
1Department of Rehabilitation Medicine, Research School CAPHRI, Maastricht University, Maastricht, The Netherlands
2Adelante, Centre of Expertise in Rehabilitation and Audiology, Hoensbroek, The Netherlands
3Centre of Expertise Urban Vitality, Faculty of Health, University of Applied Sciences Amsterdam, Amsterdam, The Netherlands
4Department of Rehabilitation, Amsterdam University Medical Centers, University of Amsterdam, Amsterdam Movement Sciences, Amsterdam, The Netherlands
5Department of Pediatrics, Amsterdam University Medical Centers, University of Amsterdam, Amsterdam, The Netherlands
*Shared first authorship.
Background: To determine whether adolescents with generalized hypermobility spectrum disorder/hypermobile Ehlers-Danlos syndrome (G-HSD/hEDS) show changes in the level of disability, physical functioning, perceived harmfulness and pain intensity after completing multidisciplinary rehabilitation treatment.
Methods: Pre-test post-test design. Fourteen adole-scents with G-HSD/hEDS participated. The multidisciplinary rehabilitation treatment consisted of a combination of physical training and exposure in vivo. Physical training aims to improve aerobic capacity, muscle strength and propriocepsis for compensating hypermobility. Exposure in vivo aims to decrease disability and pain-related fear. Pre- and post-treatment assessments were conducted to assess the level of disability, physical functioning (motor performance, muscle strength and physical activity level), perceived harmfulness and pain intensity.
Results: After completing multidisciplinary rehabilitation treatment, the adolescents showed a significant and clinically relevant improvement (improvement of 67%, p < 0.01) in functional disability. Furthermore, significant improvements were found in motor performance (p < 0.01), muscle strength (p < 0.05), perceived harmfulness (p < 0.01) and pain intensity (p < 0.01) after completing multidisciplinary rehabilitation treatment.
Conclusion: Multidisciplinary rehabilitation treatment leads to a significantly and clinically relevant improvement in the level of disability for adole-scents with G-HSD/hEDS. Positive effects were also found in physical functioning, perceived harmfulness and pain intensity. Although the results of this multidisciplinary rehabilitation treatment for adolescents with G-HSD/hEDS are promising, further study is needed to confirm these findings in a randomized design.
Key words: chronic musculoskeletal pain; joint hypermobility; disability; multidisciplinary treatment.
Accepted Apr 15, 2020; Published May 8, 2020
JRM-CC 2020: 3: 1000033
Correspondence address: Thijs van Meulenbroek, Department of Rehabilitation Medicine, Maastricht University. PO Box 616. 6200 MD Maastricht, The Netherlands. E-mail: thijs.vanmeulenbroek@maastrichtuniversity.nl
In this study, changes in disability, physical function-ing and other pain-related outcomes are evaluated for hypermobile adolescents (age 12–21 years) with chronic musculoskeletal pain after following an outpatient multidisciplinary rehabilitation treatment. This treatment consists of a combination of physical training and cognitive-behavioural therapy (exposure in vivo). Physical training (8 weeks; 2 h 2×/week) aims to improve physical parameters, such as aerobic capacity, muscle strength and propriocepsis. Exposure in vivo (6 weeks; 1 h/week) aims to restore a normal pattern of daily functioning by decreasing pain-related fear. After treatment, the adolescents had lower levels of disability, decreased pain-related fear, a reduction in pain intensity and increased levels of physical func-tioning. It is concluded that the results are promising, but the findings are based on a small sample size with-out a randomized controlled group. Therefore, the results should be interpreted with caution.
Generalized joint hypermobility (GJH) is a non-symptomatic condition characterized by increased range of motion in multiple joints due to increased laxity of connective tissue (1). Previous studies suggest a relevant relationship between chronic musculoskeletal pain (CMP) and GJH, as GJH is a risk factor for CMP (2, 3). In case GJH occurs with one or more musculoskeletal manifestations, such as chronic pain, trauma, disturbed proprioception and joint instability, it is referred to as generalized hypermobility spectrum disorder (G-HSD) (4). Similar characteristics have been reported in children and adolescents with hypermobile Ehlers-Danlos syndrome (hEDS) (5). It has been suggested that G-HSD and hEDS are clinically indistinguishable (4, 5), both lacking a specific genetic profile and are therefore labelled as G-HSD/hEDS.
