OBJECTIVE: To evaluate the effects of stretching on hamstring muscle compliance indirectly and directly.
METHODS: Twelve healthy men were instructed to perform passive stretching of one leg daily over 4 weeks, while the other leg served as a control. An instrumental straight leg raise was used to measure stretching force and muscle compliance indirectly with surface electromyography to measure muscle activity during stretching. Muscle compliance was measured directly by computerized muscle tonometer. The thickness of the biceps femoris muscle was measured by ultrasound and knee flexion strength by a dynamometer.
RESULTS: In the stretched legs the mean increase in straight leg raise was 17° after 4 weeks (p < 0.001) and the mean stretching force increased by 19 N (p < 0.001). Improved straight leg raise correlated with biceps muscle thickness (r = 0.74). The angle at which stretching was first felt increased by 15° in the stretched legs (p < 0.001). Controls showed no significant changes in straight leg raise. There was no difference in force between the stretched and control legs in comparison of the same angles. No significant changes were noted in muscle compliance, surface electromyography or isometric maximal knee flexion strength.
CONCLUSION: Stretching improved passive straight leg raise with no change in muscle compliance. Muscle viscoelastic properties and strength were preserved despite improved straight leg raise.
Key words: muscle compliance, muscle tonometer, passive stretching, range of motion, isometric strength.
J Rehabil Med 2009; 41: 80–84
Correspondence address: Jari Ylinen, Central Hospital of Central Finland, Department of Physical and Rehabilitation Medicine, Keskussairaalantie 19, FI–40620 Jyväskylä, Finland. E-mail: jari.ylinen@ksshp.fi.
Submitted February 20, 2008; accepted August 21, 2008
INTRODUCTION
Good hamstring muscle flexibility is essential in several sports including competitive aerobics, gymnastics, hurdles and the triple jump. Tight hamstring muscles may be a potential risk factor for strain injuries in sports in which a full range of movement (ROM) is needed (1). A stiff and short hamstring muscle-tendon unit may be a risk factor for low-back pain and the development of patellar tendinopathy (1, 2). However, research so far has not clearly defined the importance of stretching (3). Studies evaluating the effectiveness of different stretching methods have typically focused on hamstring muscles, probably because these muscles are often tight and are easy to stretch without interference from joint structures. Many studies have shown that even a single stretch can improve ROM, although the change lasts for only a few minutes (4, 5). Long-term exercising is thus needed to show long-lasting results, but even then the effects may disappear within a few weeks after exercise has ceased (6, 7).
Muscle compliance depends on the viscoelastic properties and contraction state of the motor unit elicited by electrical activity of the motor nerve it innervates. In the clinic, muscle compliance is commonly assessed by pressing a finger into the muscle after the patient relaxes it; thus assessment by compression describes resistance of the tissue to mechanical deformation. The greater the effort required, the higher the viscoelastic resistance, if the evaluation is performed while the muscle is at rest. Viscoelastic properties also aid in resistance to lengthening of the muscle and in restoring the resting length of the muscle. Muscle contraction, i.e. activity of the contractile part of the muscle, may greatly exceed viscoelastic force and increase muscle tone. The contractile state depends on the motor drive to the muscle, and although it is quite difficult to achieve complete relaxation of the muscle, electrical activity at rest is very low in healthy muscle and does not significantly affect muscle compliance (8).
Several devices have been developed to measure muscle compliance, but there is no gold standard method to assess it. Muscle compliance can be measured directly or indirectly. Indirect measurement is performed by moving the joint and measuring the resistance caused by the tendo-muscular system. Kubo et al. (9) found that passive resistance was independent of the elasticity of tendon structures, i.e. due to muscle stiffness. However, near end ROM, the resistance of the joint capsule and ligaments increasingly affect the results. The direct compliance measurement is performed by pressing the indenter of the tonometer perpendicular to the muscle, thus ensuring that joint structures do not affect the results. The position of the joint, however, will change the thickness of the muscle, which will affect muscle tone (10). Thus, muscle tone has to be measured in the same position for comparisons across values. Because previous studies have applied only the indirect method, the purpose of the present study was to use the direct and indirect approaches to evaluate the effects of stretching exercise on muscle (11).
