
From 1Experimental and Clinical Medicine, University of Florence, 2Azienda Ospedaliera Universitaria Careggi, Florence, 3Research Laboratory for Movements in the Biological Systems, Uniser, Pistoia and 4Functional Rehabilitation Activities, Azienda Unità Sanitaria Locale, Toscana Centro, Prato, Italy
ntroduction: Physiotherapy plays a key role in cerebral palsy rehabilitation, through addressing body function/structure deficits, minimizing
activity limitations, and encouraging participation. The muscle shortening manoeuvre is an innovative
therapeutic technique, characterized by the ability
to induce changes in muscle strength in a short time.
Objective: To describe the applicability and estimate the effect of the muscle shortening manoeuvre applied to improve motor weakness and joint excursion of the ankle in children with hemiplegic cerebral palsy.
Methods: Nine children with hemiplegic cerebral
palsy received 3 intervention sessions in one week. Muscle strength, passive and active range of
motion were assessed before, during and after the training, and at 1-week follow-up.
Results: The children experienced an immediate increase in muscle strength and joint excursion of the ankle; the improvements were still present at follow-up after 7 days.
Conclusion: The muscle shortening manoeuvre may be an effective intervention to induce an immediate increase in muscle strength and range of motion of the ankle in children affected by hemiplegia due to cerebral palsy, thus promoting better physical
functioning.
Key words: ankle joint; cerebral palsy; motion therapy, continuous passive; muscle strength; physical therapy modalities; recovery of function.
Accepted May 10, 2021; Published Jun 17, 2021.
JRM-CC 2021; 4: jrm00064
Correspondence address: Francesco Ferrarello, Functional Rehabilitation Activities, Azienda USL Toscana Centro, Prato, 59100 Prato, Italy. E-mail: francescoferrarello@tiscali.it
Doi: 10.2340/20030711-1000062
The muscle shortening manoeuvre is a continuous passive motion therapy, which has 2 components; muscle shortening and solicitation in traction. The intervention is administered by a physiotherapist and is characterized by the ability to induce changes in
muscle strength in a short time. This report describes the applicability and the effect of the manoeuvre when applied to improve motor weakness and joint excursion of the ankle in children affected by hemiplegia due to cerebral palsy. Nine children received 3 intervention sessions in one week. Muscle strength, and range of motion were monitored. The children experienced an increase in muscle strength and joint excursion of the ankle. The muscle shortening manoeuvre appears to be suitable for use in children affected by hemiplegia due to cerebral palsy. Further research is needed to verify the effectiveness of the manoeuvre in promoting better physical functioning in these patients.
Therapeutic interventions for children with cerebral palsy (CP) embrace the extent of the International Classification of Functioning, Disability and Health (ICF), aiming to address body function/structure deficits, minimize activity limitations, and encourage participation (1). Several physiotherapy interventions, such as strengthening, task-specific practice, and mobility training, to name a few, have been shown to be effective in improving motor ability (2).
The muscle shortening manoeuvre (MSM) is a therapeutic intervention characterized by the ability to induce changes in muscle strength in a short time. The manoeuvre was introduced by Grimaldi (3) and is derived from Feldman’s λ model of motor control (4). In the λ model, regulation of the stretch reflex threshold (SRT), the lower muscle length or joint angle at which motoneuronal recruitment occurs, plays a pivotal role. The dynamic SRT is influenced by stretch speed. The tonic stretch reflex represents the specific value of the dynamic SRT at zero velocity. Dynamic and tonic SRTs are expressed in relation to the configuration of the joints, within a body frame of reference (5).The ability to control the SRT angle when it is placed within the biomechanical range of a joint, differentiates the joint configurations in which muscles are spastic from those in which they are not (6,7).
The MSM has 2 components; muscle shortening and solicitation in traction. A physiotherapist applies a series of fast accelerations to a skeletal segment (e.g. the foot) in the presence of forces acting in the opposite direction (added mass and/or elastic element), thus producing tensile stress. As a result, the manoeuvre provokes a dynamic lengthening associated with sudden shortening of the agonist and antagonist muscles. Tissue deformation stimulates the muscle spindles, with an enrolment of motor units and an attempt to produce muscle tension. However, the development of tension is prevented by the sudden shortening of the muscle due to the therapeutic manoeuvre. The ambiguous perceptual stimuli are thought to determine an informational catastrophe, thus leading the central nervous system to develop new tonic SRTs, and a subsequent improvement in active muscle recruitment (3, 8–10). Positive effects have been reported in muscle strength and range of motion.