Compared with healthy peers, individuals with G-HSD/hEDS have a higher presence of physical complaints, such as activity-related pain (6), decreased muscle strength (7), impaired proprioception (8), reduced balance (9), multi-systemic dysfunction (such as hyper-elastic skin, ortho-static intolerance, gastrointestinal problems and organ dysfunction) (10) and significant disability (11). In addition, individuals with G-HSD/hEDS have also demonstrated an increased incidence of psychosocial complaints, such as pain-related fear (12) and psychiatric symptoms, including anxiety disorders, panic disorders and depression (13) compared with healthy peers.
Multidisciplinary rehabilitation treatment (MRT) in CMP may be effective in reducing disability and has been recommended in adolescents with G-HSD/hEDS (14, 15). Recently, a treatment protocol for MRT for adolescents with CMP, including a programme for adolescents with G-HSD/hEDS, was published (16). Adolescents with G-HSD/hEDS received physical training sessions and exposure in vivo (EXP) sessions. Results showed a clinically relevant and statistically significant decrease in functional disability in adolescents with CMP after MRT (17). However, based on these results, no conclusions could be drawn on potential improvements specifically for the subgroup of adolescents with G-HSD/hEDS. However, the treatment and measurement protocol was implemented in usual care, which led to a higher number of adolescents with G-HSD/hEDS.
This study has 2 primary objectives: first, to determine whether adolescents with G-HSD/hEDS showed changes in the level of disability (domain of participation) after following MRT. Secondly, to study whether improvements were found in physical functioning, perceived harmfulness and pain intensity in the adolescents with G-HSD/hEDS after MRT was finished.
Participants
In this pre–post-test design, 14 adolescents with G-HSD/hEDS completed MRT. Inclusion criteria were: (i) indication for outpatient MRT, (ii) considerable disability and fear of movement according to the expert opinion of the physician in rehabilitation medicine, (iii) age 12–21 years at the start of the treatment, (iv) chronic musculoskeletal complaints (≥ 3 months), and (v) joint hypermobility with a Beighton Score (BS) ≥ 6 (age of participants 12–17 years) or a BS of ≥ 5 (age of participants 18–21 years) (5, 18). Exclusion criteria were possible psychiatric disorders for which a psychiatric treatment is indicated and a medical (orthopaedic, rheumatic, or neurological) disease that can explain the severity of pain complaints.
To describe the population at baseline, data on sociodemographic variables (age, sex, education level, duration of pain, and school absence due to pain in the last year) were collected. Furthermore, height and weight were measured without heavy clothing and shoes. Body mass index was calculated as weight in kg divided by the square of height in m. Joint hypermobility was measured by a physician with a standardized protocol using the BS. The inter-rater reliability of the BS seems acceptable to be used in clinical practice (18). Psychosocial functioning was assessed with questionnaires regarding fear of pain (Fear of Pain Questionnaire-Child report; FOPQ-C), pain catastrophizing (Pain Catastrophizing Scale for Children; PCS-C) and depressive symptoms (Children’s Depression Inventory; CDI). The FOPQ-C, PCS-C and CDI have demonstrated good validity and reliability in children and adolescents (19–21).
Procedure
Participants in this study were included in 2 different ways. First, adolescents participated in the 2B Active trial (16). The purpose of this study was to evaluate whether MRT, including EXP, reduces functional disability in adolescents with CMP compared with care as usual. If adolescents with CMP had an indication for MRT, they were invited to participate in the study and received patient information. Adolescents younger than 18 years needed written approval from their parents and/or caregivers. The MRT for adolescents with G-HSD/hEDS consisted of a combined programme of physical training sessions and EXP sessions. A detailed description of the procedure of the trial is found elsewhere (16). Three out of 9 adolescents with G-HSD/hEDS were allocated to the MRT of combined physical training sessions and EXP sessions and, in this way, they also participated in the current study Secondly, after completion of the 2B Active trial in 2017 (17), treatment and measurement protocol according to 2B Active was implemented in usual care for adolescents with G-HSD/hEDS at Adelante/Maastricht University Medical Center+. In the period April 2017 to August 2019, an additional 11 adolescents with G-HSD/hEDS received MRT according to the protocol used in the 2B Active trial. Measurements were part of the regular care. To ask adolescents and their parents and/or caregivers for permission to use outcome of assessments for research purposes, they received an information letter and were asked to give informed consent. Adolescents younger than 16 years needed written approval from their parents and/or caregivers. After informed consent was given, the measurements were collected anonymously. Ethical approval for this study was granted by the Medical Ethics Committee Academic Hospital Maastricht/Maastricht University, the Netherlands (METC2018-0520).