METHODS
Design and settings
A comparative follow-up study with control group was performed in the Department of Physical and Rehabilitation Medicine at Jyväskylä Central Hospital, Finland.
The participants, all men who reported that their thigh muscles were stiff, were recruited from the city of Jyväskylä by advertising on the noticeboard at the University of Jyväskylä. Only males were recruited, because they are more likely to report muscle stiffness and form a larger potential participant population than women, who typically are more flexible (12). In addition, in people with stiff hamstring muscles straight leg raise (SLR) is restricted by pain sensation; pain can be more broadly variable among women because of the menstrual cycle, which would have required consideration of another study parameter (13, 14). All volunteers were tested and only those with a manually performed passive SLR ≤ 70° and normal ROM in the hip joint (flexion > 120° while the knee was flexed) were accepted for the study.
The study was approved by the local ethics committee.
Study population
Finally, 12 healthy men participated in this study (Table I). The men were not athletes, but on average engaged in recreational sports 4 times a week; most commonly cycling, running and ball games. Four were white, 6 were blue collar workers and 2 were students. All participants gave a written consent before entering the study.
| Table I. Demographics of the study population |
| | Mean (SD) | Range |
| Age, years | 34 (10) | 23–49 |
| Height, cm | 178 (5) | 170–188 |
| Weight, kg | 82 (10) | 62–104 |
| BMI, kg/m2 | 26 (2) | 21–31 |
| SD: standard deviation; BMI: body mass index. |
Outcome measures
All measurements were performed at baseline and after a 4-week home stretching programme. No stretching was performed on the day prior to the post-tests. The same tester performed the measurements. There was no warm-up before the measurements, which were always performed in the order described below.
Ultrasound (Nemio SSA-550A, Toshiba Ltd, Tokyo, Japan) was used to measure the thickness of the skin, subcutaneous fat and the biceps femoris muscle midway between the gluteal fold and the fold at the middle of the popliteal cavity, which appears when the knee is flexed. For this measurement each participant was lying prone with legs straight and feet strapped together to ensure a similar inter-individual position.
Muscle compliance was measured with a computerized muscle tonometer (CMT, Medirehab Ltd, Muurame, Finland), with each subject lying in the same position (15). The indenter, with a probe area of 1 cm2, was placed perpendicularly above the site that was measured for tissue thicknesses (Fig. 1). Measurement started when the indenter touched the tissue and exerted a force of 0.03 N. The speed of the indenter was set at 1 mm/sec, maintained until the resisting force reached a preset value of 15 N; it then returned to the starting position.
Fig. 1. Direct measurement of muscle tone with computerized tonometer. The motor pushes the indenter at a constant speed onto the muscle and resisting force and travel are registered continuously. The work performed is calculated from these parameters.
The CMT quantifies the amount of tissue displacement per unit force applied by a probe as it is pressed onto the tissue (16). The result of a CMT does not rely only a single measurement of depth in relation to specific force, but uses a sampling rate of 200 samples per second from which the work (J) done is counted while the probe compresses the tissues (area under the curve, AUC) (17). It correlates inversely with tissue stiffness, because with constant force the amount of work is less when the distance travelled by the indenter is shorter.
Measurements were performed twice consecutively at baseline to evaluate the repeatability of the AUC. For the baseline and follow-up comparison the first measurement was used.
