imprecision in the estimates (14). However, the estimated SD becomes a better replacement of the real SD compared with the use of an unpaired SD of the mean change.
A significant improvement in 6MWD was confirmed in a previous systematic review evaluating the effect of exercise interventions in patients with NSCLC following lung resection (12). In contrast baseline outcome measures from pre- and post-surgery were included where the present review has all outcome measures conducted post-surgery to eliminate the impact of lung surgery and focus entirely on the effect of rehabilitation. In addition, the present review included 2 new RCTs with a total of 131 participants. Other previous systematic reviews confirmed that both pre- and post-operative exercise was associated with positive benefits on exercise capacity and some domains of HRQoL (6, 46). Different study designs were included in the previous reviews, including a few RCTs, only one of which met the inclusion criteria of the current review (32).
During completion of the current review, a new review by Ni et al. (13) (evaluating the effects of pre- and post-operative exercise interventions) was published supporting our findings, in contrast their review included all study designs, as well as pre- and post-operative measurements.
The present review does not find that exercise improves the mental domain of HRQoL compared with usual care for patients having undergone lung resection; however, there might be a trend towards the direction of positive effects, but the confidence intervals indicate that these effects are very uncertain. The findings are in contrast to previous research in patients with COPD, patients with other cancer diseases and qualitative research in patients undergoing lung resection for NSCLC (9). One of the possible reasons for this is how HRQoL was assessed, as SF-36 is a generic HRQoL questionnaire, or the lack of statistical power in the studies in the present review.
This review is the first to examine the effects of postoperative exercise training in patients with NSCLC following lung resection with inclusion of postoperative outcome measurements alone. This method does not include the involvement of the surgery on the outcomes. Inclusion of solely RCTs improves the quality of evidence. Moreover, this review is the first to focus on the effects of early-initiated exercise, although, due to lack of studies, this analysis did not lead to any conclusion regarding this question.
This review found that exercise may have beneficial effects on exercise capacity and the physical component of HRQoL among patients following lung resection for NSCLC. However, since there are risks of bias, inconsistency and imprecision of findings, these results should be interpreted with caution.
Despite the overall low quality of the body of evidence, health professionals should consider referring patients with NSCLC to an exercise programme following lung resection. Further research is needed to confirm the efficacy of exercise