All adolescents participated in a pre-treatment and a post-treatment assessment. Assessments of the 3 adolescents in the 2B Active trial were performed by an independent physiotherapist. Assessments for the additional 11 adolescents were performed by their treating physiotherapist. Finally, both data-sets were combined.
Multi-rehabilitation treatment
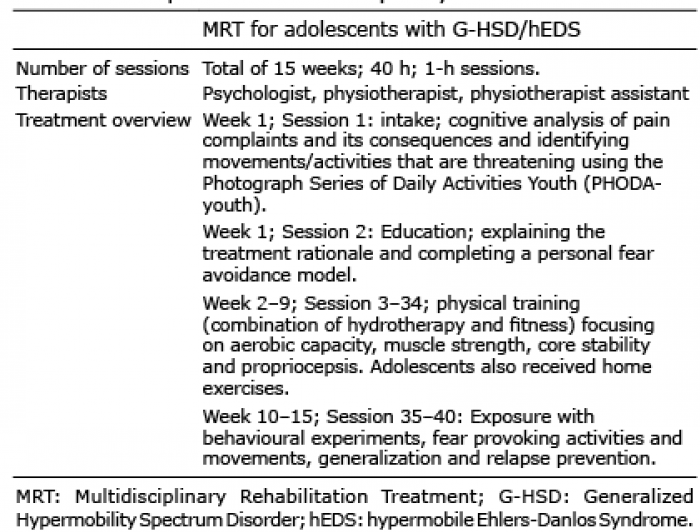
During the study intake the physician in rehabilitation medicine assessed the full medical history and current CMP-related complaints, disabilities and medication used. Afterwards the physician in rehabilitation medicine decided whether the adolescents were eligible for MRT, and monitored the treatment process. The MRT (total of 15 weeks) started with an intake and education session in the first week, provided by a skilled psychologist and physiotherapist. Subsequently, patients completed an 8-week physical training (2 h 2×/week) programme led by a physiotherapist and assistant physiotherapist. Thereafter, adolescents received an additional 6 sessions (1×/week) of EXP therapy provided by a skilled psychologist and physiotherapist. Table I provides a summary of the content of the MRT. Parallel during the MRT treatment, 3 parent meetings (in a group or individually) were offered to help parents facilitating their children with pain in learning to cope with pain (22). It was intended that both parents attend the sessions. Individual parent meetings were conducted when there were fewer than 3 parent couples available for the parent group. The physical training module focused on improving physical parameters, such as aerobic capacity, muscle strength, core stability and propriocepsis, for compensating the physical impacts of GJH. The EXP module used principles of classical conditioning and cognitive behavioural techniques to restore the normal pattern of daily functioning by reducing pain-related fear and catastrophic thinking, through exposing adolescents to fear-provoking daily life activities and movements (23). A detailed description of the MRT is found elsewhere (16).
Table I. Description of the multidisciplinary rehabilitation treatment
Primary outcome measure
The primary outcome was the Functional Disability Inventory (FDI). The FDI is a self-report measurement instrument for adolescents, which is used for measuring perceived difficulty in performing activities at school, at home and in recreational or social interactions. The instrument consists of 15 items rated on a 5-point scale (0=”no trouble” and 4=”impossible”). The FDI total score ranges from 0 to 60, with a higher score demonstrating greater disability. Scores ranging from 0 to 12 are classified as none or minimal disability, 13 to 29 as moderate disability, and scores ≥ 30 reflect severe disability (24). The FDI is a reliable and valid instrument to evaluate pain-related disability in adolescents (25).