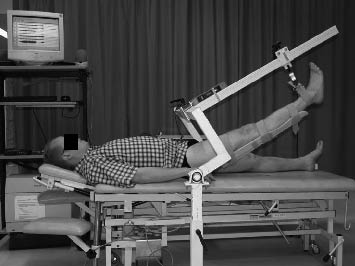
The calibration of the instrumental SLR device (Linden Ltd, Muurame, Finland) was checked with 10 kg and 20 kg standard weights, the Pro 360 Digital protractor goniometer (Mitutyo Ltd, Tokyo, Japan) and a stopwatch (Citizen, Tokyo, Japan). The men lay supine with both legs straight. One leg was held down by a strap, which went above the patella and around the examination table. A splint was attached behind the other leg to prevent flexion or hyperextension of the knee joint, and the leg was fastened to the SLR shaft at the level of the malleoli with a strain-gauge dynamometer (DS Europe Ltd, Milan, Italy) in between (Fig. 2). The shaft was set to run along the measured leg in the sagittal plane. The hip joint was set in the coronal and horizontal planes on the same level as the axis of the motor to which the shaft was attached. The angular velocity was set to 3°/sec. The speed was set low so that participants could keep their muscles relaxed and tell the tester about any discomfort arising as the stretching force continuously increased along with the angle of the hip joint. They were instructed to report to the tester, when they first felt stretching in their muscles and when the stretching became so uncomfortable that it could not be increased further. To evaluate repeatability, the measurement was repeated after 30 sec at the first testing occasion. For comparisons, the first measurement was selected.
Fig. 2. Instrumented straight leg raising device lifting the leg at a constant speed with continuous monitoring of angle, resisting force and surface electromyography.
A Muscle Tester ME3000 Professional (Mega Electronics Ltd, Kuopio, Finland) was used continuously to record 4-channel bipolar surface electromyography (sEMG) during compliance measurements. Ag/AgCl-electrodes (M-00-S, Medicotest, Ølstykke, Denmark) were applied after shaving hairy areas and careful cleaning of the skin to ensure good contact. One electrode was placed on the skin 4 cm below the gluteal fold in the middle of the biceps femoris muscle and the second below it along the body of the muscle. Two electrodes were placed on top of the gluteus maximus muscle. The distance between the mid-point of each pair of electrodes was 4 cm. Reference electrodes with preamplifier cables were placed over the greater trochanter. The raw sEMG signal was recorded at a sampling rate of 1000 Hz and analogically frequency band-pass filtered using a high-pass corner frequency of 7 Hz and the anti-aliasing filter (Butterworth) with a corner frequency of 500 Hz; amplification was achieved by a common mode rejection ratio of > 130 dB, gain 1000, and noise < 1 µV. The signal was analogue-to-digital converted (12-bit), and stored in a personal computer for later analysis. To ensure synchronization for the sEMG analysis, SLR force and angle were also transferred to the computer with this device, and occupied 2 channels. The measurement process was followed online as the computer program created real-time force and angle curves based on the data at a rate of 100 Hz.
Maximal isomeric knee flexion strength was measured by a David 200 Leg machine (David Industries Ltd, Outokumpu, Finland) in a sitting position with the hip joint at 80° and the knee joint at a 60° angle. The body was fastened to the seat with a belt running over the pelvis and the thigh was attached to the seat just above the patella. The other leg was resting on the stool during the test. Participants first performed 3 submaximal contractions of hamstring muscles towards knee flexion, gradually increasing the force to become accustomed to the position and to warm-up. Thereafter they performed 3 maximal efforts lasting up to 5 sec with 2 min pauses in between. The best effort was selected for the analysis.
Interventions
Each participant received instruction in the progressive stretching method. In the standing position, they were instructed to keep the supporting left leg and back straight while the right leg was lifted on the chair or table with the knee comfortably bent so that no marked tension was felt in the hamstring muscles. Then the knee was pushed down with the hand to straighten the joint and thus stretch the hamstrings without leaning forwards. Every 2 or 3 days participants were told to raise the support on which they placed the leg by 5 cm. The increase in height was achieved by placing books on the chair or shifting to a taller object, such as from a chair to a table. Stretching exercising was to be performed once daily in set of 6 repetitions each lasting 30 sec with 30-sec intervals. The duration of the stretch and number of repetitions was based on previous studies (18). Participants each received written instructions as well as a training diary, which they agreed to complete. The stretching programme was continued as a home-based training programme for 4 weeks.