The aim of this retrospective analysis is to describe the applicability and estimate the effect of Grimaldi’s MSM applied to improve motor weakness and joint excursion of the ankle in children with hemiplegia due to CP.
This study analysed de-identified data from 9 children with hemiplegic CP, who were referred to local health authority outpatient rehabilitation services (February to June 2009). Parents provided written informed consent, including consent for data extraction from chart review, and eventual dissemination through publication. Children gave informed oral assent before the intervention was administered. The procedures were in accordance with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Participants
The participants’ age ranged from 8 to 12 years, and the children were able to walk independently without assistive devices. None of them had undergone orthopaedic surgery within the previous 12 months or botulinum toxin therapy within the previous 6 months. They did not take anti-spastic medications, and did not have dyskinesia, dystonia, severe muscle contractures, or other relevant comorbidities. The children did not participate in any other rehabilitation intervention during the follow-up period.
Intervention
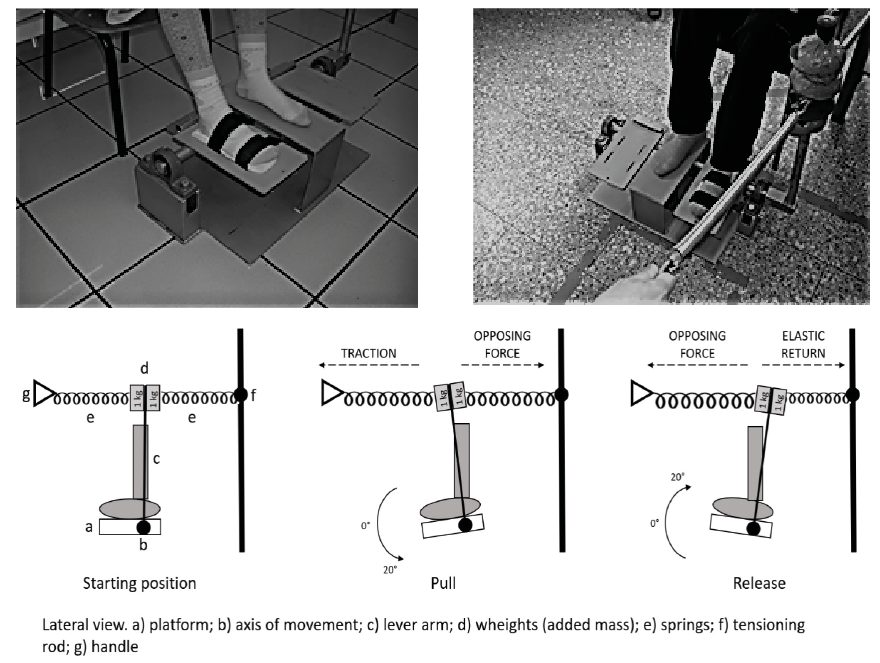
A mechanical device was used to perform repetitive passive mobilization of the ankle (Fig. 1). The device comprises 3 rectangular parallel platforms. The horizontal axis of movement of the platforms coincides with the projection of the ankle transverse axis, thus isolated dorsal and plantarflexion movements can be performed during mobilization. An accelerometer (PCE Inc., (Southampton, UK) MSR 145S, sampling rate 50 points/s) positioned on one end of the device’s axis records the frequency and excursion of the oscillations. The other end of the axis is connected to a perpendicular lever arm. Two weights and 2 springs have been placed at the lever arm upper extremity. One of the springs is connected to a tensioning rod; the therapist acts on the other spring by means of a handle and small arm movements, thus inducing oscillations of the platform at the desired amplitude and frequency (Fig. 1).
Fig. 1. Mechanical set-up of the device. Alternating pull and release induce oscillations of the platform, producing relative muscle lengthening followed by sudden shortening of ankle dorsi- and plantar-flexor muscles. The fast accelerations are applied while the ankle is subjected to a force acting in the opposite direction (tensile stress).
The subject was seated on a chair with the hip and knee joint at 90° of flexion. Cushions were utilized to adjust the height of the seat. The plegic foot was positioned on the moving platform, on a foam layer. Velcro strips prevented the foot from slipping. Three, 20-min dorsal and plantarflexion mobilization sessions were administered by means of the device, at a frequency of 1.5 Hz. The child was invited to sit quietly, relax, avoid any voluntary movement, and let the therapist move their foot. The child was asked to focus attention on the ankle, they were also allowed to talk with parents (or relatives) or browse/read a book. The therapist induced a joint excursion from 20° of dorsiflexion to 20° of plantarflexion. The intervention was individually administered for one week, every other day, face-to-face in paediatric settings, by trained physiotherapists.
