
From the Department of Rehabilitation Medicine, Shanghai First People’s Hospital, Shanghai Jiao Tong University, Shanghai 200080, China
Objective: To evaluate the effectiveness and safety of transcranial direct current stimulation for fibro-myalgia.
Methods: Databases, conference records and registered trials were searched for articles published from the date of establishment of the database
through to October 2015. Six randomized controlled trials (n=192) of transcranial direct current stimulation for fibromyalgia were included in the current study.
Data extraction: Two researchers independently screened the literature, assessed methodological quality using the Cochrane Collaboration’s tool, and extracted data.
Data synthesis: Studies were divided into 3 groups for meta-analysis according to stimulation site and polarity. Significant improvement in pain and general fibromyalgia-related function was seen with anodal transcranial direct current stimulation over the primary motor cortex (p<0.05). However, the pressure pain threshold did not improve (p>0.05). Anodal transcranial direct current stimulation over the left dorsolateral prefrontal cortex did not significantly reduce pain or improve general fibromyalgia-related function compared with sham stimulation (p>0.05). Cathodal transcranial direct current stimulation over the primary motor cortex did not improve the pressure pain threshold compared with sham stimulation (p>0.05). No significant adverse effects were seen.
Conclusion: Anodal transcranial direct current stimulation over the primary motor cortex is more likely than sham transcranial direct current stimulation to relieve pain and improve general fibromyalgia-related function.
Key words: transcranial direct current stimulation; fibro-myalgia; meta-analysis.
Accepted Oct 7, 2016; Epub ahead of print Dec 16, 2016
J Rehabil Med 2017; 49: 2–9
Correspondence address: Wen-hua Chen, Department of Rehabilitation Medicine, Shanghai First People’s Hospital, Shanghai Jiao Tong University, Shanghai 200080, China. E-mail: wenhuachen@live.cn
Fibromyalgia is a systemic disease of unknown
aetiology (1). Its main symptoms are extensive physical pain and discomfort. Fibromyalgia is common in the clinical setting, with a reported prevalence of 2–5% and a higher incidence in women (2, 3). Although its pathogenesis is unclear, many physicians believe that fibromyalgia is a chronic pain syndrome caused by dysfunction of the central nervous system responsible for regulating sensory inputs (4, 5).
Several factors support fibromyalgia being related to central dysfunction. Regional cerebral blood flow is reduced in patients with fibromyalgia (6), and some centrally acting drugs can improve fibromyalgia (7). Neuroimaging (8) and electroencephalographic (9, 10) evidence also support this hypothesis. The best treatment for fibromyalgia is debated (11). Current evidence suggests that small doses of tricyclic antidepressants, cardiovascular exercise, cognitive behavioural therapy, and patient education are effective (1); however, the efficacy of treatment is often unsatisfactory (11). Therefore, there is an urgent need for a new and effective clinical intervention for fibromyalgia.
Several invasive and non-invasive stimulation techniques that can modulate the activity of the cortical neurones are being investigated to treat chronic pain syndrome (3). Transcranial direct current stimulation (tDCS), a non-invasive cranial stimulation technique that can modulate cortical excitability (12), has attracted widespread attention, as it is safe and easy to perform (13). The process can be blinded in both participants and evaluators, making it appropriate for investigation through randomized trials (13). Transcranial direct current stimulation has been studied widely with regard to rehabilitation from stroke (14, 15), mental illness (16, 17) and pain (18). A meta-analysis has shown that tDCS induces a significant analgesic effect in neuropathic pain after spinal cord injury (19). Transcranial direct current stimulation over M1 could relieve pain by regulating the hypothalamic suppression network and the intervening cortical and subcortical synaptic connections (20). Since fibromyalgia is a form of chronic pain syndrome in which dysfunction of the central nervous system has been implicated (4, 5), tDCS could theoretically be useful in relieving the condition. Marlow et al. (21) previously reviewed studies on tDCS for the treatment of fibromyalgia. A systematic review and meta-analysis reported that anodal tDCS over the motor cortex could relieve chronic pain (22). However, to the best of our knowledge, there has been no meta-analysis to assess the efficacy and safety of transcranial direct current stimulation in patients with fibromyalgia. Randomized controlled trials were included in the study, and anodal/cathodal transcranial direct current stimulation was compared with sham stimulation to evaluate the efficacy and safety of anodal/cathodal transcranial direct current stimulation in patients with fibromyalgia. The outcomes included pain, Fibromyalgia Impact Questionnaire, pressure pain threshold, and adverse events.