Data analysis
The results are expressed as means with standard deviations (SD) and with 95% confidence intervals (CI). The normality of the variables was evaluated by the Shapiro-Wilk test. Test-retest repeatability on the same day was evaluated by intraclass correlation coefficients (ICC) with the one-way random effects model. Coefficients of repeatability with 95% CI were calculated for each measurement. The α-level was set at 0.05 for all tests. Repeated measures were analysed with generalized linear models.
RESULTS
Stretching force increased in a curvilinear manner with increasing angle during measurement and there was no significant difference in SLR between the right and left legs at baseline (Table II). At the 4-week follow-up the mean tolerable angle in SLR of the stretched leg had increased significantly compared with baseline (p < 0.001) and it was also significantly greater compared with the control leg. The peak angle in the control leg showed no significant change between baseline and follow-up. The mean resisting force at the angle at which stretching was tolerated increased significantly at the follow-up compared with baseline for the stretched leg, but not for the control leg. However, there was no statistically discernible difference in force between the stretched and control legs in comparison of the same angles.
| Table II. Average tolerated range of motion prior to and after a 4-week period of regular stretching exercise, and angles at which the stretching was first felt in an instrumented straight leg raise |
| | Baseline | Change at 4 week follow-up | p-value* |
| Stretched leg Mean (SD) | Control leg Mean (SD) | Stretched leg Mean (95% CI) | Control leg Mean (95% CI) |
| Stretching felt: Angle, ° Force, N | 41 (12) 70 (7) | 43 (14) 71 (9) | 15 (11–18) 2 (–6–10) | 2 (–2–6) 1 (–4–6) | < 0.001 0.76 |
| Stretching tolerated: Angle, ° Force, N | 69 (9) 86 (13) | 68 (10) 84 (17) | 17 (14–20) 19 (9–28) | 2 (–2–6) 7 (–5–20) | < 0.001 0.11 |
| *Difference between sides. SD: standard deviation; CI: confidence interval. |
The angle at which stretching was felt in SLR, as well as the force required to produce it, also increased significantly at the follow-up compared with baseline (p < 0.001) and, again, there was no significant change in the control leg.
In the relaxed prone position, the mean sEMG activity of the biceps femoris muscle in the stretched leg was 11 (SD 7) µV at the baseline and 16 (SD 14) µV at the follow-up; that of the gluteus maximus muscle was 7 (SD 4) µV and 8 (SD 5) µV at the baseline and the follow-up, respectively. The mean amplitude sEMG activity of both muscles remained fairly constant throughout the SLR. There was no significant change in sEMG amplitude during SLR between legs or between the baseline and the follow-up.
The ICCs for 2 consecutive direct muscle compliance measurements (AUC) on the same test occasion for the stretched and control legs with CMT were 0.92 (95% CI 0.76–0.98) and 0.97 (95% CI 0.89–0.99). The mean maximal depth was 29.1 (2.9) mm in the stretched legs and 28.5 (2.7) mm in the controls at the baseline. The corresponding mean changes after 4 weeks were 2.1 (95% CI 0.3–0.38) mm and 3.0 (95% CI 1.5–4.4) mm for the stretched and control legs, respectively. Thus, the travel of the shaft increased somewhat in both legs, but there was no significant difference between the legs. The mean compliance expressed as work (AUC) was 0.27 (SD 0.03) J in the stretched legs and 0.27 (SD 0.02) J in the controls at the baseline. The corresponding mean changes after 4 weeks were –0.00 (95% CI –0.01–0.01) J and –0.00 (95% CI –0.10–0.01) J for the stretched and control legs, respectively. Thus, there was no significant difference compared with the baseline or between the stretched and control legs at the 4-week follow-up.