Outcome measures
Muscle strength, passive and active range of motion (PROM and AROM) were assessed before the first treatment session (baseline, T0), at the end of the 1st, 2nd, and 3rd sessions (T1, T2, and T3, respectively), and one week after the 3rd session (follow-up, T4). The strength of the ankle dorsal and plantar flexor muscles were measured with a digital handheld dynamometer (in kg) (Weiheng Portable Electronic Scale; Guangzhou Weiheng Electronics Co., Ltd, Guangdong, China). Three joint angles were considered (neutral ankle position 0°, plantarflexion 20° and 40°). Three tests per-angle were performed, for the assessment that was considered the best result. Ankle excursion was measured with a manual goniometer, computing from maximum dorsiflexion to maximum plantarflexion and vice versa. The AROM was evaluated by applying minimal manual resistance.
The minimal detectable change (MDC95) has been estimated in children with CP for plantar flexors strength (0.211 kg) and dorsiflexion excursion (7.94°) (11, 12).
The Selective Motor Control scale (SMC) (13) and the modified Physician Rating Scale (PRS) (14) were administered at T0 and T3. The SMC was designed to assess the ability to voluntarily control the dorsiflexors; it ranges from 0 (no intentional movement) to 4 (intentional movement throughout the available range of motion) (13). The PRS is an observational gait assessment tool; the score ranges from –2 (poor) to 22 (normal) per limb (14). Children were videotaped according to a protocol; the recordings were analysed offline.
The intervention progression and assessment procedure are shown in Table I.
Table I. Intervention progression and assessment procedure
Statistical analysis
Descriptive statistics were performed to analyse demographic, clinical, and outcome data. Friedman’s test was used to analyse variation in muscle strength and range of motion. In case of significant results, post hoc tests were performed (Dunn’s test). The Hodges-Lehmann estimator was used to estimate the 95% confidence intervals (95% CIs) of the median differences. Data on plantar flexors strength and dorsiflexion excursion were further analysed by plotting the median of the differences (95% CI) and the range of random measurement error (i.e. the interval between the ±MDC95 values); MDC95 proportions representing the children showing an improvement in performance (i.e. equal to or greater than the absolute values of the MDC95) were also calculated. Fisher’s exact test was used to investigate variation in SMC score. Change in PRS scores was examined using the Wilcoxon signed-rank test. IBM SPSS Statistics for Windows (version 20.0; IBM Corp, Armonk, NY, USA) was utilized for calculations. The significance level was set at p < 0.05.
Demographic, clinical, and outcome data are shown in Table II. Friedman’s tests showed significant differences between the assessments (Table III). The median increase in muscle strength, PROM, and AROM are shown in Fig. 2 and Fig. 3. Dunn’s post hoc tests showed significant improvements at T2, T3 and T4 (Table III).
For plantar flexors strength, analysis based on MDC95 showed partial overlapping of the 95% CIs at T1 and, in one case, at T4 (Fig. 2). The proportion of children showing an improvement in performance were 44–67–44% at T1, 100–89–78% at T2, 100–100–89% at T3, and 100–100–67% at T4 (Fig. 2). In PROM and AROM analysis overlapping of the 95% CIs was observed across assessments (Fig. 3); the proportions of children showing improvements were 56–89% (PROM) and 56–78% (AROM) (Fig. 3).
No differences were observed between SMC scores at T0 and T3 (Fisher’s exact test = 9.579, p = 0.071). Improvement in PRS scores was observed at T3 (Z = 2.536, p = 0.011; Hodges-Lehmann estimator 4.0, 95% CI 2.0/6.0).
Table II. Demographic, clinical, and outcome data
Table III. Friedman’s tests and post hoc analysis results
Fig. 2. Change in muscle strength. (A) From left to right: median of the differences (kilograms) between T0 and T1, T0 and T2, T0 and T3, and T0 and T4 for each of the joint angle tested, respectively. The error bars represent the 95% confidence interval. (B) From left to right: individual differences (kilograms) between T0 and T1, T0 and T2, T0 and T3, and T0 and T4 for each of the joint angle tested, respectively. The horizontal lines indicate a difference of 0 and, only for plantar flexor strength, the ±MDC95 values. D: Dorsiflexor; np: neutral position; P: plantar flexor; pf: plantarflexion.