intervention in people with NSCLC, and whether these effects can be maintained beyond the active intervention period. Additional research is required to investigate when exercise intervention should be initiated following lung resection to obtain the best result and prevent or minimize postoperative impairments. This knowledge may contribute to the design of future exercise research in patients with operable NSCLC.
This review is supported by grants from the Center for Integrated Rehabilitation of Cancer Patients (CIRE), which is supported by the Danish Cancer Society and the Novo Nordisk Foundation. Funding has also been provided by Rigshospitalet, University of Copenhagen; the Faculty of Health and Medical Sciences, University of Copenhagen; and the City of Copenhagen. CopenRehab is supported by a grant from the City of Copenhagen.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize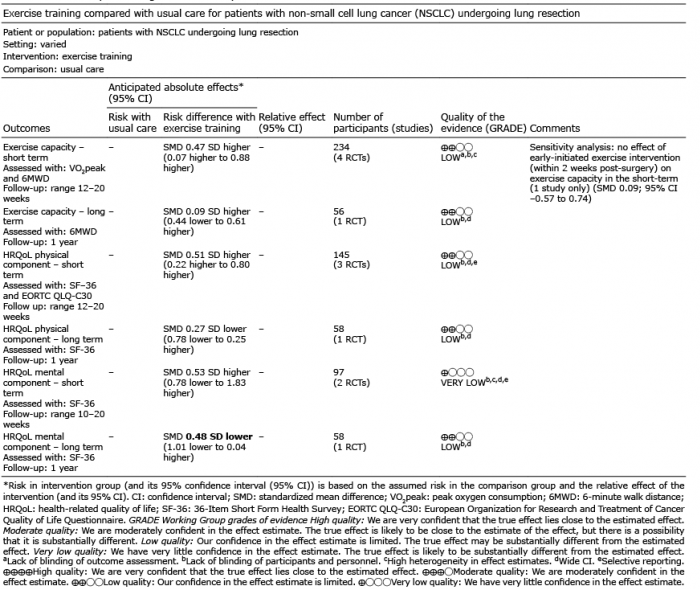 Click to show fullsize
Click to show fullsize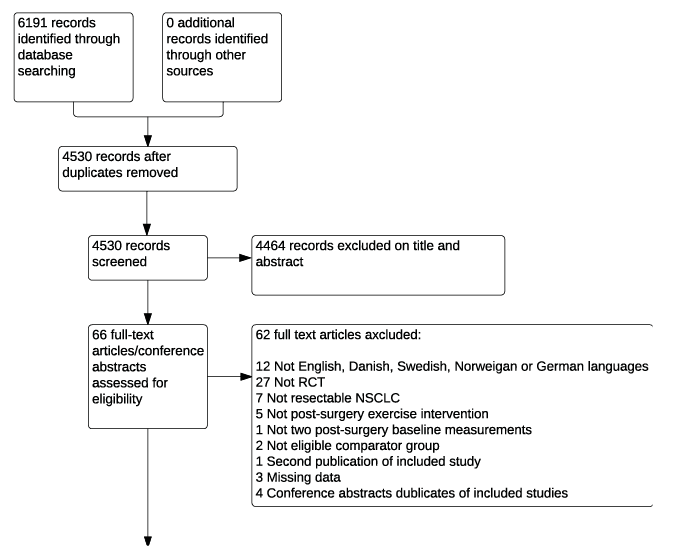 Click to show fullsize
Click to show fullsize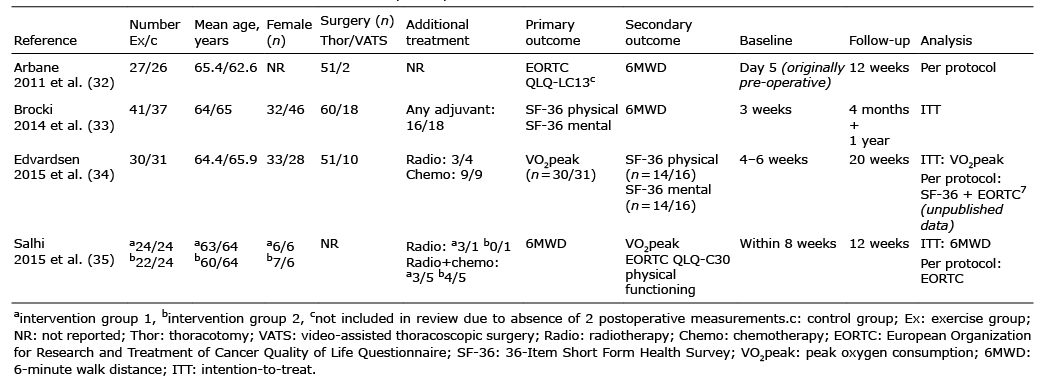 Click to show fullsize
Click to show fullsize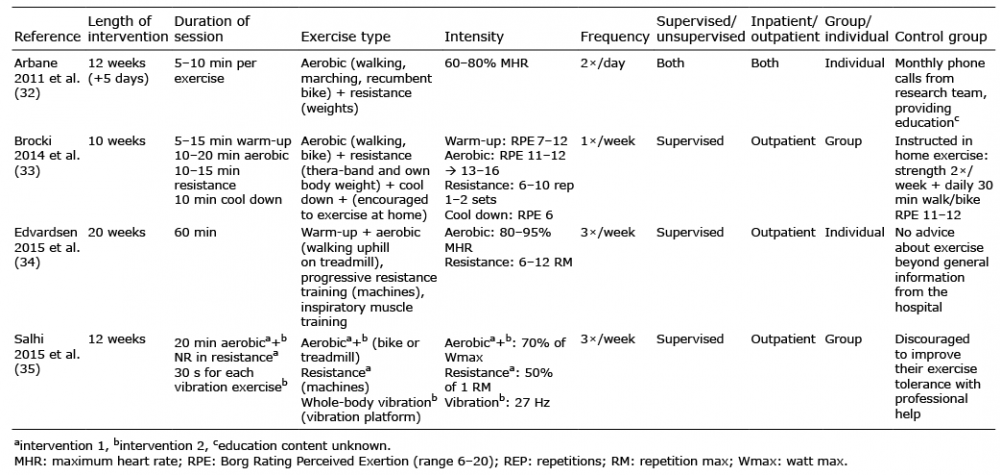 Click to show fullsize
Click to show fullsize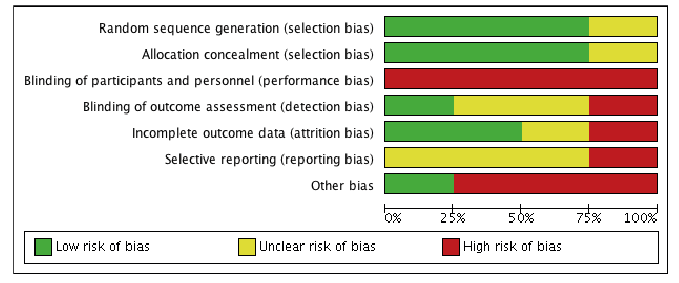 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize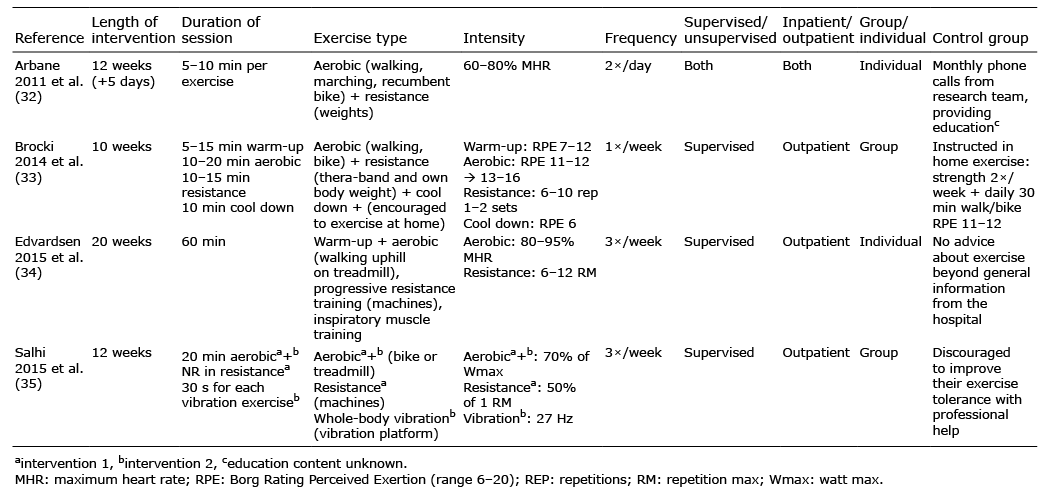 Click to show fullsize
Click to show fullsize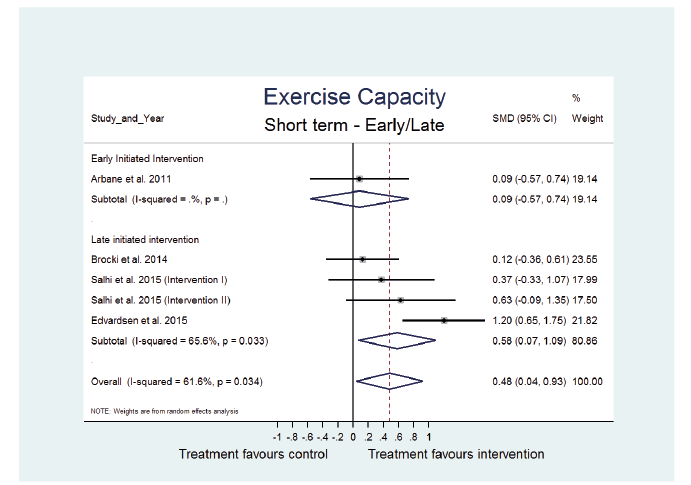 Click to show fullsize
Click to show fullsize