At the baseline mean maximal isometric knee flexion forces for the stretched and control legs were 302 (SD 57) N and 334 (SD 75) N, respectively; at the 4-week follow-up the corresponding mean changes were 9 N (95% CI: –3–22) and –10 N (–39–20). There was no significant difference in knee flexion strength between the legs at either the baseline or the follow-up.
The thickness of the biceps femoris muscle varied considerably across individuals and ranged from 52.7 mm to 72.6 mm. The mean (SD) thickness was 60.8 (6.1) mm and correlated with body weight (r = 0.82; 95% CI 0.47–0.95). There was no correlation between the thickness of biceps muscle and maximal angle in SLR at the baseline. However, at the follow-up there was a clear correlation between the change in SLR and the thickness of the biceps muscle in the stretched leg (r = 0.74; 95% CI 0.30–0.92).
According to the training diaries the mean (SD) frequency of stretching exercises was 23 (SD 4) times and range was from 15 to 28 times during the 4-week study period. The average total time spent on stretching exercises was 69 (SD 13) min.
DISCUSSION
The 4-week stretching programme performed at home produced significant changes in SLR. The peak angle increased by 25% and the angle at which stretching was first felt increased by 37%, while in the control leg the corresponding changes were insignificant. In the present study greater improvement occurred in participants with thicker muscles, which may be attributable to their greater potential to change. Chleboun et al. (19) noted that muscle volume accounted for most of the variance in muscle resistance during stretching.
Improved SLR could be wrongly interpreted resulting from a decrease in tissue resistance. However, at the same angles used at the baseline, there was no significant difference in the force required for stretching at the follow-up. These results are in agreement with those of previous studies, which also found that stretching exercise over 4–6 weeks improved the stretchability of hamstring muscles with improved ROM, but that the resistance to the stretch remained at the same level (20–23).
The resisting force in the end of passive SLR in the stretched leg increased by 19 N compared with baseline. This finding indicates that the gain in SLR angle resulted from an increased tolerance for force used in stretching. This hypothesis is also supported by the fact the stretch sensation was also elicited at a greater angle at the follow-up compared with baseline, which has not been reported previously. However, this outcome does not exclude structural changes that could have elicited an elevated sensory and pain threshold for stretching force. The resistive forces did not diminish, implying no attenuation in the resilience of tissues as a result of stretching. In addition, this finding indicates that the muscle’s capacity to restore energy during the stretch-shortening cycle may not decrease because of stretching, despite increased ROM. Animal studies suggest that stretching induces structural changes and improved stretchability because of an increase in the number of sarcomeres in a series (24). Thus, resilience can be maintained at low angles, even with the increase in total ROM. A larger angle in SLR at follow-up means, that the stretched leg can attain greater stretch with an accompanying greater tensile tissue stretch and energy absorption compared with baseline. Thus, increased work may be produced if the hamstring muscles are contracted with full ROM.
Magnusson (25) showed that static stretching does not affect muscle compliance, if the force used does not exceed the pain threshold. We wanted to avoid causing pain, but still use a stretching force at an effective level. Thus, progressive force was used in static stretching exercises during the course of one month.
Muscle electrical activity is related to muscle compliance. Increased activity will decrease muscle compliance (8, 26–28). However, in relaxed muscle, this activity is low and does not significantly affect resistance in stretching (8). In the present study, we noted that although complete relaxation of leg muscles was difficult to achieve in the supine position, sEMGs in both the biceps femoris and gluteus maximus muscles were low during stretching. Thus, passive tissue properties appear to be responsible for the increase in resistance with increased SLR after stretching exercise, as in previous studies (8, 29).
There are several different stretches to choose from for the hamstrings. Forward bending in the standing position is commonly taught, although it may strain the low back and has shown to be an ineffective stretching method in a randomized study (30). It was thus rejected in the present study.