Fig. 3. Change in range of motion of the ankle. AROM: active range of motion; PROM: passive range of motion. (A) From left to right: median of the differences (degrees) between T0 and T1, T0 and T2, T0 and T3, and T0 and T4. The error bars represent the 95% confidence interval. (B) From left to right: individual differences (degrees) between T0 and T1, T0 and T2, T0 and T3, and T0 and T4. The horizontal lines indicate a difference of 0 and the ±MDC95 values. AROM: active range of motion; PROM: passive range of motion.
This is the first report to describe the applicability of the MSM in children affected by CP. The intervention was administered in accordance with the study protocol and no adverse events were observed. Children experienced an immediate increase in muscle strength and joint excursion of the ankle; the improvements were still present at follow-up after 7 days. Interesting observations can be drawn from the analysis based on MDC95; it is derived from the standard error of the mean (SEM) and a 95% degree of confidence, and can be regarded as the minimum amount of change due to a real modification in performance rather than to the random measurement errors. Apart from T1, analysis of individual data showed a remarkable proportion of children (67–100%) with improvements in performance equal to or greater than the absolute values of the MDC95, for plantar flexors strength and ankle joint excursion (Table II, Fig. 2 and Fig. 3). The quality of gait pattern was also enhanced, probably due to the ability to perform a better push-off and swing phase; although an MDC95 value is not available for the PRS. Despite the variations observed in the children’s ability to move their ankles, change scores in the SMC were not significant.
This study has some limitations. An electro-goniometer would have given more accurate measurements of the ankle joint angles; a mean score of the 3 strength tests performed per-angle would have probably been more reliable. Moreover, we did not consider assessing spasticity; as it interferes with muscle strength and joint mobility, the use of an outcome measure such as the Tardieu Scale (15) or an objective, neurophysiological assessment, such as the tonic SRT measurement (5) would have provided additional data. In the current investigation, we chose the dosing of the intervention (i.e. 3 × 20-min sessions) with reference to a previous study (8); due to the exploratory nature of the research, alternative dosages (e.g. greater frequency and duration) could have been considered. Finally, children should have been monitored for a longer time.
The effect of the MSM was previously investigated in individuals with multiple sclerosis (8), spinal cord injury (9), and shoulder impingement (3, 10). The current findings regarding strength and joint excursion are in agreement with previous studies (3, 8–10). In the children in the current study, impairment of the ankle was due to muscle weakness and unbalanced muscle action. According to Feldman’s model, the modulation of SRTs allows interaction with the environment by mean of a fluent control of muscular forces and joint angle. Regulation of thresholds, and positional and velocity gains of the stretch reflex are consequences of supraspinal action and may have implications in motor control disorders related to diseases of the nervous system (4). The positive effect could be explained by the proprioceptive feedback due to the MSM, inducing a neuromuscular review; novel muscle tonic SRTs and configurations of the joint, within different body frames of reference (6, 7) may have produced a stronger and more balanced agonist-antagonist muscular action. We are aware that the findings are related to body structure, and not to activity and participation domains; moreover, in management of CP, upstream therapeutic effects (e.g. on other ICF domains) are not supported by substantial evidence (2). However, in the context of multiple limiting factors, an eventual positive effect of MSM may allow better engagement in goal-directed and motor learning-based interventions (2).