Databases, conference records, and registered trials were searched for articles published from the establishment of the database through October 2015. The databases included the Cochrane Library, JBI Database of Systematic Reviews, PubMed, ISI Web of Knowledge, Science-Direct, and Embase. A detailed list of search terms is provided in Appendix SI.
Inclusion criteria were: (i) randomized controlled trial; (ii) diagnostic criteria for fibromyalgia based on the criteria of the American College of Rheumatology (1990 OR 2010 ACR) (23, 24); (iii) experimental groups accepted tDCS alone or tDCS combined with other interventions for fibromyalgia; and (iv) control groups accepted sham tDCS alone or sham tDCS combined with other interventions for fibromyalgia. Exclusion criteria were: (i) non-randomized controlled trial or randomized controlled crossover trial; (ii) patients not meeting ACR criteria for fibromyalgia; (iii) data errors; (iv) animal experiment; (v) articles reporting on already published study populations.
Two researchers (YB, ZW) screened the literature independently in accordance with the inclusion and exclusion criteria, and extracted data. Disagreements were resolved through consultation or discussion with a third person (QQ). The literature was extracted as follows:
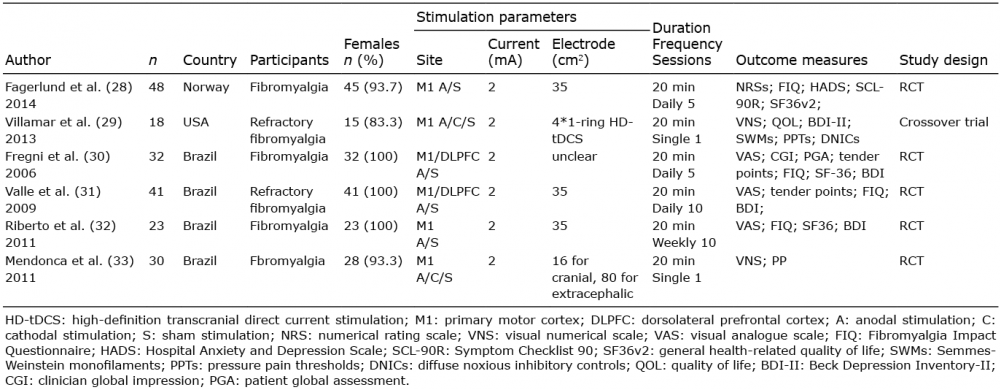
Table I. Basic characteristics of the included trials
Two researchers (QQ, MY) independently used the Cochrane Collaboration’s tool for assessing risk of bias as low, unclear or high (25). Disagreements were resolved by consultation or discussion with a third researcher (CWH). If the necessary information was missing, an attempt was made to contact the authors.
For all continuous variables, standardized mean difference (SMD) with 95% confidence interval (CI) was used to estimate the summary effect size (SES). Effect sizes were classified as small (<0.2), medium (0.2–0.8) or large (> 0.8) (26). Sensitivity analysis was performed to confirm the stability of the results.
RevMan 5.0 software (RevMan, The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, 2008), provided by the Cochrane Collaboration, was used for data analysis. I2 statistics were used for all comparisons to quantify heterogeneity (27). If p > 0.05 and I2 ≤ 50%, a fixed-effects model was chosen. If p ≤ 0.05 and I2 > 50%, a random-effects model was chosen (2).