Secondary outcome measures
Physical functioning. The level of physical functioning was determined by measuring motor performance, muscle strength, muscle strength endurance and physical activity level. For measuring motor performance, the single leg hop for distance (SLHD) was used. The adolescents were asked to jump as far as possible on a single leg, without losing balance. The distance was measured in centimetres from the toe at push-off to the heel at the place the adolescents landed. After one practice attempt, the greatest distance measurement of 3 valid hops with both sides was used for further analysis. The SLHD has demonstrated high intra-subject reliability (26).
To measure isokinetic muscle strength in knee extensors and flexors, the Biodex System 3 Pro dynamometer (Biodex Medical Systems, Shirley, NY, USA ) was used. The adolescent was invited to take place in an upright sitting position and the tested leg was stabilized with a fixation strap. The lever arm was attached to the adolescent’s lower leg by a padded cuff 2 cm proximal to the medial malleolus, and the axis of movement of the dynamometer was in line with the axis of movement of the knee flexion/extension. After one try-out attempt, 5 duplications of maximal voluntary concentric knee flexion and extension were measured at the angular velocity of 60°/s. Peak torque (PT; Nm) was assessed, and represents the highest muscular force output similar to one repetition maximum effort in isotonic, and represents the muscle’s maximum strength capability. PT/body weight is the PT normalized for body weight, used to standardize and compare scores in further analyses.
The same set-up as above (isokinetic muscle strength, Biodex System 3 Pro dynamometer) was used to measure isokinetic muscle strength endurance. After one try-out attempt, the adolescent had to perform 30 repetitions of maximal concentric knee flexion and extension, with an angular velocity of 240°/s. The test was carried out 60 s after the isokinetic test of 60°/s. Total work (J) is the work produced throughout the test and represents the muscle’s capability. The Biodex isokinetic dynamometer has been shown to be a reliable and valid measure (27).
The level of physical activity (PAL) during daily life was measured using a tri-axial accelerometer (AX3; Axivity, Newcastle, UK) attached to the waist using plaster (Tegaderm Film; 10 × 12 cm). The adolescents were instructed to remove the accelerometer during activities potential harmful for the device, such as contacts sports or swimming. In addition, all adolescents were asked to keep a diary of data interruption, such as removing the device and the reason for doing this. Furthermore, wake-up time and sleeping were noted. To be included as a valid measurement, a minimum of 3 weekdays with at least 10 h of recording and one weekend day with at least 8 h of recording had to be available during the 7-day monitoring period (28). Raw data processing was performed using Matlab (The Math Works Inc., Natick, MA, USA). An algorithm, based on the method that was used for the Actiwatch 7 (Philips, Netherlands), was designed to obtain activity counts from the raw data, resulting in one resultant acceleration signal. This signal was rectified and filtered using a high-pass filter at 3 Hz and a low-pass filter at 10 Hz. The highest recorded sample per second was selected and summed per minute (counts/min). Daily uptime was defined as the period between getting up and going to sleep (in min).
PAL was expressed as 3 quantities:
Total activity (TA) during uptime, determined by the total sum of counts during uptime.
Mean activity (MA) level during 24 h, which refers to the mean number of counts per min per day. Sleeping time is included in the total score.
Peak activity (PA) level, calculated as the highest number of counts achieved in 1 min per daytime wake period.
TA and PA measurements were calculated as a total and separately for the week and weekend days.
Perceived harmfulness (PHODA-youth).The Photograph Series of Daily Activities for youth (PHODA-youth) assessed perceived harmfulness. This consists of 51 age-specific photographs that had to be rated on a scale 0–10 (0=”not harmful at all” and 10=”extremely harmful”). The PHODA-youth consists of 3 subscales: activities of daily living and household (PHODA-ADL; 13 items), intensive physical activities (PHODA-PA; 27 items) and social activities (PHODA-SA; 11 items). The total score was calculated by summing all items (range 0–510) and subscale scores were calculated by summing the scores on all items in that subscale. Higher scores indicate higher levels of perceived harmfulness. The PHODA-youth has been demonstrated to be valid and reliable in adolescents with CMP (29).
Pain intensity (VAS). The visual analogue scale (VAS) consisted of a pre-measured line (100-mm) that ranges across a continuum from “no pain” to “worst pain imaginable”. The adolescents were asked to score 3 VAS scales: (i) current pain, (ii) the worst/most severe pain experienced in the last week, and (iii) the least pain experienced in the last week. The mean of these 3 VAS scores was calculated and used to express pain intensity in the analyses. The VAS demonstrated good reliability and validity in measuring pain intensity in children older than 8 years (30).