It may be stated that a person’s legs cannot be seen as independent of each other. However, this is not the weakness of the current study. On the contrary, as people move, it will strain the leg muscles, but the gravity and forces exerted due to movements in the ordinary life commonly strain both legs similarly. Thus, the biological variance in compliance is assumed to be similar in both legs. Intervention that is directed to one leg only, as stretching in the present study, may cause the difference between the legs.
No previous studies have evaluated muscle compliance directly after stretching exercise. In the present study, the travel of the shaft increased similarly in both legs at the follow-up, while the work (AUC) did not increase. The difference in depth between baseline and follow-up is probably due to biological variance in measurements. Thus, no significant changes in muscle compliance were observed with CMT after the stretching intervention. Several studies have shown that stretching may cause an acute decrease in muscle strength following the stretching exercise (31, 32). The results of the present study do not counter this finding, as no stretching exercises were performed on the measurement day and the decrease in muscle strength has been shown to be transitory, disappearing soon after the stretching exercise (32).
In conclusion, stretching did not affect muscle compliance measured either directly or indirectly. Thus, elastic properties of the muscle and maximal force produced were sustained despite increased ROM. Stretching increased not only tolerance to stretching force, but also the angle at which the stretching was first felt.
ACKNOWLEDGEMENT
The research project was supported by a grant from Jyväskylä Central Hospital.
REFERENCES
1. Witvrouw E, Danneels L, Asselman P, D’Have T, Cambier D. Muscle flexibility as a risk factor for developing muscle injuries in male professional soccer players: a prospective study. Am J Sports Med 2003; 31: 41–46.
2. Gajdosik RL. Passive compliance and length of clinically short hamstring muscles of healthy men. Clin Biomech 1991; 6: 239–244.
3. Weldon SM, Hill RH. The efficacy of stretching for prevention of exercise-related injury: a systematic review of the literature. Manual Ther 2003; 8: 141–150.
4. Magnusson SP, Aagaard, Larsson P, Kjaer M. Passive energy return after repeated stretches of the hamstring muscle-tendon unit. Med Sci Sports Exerc 2000; 32: 1160–1164.
5. Spernoga SG, Uhl TL, Arnold BL, Gansneder BM. Duration of maintained hamstring flexibility after a one-time, modified hold-relax stretching protocol. J Athl Train 2001; 36: 44–48.
6. Depino GM, Webright WG, Arnold BL. Duration of maintained hamstring flexibility after cessation of an acute static stretching protocol. J Athl Train 2000; 35: 56–59.
7. Willy RW, Kyle BA, Wore SA, Chleboun GS. Effect of cessation and resumption of static hamstring muscle stretching on joint range of motion. J Orth Sports Phys Ther 2001; 31: 138–144.
8. Magnusson SP, Simonsen EB, Aagaard P, Boesen J, Johannsen F, Kjaer M. Determinants of musculoskeletal flexibility: viscoelastic properties, cross-sectional area, EMG and stretch tolerance. Scand J Med Sci Sports 1997; 7: 195–202.
9. Kubo K, Kanehisa H, Fukunaga T. Is passive stiffness in human muscles related to the elasticity of tendon structures? Eur J Appl Physiol 2001; 85: 226–232.
10. Alamäki A, Häkkinen A, Mälkiä E, Ylinen J. Muscle tone in different joint positions and at submaximal isometric torque levels. Physiol Meas 2007; 28: 793–802.
11. Gajdosik RL. Passive extensibility of skeletal muscle: review of the literature with clinical implications. Clin Biomech 2001; 16: 87–101.
12. Youdas JW, Krause DA, Hollman JH, Harmsen WS, Laskowski E. The influence of gender and age on hamstring muscle length in healthy adults. J Orthop Sports Phys Ther 2005; 35: 246–252.
13. Riley JL 3rd, Robinson ME, Wise EA, Price DD. A meta-analytic review of pain perception across the menstrual cycle. Pain 1999; 81: 225–235.