A total of 475 studies were obtained on preliminary searching of the literature, of which 6 studies (n = 192; 184 female) (28–33) met the inclusion criteria. The inclusion and exclusion process is shown in Fig. 1. The differences in the basic characteristics of the included studies are outlined in Table I. Details of the risk of bias within studies are shown in Fig. 2.
Fig. 1. Literature screening process.
Fig. 2. Risk-of-bias summary. The authors’ judgments about each risk-of-bias item for each of the included trials.
Anodal tDCS over M1 vs sham tDCS. This analysis included 6 trials (28–33) with a total of 168 participants, of whom 84 were assigned to the anodal group and 84 to the sham group. With little statistical heterogeneity (χ2 = 6.66, p = 0.25, I2 = 25%), the overall effects was calculated with a fixed-effects model. Anodal tDCS over M1 was more likely to control pain than sham tDCS. The pooled SMD for pain was –0.59 (95% CI: –0.90 to –0.27) (Fig. 3A). The difference was statistically significant (Z = 3.66, p = 0.0002).
Fig. 3. Summary effect size for relieving pain. (A) Pain scores for anodal transcranial direct current stimulation (tDCS) over M1 compared with sham tDCS, as analysed with the fixed-effects model. (B) Pain scores for cathodal tDCS over M1 compared with sham tDCS, as analysed with the fixed-effects model. (C) Pain scores for anodal tDCS over the left dorsolateral prefrontal cortex (DLPFC) compared with sham tDCS, as analysed with the fixed-effects model. M1: primary motor cortex; SD: standard deviation; 95% CI: 95% confidence interval; Std. mean difference: standard mean difference; IV: inverse variance.
Cathodal tDCS over M1 vs sham tDCS. This analysis included 2 trials (29, 33) with a total of 48 participants, of whom 24 were assigned to the cathodal group and 24 to the sham group. With no statistical heterogeneity (χ2 = 0.78, p = 0.38, I2 = 0%), the overall effects was calculated with a fixed-effects model. Cathodal tDCS over M1 did not significantly relieve pain compared with sham tDCS. The pooled SMD for pain was –0.17 (95% CI:–0.74 to 0.40) (Fig. 3B), and the difference was not statistically significant (p > 0.05).
Anodal tDCS over the left dorsolateral prefrontal cortex (DLPFC) vs sham tDCS. This analysis included 2 trials (30, 31) with a total of 48 participants, of whom 24 were assigned to the anodal group and 24 to the sham group. With little statistical heterogeneity (χ2 = 1.27, p = 0.26, I2 = 21%), the overall effects was calculated with a fixed-effects model. Anodal tDCS over the left DLPFC did not relieve pain compared with sham tDCS. The pooled SMD for pain was –0.32 (95% CI: –0.89 to 0.26) (Fig. 3C), with no statistically significant difference (Z = 1.08, p = 0.28).
Anodal tDCS over cortex-M1 vs sham tDCS. This analysis included 4 trials (28, 30–32) with a total of 120 participants, of whom 60 were assigned to the anodal group and 60 to the sham group. With no statistical heterogeneity (χ2 = 1.04, p = 0.79, I2 = 0%), the overall effects was calculated with a fixed-effects model. Anodal tDCS over M1 was more likely to improve general fibromyalgia-related function than sham tDCS. The pooled SMD for the Fibromyalgia Impact Questionnaire (FIQ) was –0.66 (95% CI: –1.03 to –0.29) (Fig. 4A). The difference was statistically significant (Z = 3.48, p = 0.0005).
Fig. 4. Summary effect sizes for functional improvement. (A) Fibromyalgia Impact Questionnaire scores for anodal transcranial direct current stimulation (tDCS) over M1 compared with sham tDCS, as analysed with the fixed-effects model. (B) Fibromyalgia Impact Questionnaire scores for anodal tDCS over the left dorsolateral prefrontal cortex (DLPFC) compared with sham tDCS, as analysed with the fixed-effects model. M1: primary motor cortex; SD: standard deviation; 95% CI: 95% confidence interval; Std. mean difference: standard mean difference; IV: inverse variance.a
Anodal tDCS over left DLPFC vs sham tDCS. This analysis included 2 trials (30, 31) with a total of 48 participants, of whom 24 were assigned to the anodal group and 24 to the sham group. With no statistical heterogeneity (χ2 = 0.45, p = 0.50, I2 = 0%), the overall effects was calculated with a fixed-effects model. The pooled SMD for the FIQ was –0.22 (95% CI: –0.79 to 0.35) (Fig. 4B), with no statistically significant difference (Z = 0.76, p = 0.45).