Statistical analysis
Data analysis was performed using the IBM Statistical Package for the Social Sciences (SPSS), version 25.0 (IBM Corp, Armonk, NY, USA). Due to the small sample size, normality of variables cannot be assumed and therefore non-parametric tests were used (31). Descriptive data of sociodemographic variables, anthropometric measurements and hypermobility were presented as median and interquartile range (IQR). Statistically significant inter-individual changes for functional disability, physical performance, perceived harmfulness and pain intensity were assessed using the Wilcoxon signed-rank test. Test statistics were presented by the corresponding z, the significance value (p), and an effect size (r). Effect sizes were calculated by dividing the z-score through the root of the number of observations. The effect size r was described indicating small effects from r ≥ 0.1 to r < 0.3, medium effects from r ≥ 0.3 to r < 0.5, and large effects from r ≥ 0.5. p-values less than 0.05 were considered statistically significant.
Descriptive analysis
Fourteen Caucasian adolescents (13 females, 1 male) participated in this study with a median age of 17.5 years (IQR 16.0–20.3). The median BS was 6 (IQR 6–7). At baseline, the median level of the FOPQ-C was 50 (IQR 34–61), which almost represents a high level of pain-related fear according to the norm (score ≥51) (19). The median level of the PCSC-C was 26 (IQR 17–34), meaning high levels of catastrophizing thoughts about pain according to the norm (high ≥ 26) (32). For depressive symptoms, the median level of the CDI was 19.0 (IQR 13–22), which indicates the adolescents were at risk for depression (cut-off point ≥ 16) (21). Baseline sociodemographic and anthropometric measurements were presented in Table II. One adolescent did not complete both PHODA measurements and the post-treatment FDI. Four adolescents did not complete the PAL measurements due to allergic reactions from plaster (n = 2) and unwilling to wear the accelerometer (n = 2) and one of them also did not complete the post-treatment PHODA. A 6th adolescent did not meet the criteria for a valid post-treatment PAL registration; instead, a minimum of 3 weekdays with at least 10 h of recording only one valid weekday was measured.
Table II. Baseline sociodemographic and clinical characteristics of the study sample (n = 14)
Outcomes of multidisciplinary rehabilitation treatment
Compared with the pre-treatment level of disability (median 24) adolescents with G-HSD/hEDS showed significant improvements at post-treatment (median 8.0), z = –3.18, p < 0.01, r = –0.61. The individual scores of the FDI are presented in Fig. 1.
Fig. 1. Reduction in individual Functional Disability Inventory (FDI) scores of the adolescents with generalized hypermobility spectrum disorder/hypermobile Ehlers-Danlos syndrome (G-HSD/hEDS) (n = 13).
Regarding secondary outcomes, significant improvements were found in post-treatment motor performance (z = –3.30, p < 0.01, r = –0.62), knee extension muscle strength (z = –3.30, p < 0.01, r = –0.62), knee flexion muscle strength (z = –3.30, p < 0.01, r = –0.62), knee extension muscle strength endurance (z = –2.35, p < 0.05, r = –0.42) and knee flexion muscle strength endurance (z = –2.35, p < 0.05, r = –0.42) compared with pre-treatment. Analyses of the non-preferred leg were not presented, but results were comparable to outcomes, as presented, of the preferred leg. There were no statistical differences found in all post-treatment PAL conditions compared with pre-treatment PAL conditions. Regarding perceived harmfulness, post-treatment significant improvements were found in the total score (z = –3.06, p < 0.01, r = –0.61) and all subscales (PHODA-ADL: z = –2.67, p < 0.01, r = –0.52; PHODA-PA: z = –3.06, p < 0.01, r = –0.61; PHODA-SA: z = –2.80, p < 0.01, r = –0.54). Furthermore, post-treatment significant improvements in self-reported pain intensity were found (z = –2.79, p < 0.01, r = –0.51) (Table III).