14. Greenspan JD, Craft RM, LeResche L, Arendt-Nielsen L, Berkley KJ, Fillingim RB, et al. Consensus Working Group of the Sex, Gender, and Pain SIG of the IASP. Studying sex and gender differences in pain and analgesia: a consensus report. Pain 2007; 132 Suppl 1: S26–45.
15. Ylinen J, Teittinen I, Kainulainen V, Kautiainen H, Vehmaskoski K, Häkkinen A. Repeatability of a computerized muscle tonometer and the effect of tissue thickness on the estimation of muscle tone. Physiol Meas 2006; 27: 787–796.
16. Leonard CT, Deshner WP, Romo JW, Suoja ES, Fehrer SC, Mikhailenok EL. Myotonometer intra- and interrater reliabilities. Arch Phys Med Rehabil 2003; 84: 928.
17. Ylinen J, Airaksinen O, Kolari P. Digital tissue compliance meter. Acup Electro-Ther Res 1993; 18: 169–174.
18. Ylinen J. Stretching therapy. For sport and manual therapies. Oxford: Churchill Livingstone; 2007.
19. Chleboun GS, Howell JN, Conatser RR, Giesey JJ. The relationship between elbow flexor volume and angular stiffness at the elbow. Clin Biomech 1997; 12: 383–392.
20. Gajdosik RL, Allred JD, Gabbert HL, Sonsteng BA. A stretching program increases the dynamic passive length and passive resistive properties of the calf muscle-tendon unit of unconditioned younger women. Eur J Appl Physiol 2007; 99: 449–454.
21. LaRoche DP, Connolly DAJ. Effects of stretching on passive muscle tension and response to eccentric exercise. Am J Sports Med 2006; 34: 1000–1007.
22. Magnusson SP, Simonsen EB, Aagaard P, Sorensen H, Kjaer M. A mechanism for altered flexibility in human skeletal muscle. J Physiol 1996; 497: 291–298.
23. Reid DA, McNair PJ. Passive force, angle, and stiffness changes after stretching of hamstring muscles. Med Sci Sports Exerc 2004; 36: 1944–1948.
24. Williams P, Simpson P, Kyberd J, Kenwright J, Goldspink G. Effect of rate of distraction on loss of range of joint movement, muscle stiffness, and intramuscular connective tissue content during surgical limb lengthening: a study in the rabbit. Anat Rec 1999; 255: 78–83.
25. Magnusson SP. Passive properties of human skeletal muscle during stretch maneuvers. A review. Scand J Med Sci Sports 1998; 8: 65–77.
26. Halbertsma JP, van Bolhuis AI, Goeken LN. Sport stretching: effect on passive muscle stiffness of short hamstrings. Arch Phys Med Rehabil 1996; 77: 688–692.
27. Gubler-Hanna C, Laskin J, Marx BJ, Leonard CT. Construct validity of myotonometric measurements of muscle compliance as a measure of strength. Physiol Meas 2007; 28: 913–924.
28. Murayama M, Nosaka K, Yoneda T, Minamitani K. Changes in hardness of the human elbow flexor muscles after eccentric exercise. Eur J Appl Physiol 2000; 82: 361–367.
29. Halbertsma JPK, Goeken LNH. Stretching exercises: effect of passive extensibility and stiffness in short hamstrings of healthy subjects. Arch Physiol Med Rehabil 1994; 75: 976–981.
30. Sullivan MK, Dejulia JJ, Worrell TW. Effect of pelvic position and stretching method on hamstring muscle flexibility. Med Sci Sports Exerc 1992; 24: 1383–1389.
31. Mohr T, Kjaer M. Viscoelastic stress relaxation during static stretch in human skeletal muscle in the absence of EMG activity. Scand J Med Sci Sports 1996; 6: 323–328.
32. Rubini EC, Costa AL, Gomes PS. The effects of stretching on strength performance. Sports Med 2007; 37: 213–224.