Fig. 5. Summary effect size for pressure pain threshold improvement. (A) Pressure pain threshold scores for anodal transcranial direct current stimulation (tDCS) over M1 compared with sham tDCS, as analysed with the fixed-effects model. (B) Pressure pain threshold scores for cathodal tDCS over M1 compared with sham tDCS, as analysed with the fixed-effects model. M1: primary motor cortex; SD: standard deviation; 95% CI: 95% confidence interval; Std. mean difference: standard mean difference; IV: inverse variance.
Anodal tDCS over M1 vs sham tDCS. This analysis included 2 trials (29, 33) with a total of 24 participants, of whom 24 were assigned to the anodal group and 24 to the sham group. With no statistical heterogeneity (χ2 = 0.13, p = 0.71, I2 = 0%), the overall effects was calculated with a fixed-effects model. Anodal tDCS over M1 did not significantly improve the pressure pain threshold compared with sham tDCS. The pooled SMD for the pressure pain threshold was –0.07 (95% CI: –0.64 to 0.49) (Fig. 5A), with no statistically significant difference (Z = 0.25, p = 0.8).
Cathodal tDCS over left DLPFC vs sham tDCS. This analysis included 2 trials (29, 33) with a total of 30 participants, of whom 24 were assigned to the anodal group and 24 to the sham group. With no statistical heterogeneity (χ2 = 0.65, p = 0.42, I2 = 0%), the overall effects was calculated with a fixed-effects model. Anodal tDCS over M1 did not significantly improve the pressure pain threshold compared with sham tDCS. The pooled SMD for the pressure pain threshold was 0.11 (95% CI: –0.46 to 0.68) (Fig. 5B), with no statistically significant difference (Z = 0.38, p = 0.7).
Although attempts were made to obtain data from the follow-up periods by extracting the data and contacting the authors, it was not possible to calculate the overall effects of tDCS on fibromyalgia during the follow-up period, which limits the value of the whole analysis. Valle et al. (31) suggested that 10 sessions of anodal tDCS over M1 were more likely to control pain and improve general fibromyalgia-related function in patients with fibromyalgia, and the effect lasted for up to 2 months after the end of treatment. The effect of 10 sessions lasted longer than the effect of 5 sessions (31). Fagerlund et al. (28) showed pain reduction by tDCS 30 days after the last stimulation.
In the included studies, 1 participant did not receive an intervention, 1 refused to continue with the intervention because she had symptoms of depression and therefore declined to answer the questionnaire, and 1 participant dropped out without explanation. The rates of drop out between the active and sham groups were 3/144 and 2/84 respectively, with no statistically significant difference (p > 0.05). The most common side-effects were tingling and itching, which vanished within a few minutes. No participants experienced serious discomfort or cognitive impairment (29).
When the fixed-effects model and random-effects model were exchanged, the outcomes did not change significantly, which indicated high stability of the meta-analysis (34). When excluding the only study (29) that used 4*1-ring high-definition transcranial direct current stimulation (HD-tDCS) and which had the smallest sample size, the direction of the outcome did not change, but the heterogeneity increased (SMD for pain was –0.59 (95% CI: –0.94 to –0.23), I2 = 40%) (Fig. 6).
Fig. 6. Sensitivity analysis excluding data from the study that used high-definition transcranial direct current stimulation (HD-tDCS).