Table III. Results of the primary and secondary outcomes for all time-points of measurements
This study demonstrated that adolescents with G-HSD/hEDS show significant improvements in functional disability following MRT. These improvements were represented as a large effect size (r > 0.5). According to the norm of the FDI, the pretreatment level of 24 points out of 60 is classified as moderate disability (score 13–29), while the post-treatment median level of 8 points out of 60 represents no/minimal disability (score 0–12) (24). Thus, after MRT adolescents with G-HSD/hEDS were able to function quite well. The decrease in functional disability (16 points) can be seen as a clinically relevant change (FDI reduction of ≥ 7.8 points) (33).
Furthermore, MRT showed improvements in pain intensity. The reduction in pain (63%) is remarkable, since MRT focused on reducing the level of disability and pain reduction was not the main goal. This finding could be attributed to improvements in propriocepsis and deconditioning after completing the physical training sessions (8). The results showed a 63% reduction in pain intensity, which is considered as a clinically significant improvement for average pain intensity (34).
In addition, MRT showed post-treatment improvements in most subcategories of physical functioning, such as muscle strength, muscle strength endurance, and motor performance which is determined by coordination, balance and joint stability. These improvements in the physical parameters are hypothesized to be important for compensating the physical impacts of GJH. In contrast to the improvements in the level of functioning, the level of physical activity in daily life remains similar. A possible explanation for this finding could be that adolescents with G-HSD/hEDS perceive their daily life activities as improved, which is reflected by a decrease in the perceived difficulty of performing activities at school, at home and in recreational or social interactions. However, the objective measurements presented as total counts did not confirm these beliefs. Finally, MRT showed improvements in pain-related fear, measured as perceived harmfulness. This reduction might be due to the fact that pain and fear share some common brain networks and therefore a decrease in pain intensity might also lead to a decrease in pain-related fear (35). The decrease in pain-related fear might also be explained due to clarification of the condition and exposing adolescents to fear-provoking daily life activities and movements.
It seems remarkable that despite the small sample size of this study, significant improvements were found in most of the outcome variables with medium-to-large effects. Earlier studies in children and adults with G-HSD/hEDS who received physical training only, showed comparable results regarding improvements in pain intensity (36, 37). In addition, a RCT study showed that a physiotherapist-prescribed exercise programme for children with G-HSD/hEDS and hypermobile knees led to improvements in knee muscle strength, pain reduction and psychosocial factors (38). However, our population had considerable disability and fear of movement, and therefore MRT was indicated. Furthermore, the current findings regarding pain intensity and physical functioning were also in line with results of children aged 5–16 years with G-HSD/hEDS receiving a multidisciplinary intervention with both physiotherapy and occupational therapy (39). However, no specific attention towards psychological symptoms, such as anxiety, was conducted, the main outcome measure was child-reported pain and no specific parent guidance was part of the intervention. Another study with combined physical and cognitive-behavioural therapy showed comparable results regarding improvements in performance of daily life activities, increased muscle strength and endurance and reduced kinesiophobia (40). However, the participants in the study of Bathen et al. (40) were exclusively female adults, were hospitalized for 2.5 weeks as part of the treatment, and the cognitive-behavioural approach aimed at raising awareness of thought and patterns in life. To our knowledge, our study is the first interventional study focusing on outpatient rehabilitation treatment for adolescents with G-HSD/hEDS to investigate the outcome of MRT, containing a combination of physical training sessions and EXP sessions, on the level of disability, physical functioning, pain-related fear and pain intensity.
This study has some limitations, which should be considered. The first limitation is the pre-test post-test design with the lack of a control group. Overall, this limits our ability to infer causation of any improvements observed to participation in MRT. Non-specific factors, such as expectancy, also cannot be controlled in a single-group study design and may play an important role in the beneficial results found in this study. A second limitation is the small sample size in this study. Although we intended to perform a subgroup analysis, the treatment effect in a subgroup of adolescents with G-HSD/hEDS in the 2B Active trial, the number of patients needed was not attained. In the current study, we are able to present information on the progress of adolescents with G-HSD/hEDS following MRT. A third limitation is the pre-post treatment assessment by the treating physiotherapist during the usual care, which could be prone to bias. To limit the bias, a measurement protocol was used with prescribed steps to ensure the same procedure and order of measurements, which was used in the 2B Active trial. The fourth limitation is the relatively large number of analyses performed. Therefore, there is an elevated risk of a type I error. However, 16 out of the 19 analyses were considered significantly different, and even lowering α still leads to mainly significant outcomes.