We conclude that the MSM is suitable for use in children affected by hemiplegia due to CP. Well-designed preclinical and clinical studies are needed to investigate its neurophysiological effect, relationship with human motor control and learning, and efficacy. Considerations should be made regarding the potential impact of the stimulation on spasticity; should a positive effect result, the minimal burden of the intervention would make it attractive compared with surgical or pharmacological interventions. Should the effectiveness be confirmed, further research may address how the MSM could help in minimizing activity limitations and encouraging participation.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize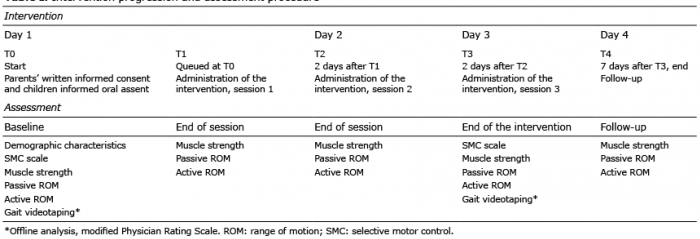 Click to show fullsize
Click to show fullsize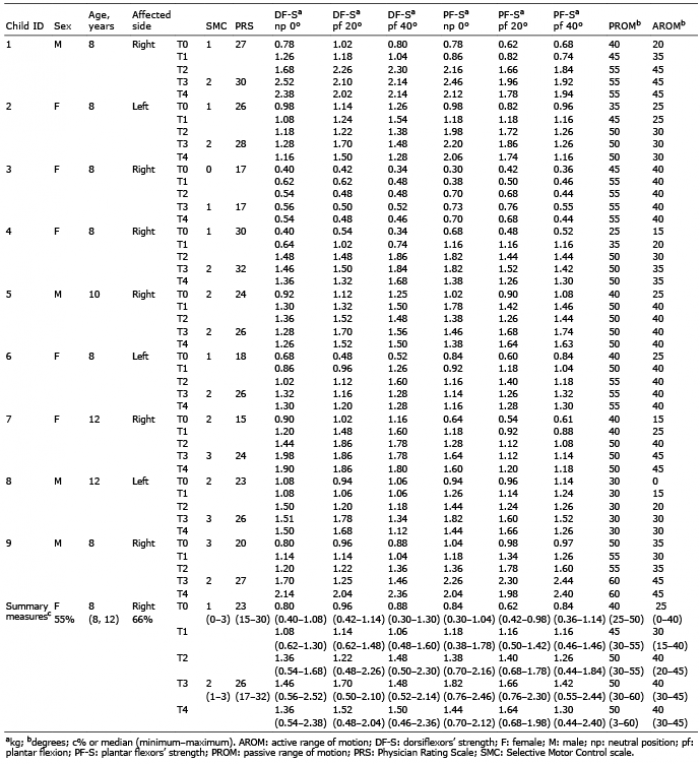 Click to show fullsize
Click to show fullsize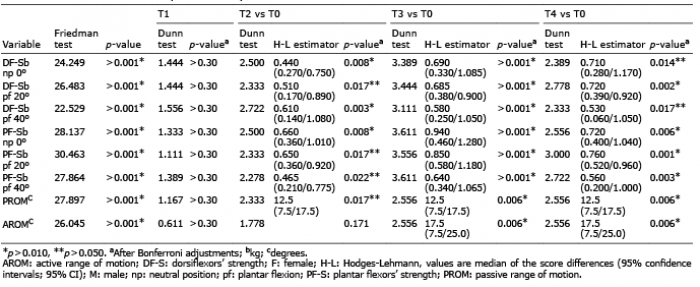 Click to show fullsize
Click to show fullsize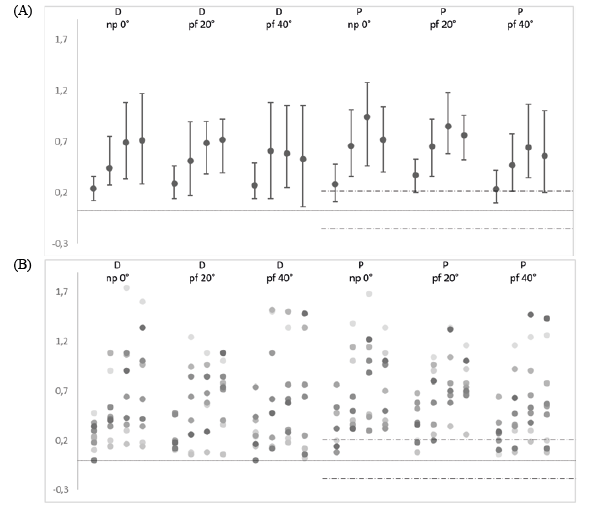 Click to show fullsize
Click to show fullsize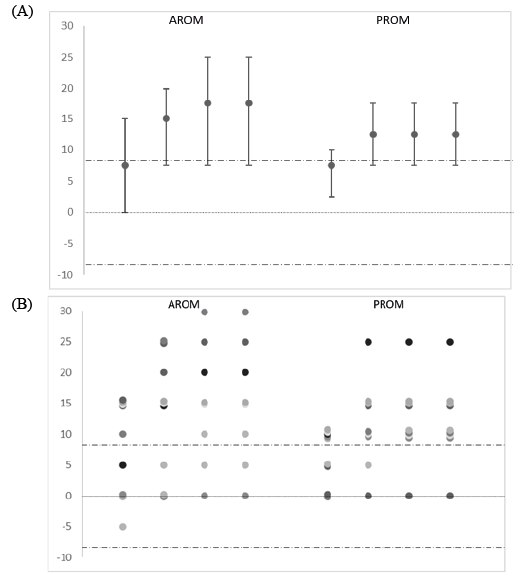 Click to show fullsize
Click to show fullsize