Funnel plots did not appear to be asymmetrical, which suggests a low risk of publication bias in the analysis of pain and FIQ (Fig. 7). To minimize any oversight of related publications, 2 researchers (YB, ZW) screened the literature independently. In addition, the databases, conference records, and registered trials were searched for articles and the search field was expanded by including free words and keywords. However, this meta-analysis may be subject to publication bias because studies with negative results are less likely to be published, therefore resulting in an overestimation of effect.
Fig. 7. Funnel plots for assessment of publication bias in (A) pain and (B) Fibromyalgia Impact Questionnaire (FIQ)
This meta-analysis found that anodal tDCS over M1 might relieve pain and improve general fibromyalgia-related function, but does not significantly increase the pressure pain threshold. These findings address a similar question using similar approaches as a previous systematic review and meta-analysis of 4 trials on chronic pain, which found a pooled effect size of 2.29 with a 95% CI of 3.5–1.08. The meta-analysis combined data concerning different types of chronic pain, including fibromyalgia, pain due to spinal cord injury, and pain due to multiple sclerosis (22).
Anodal tDCS is thought to increase cortical excitability, while cathodal stimulation decreases it (35). Anodal tDCS over the motor cortex has been used to manage several chronic pain conditions (36). However, the direction of modulation depends on the state of the underlying network, and pain networks may be altered (29). Antal & Paulus (37) reported that cathodal tDCS produced a significant analgesic effect in orofacial pain, and Knotkova et al. (38) found that it was effective in treating complex regional pain syndrome. The current meta-analysis did not support this analgesic effect. However, these results should still be considered, because the 2 included studies (29, 33) both carried out a single session of cathodal tDCS, and the short-term effects cannot be compared directly with these longer-term studies.
In the meta-analysis of anodal tDCS over the left DLPFC, 1 of the 2 included studies, which carried out 5 consecutive sessions, showed that tDCS was no more likely to control pain than sham tDCS (30). However, the other included study, which comprised 10 sessions, reached completely different conclusions (31). Therefore, the current meta-analysis might have a potential bias because of the different number of sessions performed across studies. However, there was not an adequate number of studies to carry out subgroup analysis according to differences in the number of sessions.
Numerous studies have shown that M1 cortex stimulation, including invasive and non-invasive techniques, can relieve pain, which might be the basis for performing tDCS over M1 (30, 39). tDCS over M1 is more likely to control pain than tDCS over the left DLPFC because the former acts by modulating the sensory component of pain (9, 10), while the latter is related to the cognitive and emotional aspects of pain (40). No serious side-effects were found in the included studies and tDCS did not adversely affect cognition in any way.
Although the search field was expanded by including free words and keywords, ultimately only 6 studies could be included in the meta-analysis. Although all the included trials described placement of the anode over the C3 position based on the International 10/20 EEG System, which corresponds approximately to the location of the left M1, the location of C3 was measured by different researchers, and it is therefore difficult to assess whether these studies target the same brain functions. All the included trials employed stimulation with intensities of 2 mA; however, the size of electrodes differed, and it is also unclear whether these different sizes affect the function of tDCS. The included studies measured pain on different scales including visual analogue scales, numerical rating scale, and visual numerical scale. Furthermore, pain was not measured exactly at the same time in various studies (28–33). In addition, there were differences among the trials in terms of the number of sessions, duration, devices, and the length of time from fibromyalgia onset. All these differences across studies might have introduced potential biases into the meta-analysis. However, there was insufficient data to perform subgroup analysis. Finally, the pain scores were reported by patients, and are thus subjective and might lead to measurement bias.
Two studies did not describe the methods for randomization (32, 33), which might increase selection bias, and 4 studies did not describe concealment of the randomization scheme (30–33), which might also increase selection bias. However, all included studies conducted blinding of participants and raters (28–33), which might decrease performance bias and detection bias. Two researchers (YB, ZW) independently extracted data according to a worksheet, and disagreements were resolved through consultation or discussion with a third person (QQ), which might decrease the risk of bias within studies. Considering these limitations and potential biases, the results of the current meta-analysis must be interpreted with caution, especially in terms of cathodal stimulation, stimulation over the DLPFC, and single sessions of stimulation. Moreover, although attempts were made to obtain data regarding the follow-up period and to contact the authors, it was not possible to calculate the overall effects during the follow-up period, which limits the value of the present analysis. Further studies with larger sample sizes are needed to provide more evidence on the use of tDCS for fibromyalgia.