The results of this study are promising and could have clinical implications. Many authors propose MRT for adolescents with G-HSD/hEDS (14, 15, 39, 40). In consideration of the multidimensional and diversity of symptoms and conditions the current study suggests that a multidisciplinary approach is recommended. However, our findings are based on a small sample size without a randomized controlled group and, as a result, this interpretation should be treated with caution. Therefore, further studies are needed using a randomized design with larger sample sizes, including a long-term follow-up evaluation to investigate the effectiveness of MRT in adolescents with G-HSD/hEDS. Furthermore, in this study we did not include measures of multi-systemic dysfunction and fatigue, which are important constructs of functional disability (10). In particular, multi-systemic dysfunction was related to a deteriorating level of functioning. Therefore, it might be advisable to include these constructs in further studies and clinical practice in order to identify adolescents with G-HSD/hEDS who are at risk of further decline in functioning.
Conclusion
In adolescents with G-HSD/hEDS, MRT leads to a significantly and clinically relevant improvement in func- tional disability. Furthermore, improvements in physical functioning, perceived harmfulness and pain intensity occurred after MRT. Although the results of this MRT in rehabilitation care for adolescents with G-HSD/hEDS are promising, these findings should be replicated in a study with a randomized design.
The authors would like to thank the participating adolescents, Richard Geers Ing. for processing the raw data of the accelerometer and the treatment team for offering the intervention and recruiting and measuring the adolescents. The idea for this work was funded by Fonds Nuts Ohra, Stichting Vooruit and Adelante.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize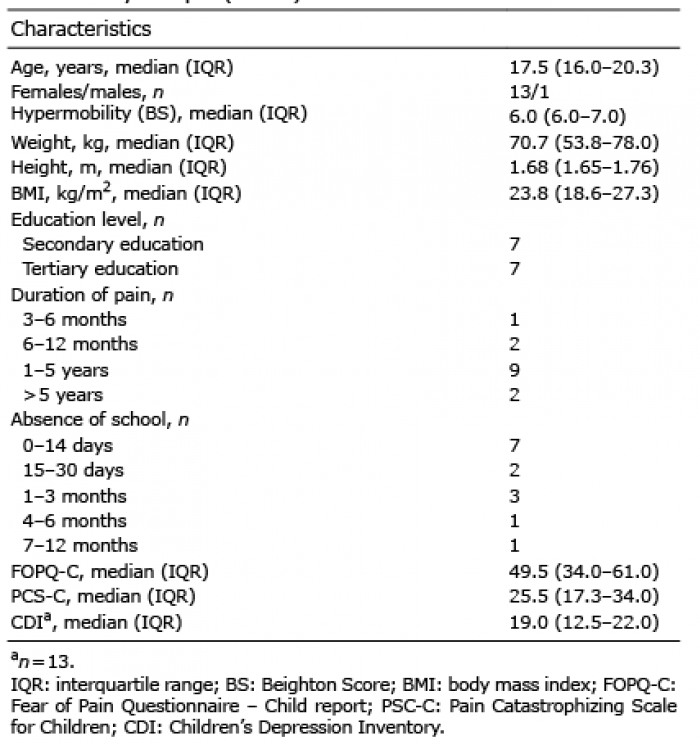 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize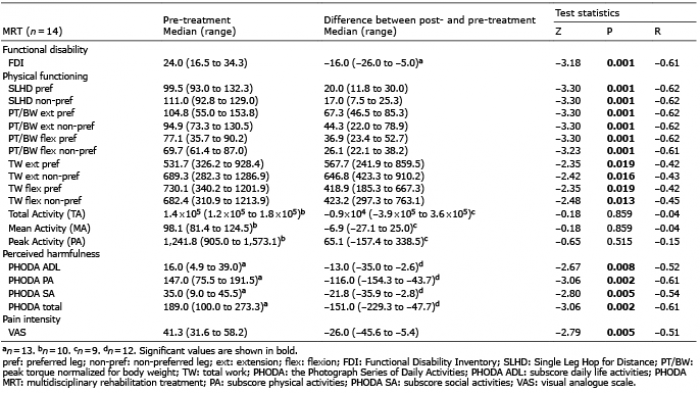 Click to show fullsize
Click to show fullsize