This meta-analysis shows that anodal tDCS over M1 was more likely to control pain and improve general fibromyalgia-related function in patients with fibromyalgia than sham tDCS. However, owing to the potential biases and small sample size, there is insufficient evidence to draw conclusions about the efficacy of tDCS in fibromyalgia, especially cathodal stimulation over the DLPFC, and tDCS on the pressure pain threshold in patients with fibromyalgia. No serious side-effects or adverse effects on cognition were found in the included studies.
The authors would like to thank Zhi-rui Zhou for assistance with formulating the search strategies.


 Click to show fullsize
Click to show fullsize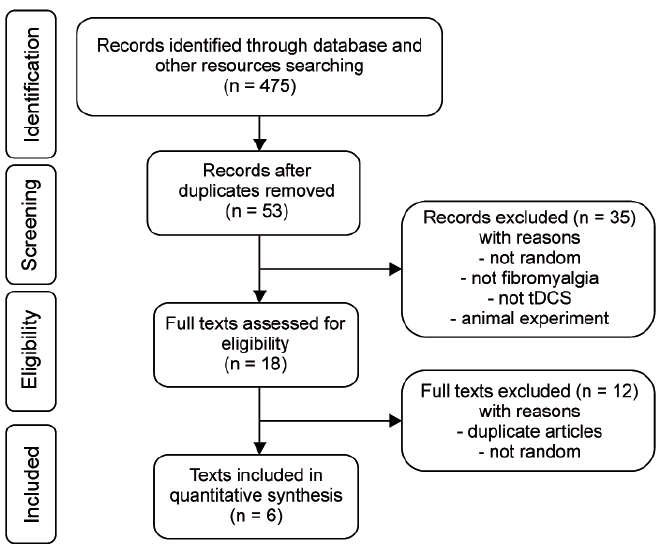 Click to show fullsize
Click to show fullsize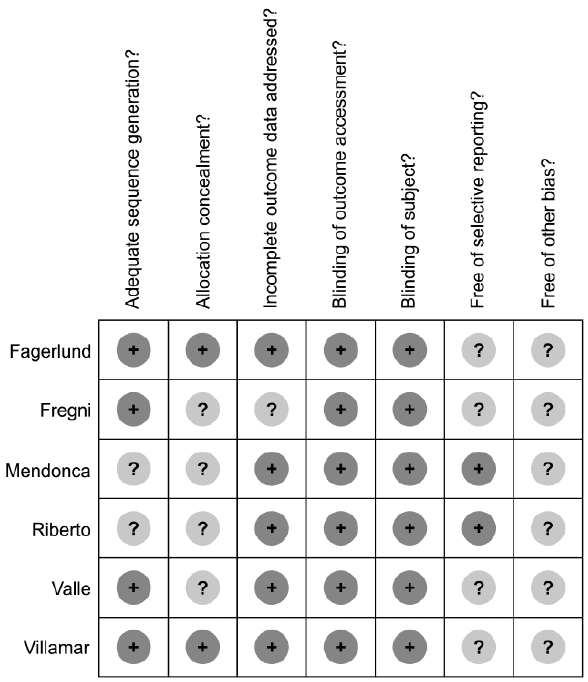 Click to show fullsize
Click to show fullsize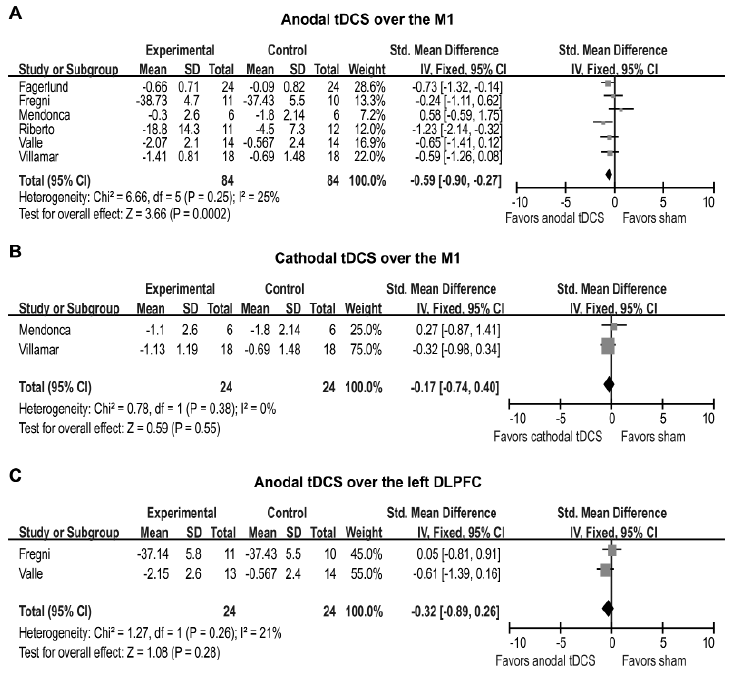 Click to show fullsize
Click to show fullsize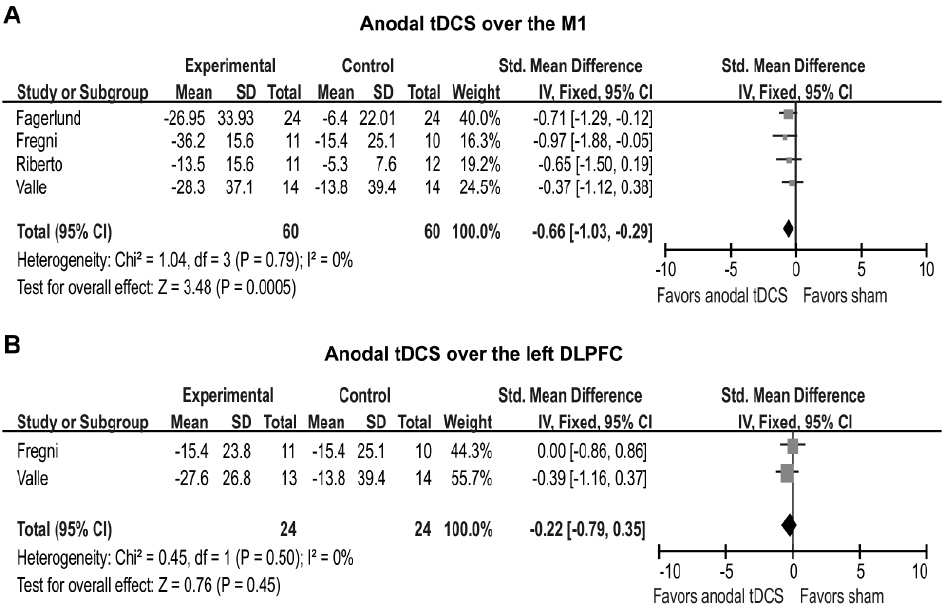 Click to show fullsize
Click to show fullsize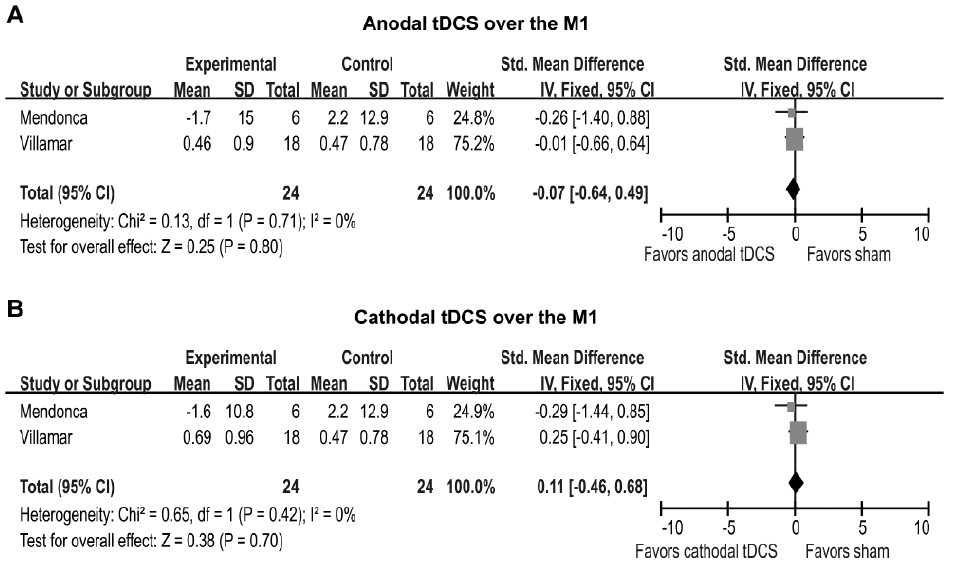 Click to show fullsize
Click to show fullsize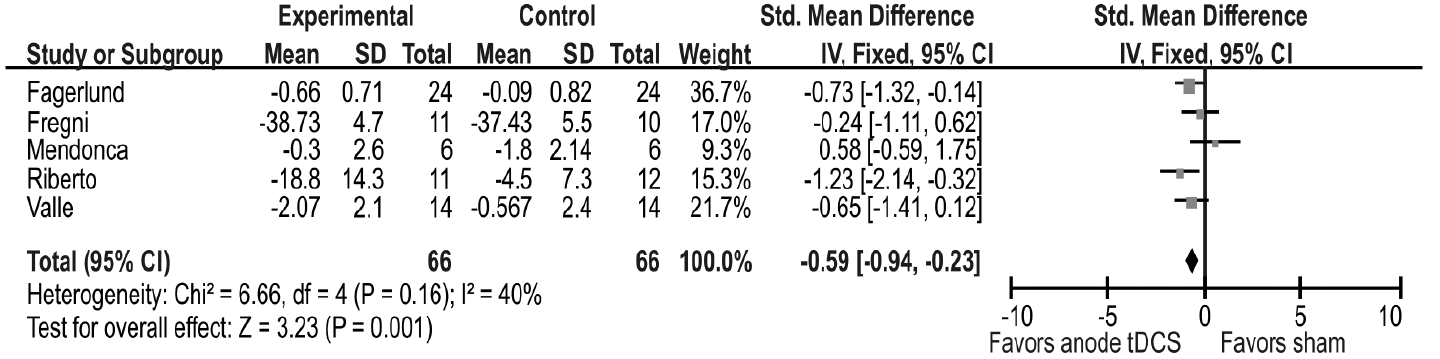 Click to show fullsize
Click to show fullsize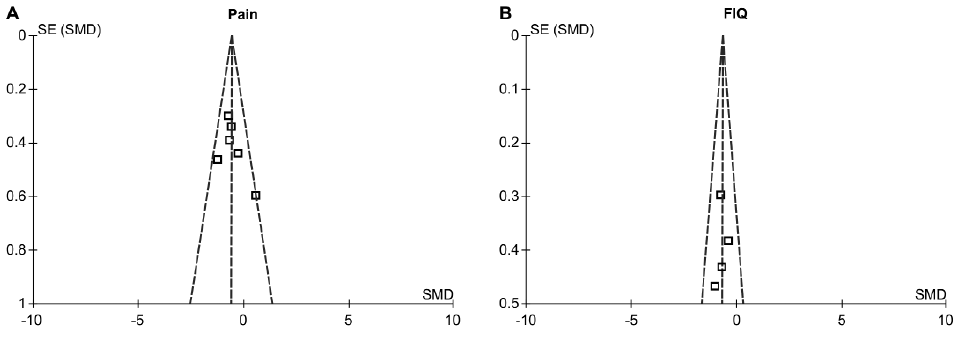 Click to show fullsize
Click to show fullsize