
1Department of Nephrology, Japanese Red Cross Nagoya Daiichi Hospital, Nagoya, Japan
2Department of Nephrology, Kaikoukai Josai Hospital, Nagoya, Japan
3Department of Rehabilitation, Kaikoukai Josai Hospital, Nagoya, Japan
4Department of Health Fitness Programmer, Nagoya Kyoritsu Hospital, Nagoya, Japan
Background: Physical impairment or frailty due to sarcopaenia is common in patients with chronic kidney disease and those receiving dialysis. This study examined the association between muscle weakness and kidney function in Japanese patients with chronic kidney disease.
Methods: A total of 23 stable outpatients were enrolled in the study. Several indices were used to assess muscle function; hand grip strength, isometric knee extension strength, Timed Up and Go test (TUG), and the short physical performance battery. The relationships between these indices and estimated glomerular filtration rate (eGFR) as a measure of kidney function were analysed statistically.
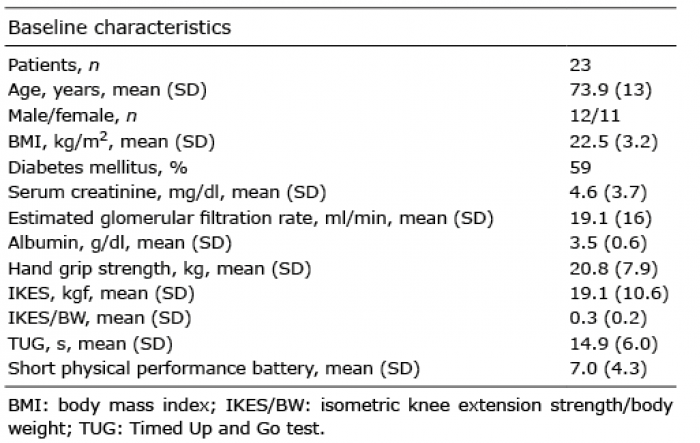
Results: Patients’ characteristics were as follows: mean age 73.9 years (standard deviation (SD) 13); 12 males, 11 females; body mass index (BMI) 22.5 kg/m2 (SD 3.2); serum creatinine (sCr) 4.6 mg/dl (SD 3.7); estimated glomerular filtration rate (eGFR) 19.1 ml/min (SD 16). Their physical performance indices were: hand grip strength 20.8 kg (SD 7.9); isometric knee extension strength 19.1 kgf/kg (SD 10.6); TUG 14.9 s (SD 6.0); and short physical performance battery score 7.0 (SD 4.3). Multiple regression analysis adjusted for age revealed significant associations between isometric knee extension strength/body weight and eGFR (F [2,19] = 8.38, p = 0.002) and TUG and eGFR (F=4.98 [2,18], p = 0.02).
Conclusion: Deterioration in muscle function or maintenance of posture is associated with chronic kidney disease.
Key words: frailty; sarcopaenia; physical impairment; hand grip strength; isometric knee extension strength; Timed Up and Go test; chronic kidney disease.
Accepted Dec 20, 2018; published Mar 12, 2019
JRM-CC 2019; 2: 1000013
Correspondence address: Hideaki Ishikawa, Department of Nephrology, Japanese Red Cross Nagoya Daiichi Hospital, 453-8511 Nakamuraku Nagoya Aichi, Japan.
Frailty due to sarcopaenia is common in patients with chronic kidney disease and those receiving dialysis. However, there is limited information available on the relationship between kidney function and such comorbidities in the Japanese chronic kidney disease population. Such comorbidities are a potential risk for poor physical activity, disability, falls, more frequent hospitalization and, especially, increased mortality. This study included a total of 23 stable outpatients, and measured several indices of muscle function, such as hand grip strength, isometric knee extension strength, Timed Up and Go test, and short physical performance battery. Relationships between these indices and kidney function, assessed by the estimated glomerular filtration rate, were then examined. Deterioration in muscle function and maintenance of posture were found to be associated with chronic kidney disease.
Although patients with chronic kidney disease (CKD) may develop physical impairment due to frailty, the detailed relationship between frailty and CKD is not fully understood (1). It has been reported that chronic inflammation or protein-energy wasting (2) in patients with CKD may play a major role in the development of age-related muscle atrophy, diagnosed as sarcopaenia (3).
Sarcopaenia may cause functional limitations, such as slow or unstable walking. These changes are followed by development of disability and the patient becoming physically inactive. The combination of these symptoms leads to “frailty”, or physiological decline (4). Sarcopaenia should therefore be recognized as the first step in the development of frailty.
Frailty is also a potential risk factor for frequent hospitalization and increased mortality (5). It should also be recognized that different types of frailty or sarcopaenia are prevalent in geriatric patients (6). In general, a proportion of CKD patients in Japan are elderly (7) and therefore it is important to evaluate physical impairment due to muscle loss in this population. Previous studies have shown that the GFR appears to be an important mediator of fragility in patients with CKD, with an estimated glomerular filtration rate (eGFR) <45 ml/min associated with an increased likelihood of becoming frail (8, 9).
It has also been reported that renal sarcopaenia might be characterized by loss of skeletal muscle strength (10). Another study revealed that uraemic toxins might be associated with CKD-related skeletal muscle atrophy (11).
Despite the need to be aware of this situation, there is currently no consensus on how to assess physical impairment due to sarcopaenia in Japanese patients with CKD. Previous studies have shown that there are several feasible and reliable tests that are useful for identifying sarcopaenia in these patients, such as hand grip strength (HGS), isometric knee extension strength (IKES), and the Timed Up and Go test (TUG) (12, 13).
We therefore measured these clinical indices in our CKD patients, with safety being assured by the help of healthcare providers, including doctors, nurses, physical therapists, nutritionists, and a health fitness programmer. The purpose of the study was to determine whether changes in muscle function were associated with impaired kidney function in Japanese patients with CKD.
This study demonstrated clearly that deterioration in muscle function or maintenance of posture was associated with CKD in Japanese patients. This finding should help to increase awareness among nephrologists of the importance of critical comorbidities, such as physical impairment, in the Japanese CKD care setting.
The study design was cross-sectional. CKD was defined as an estimated glomerular filtration rate (eGFR) <60 ml/min/1.73 m2 (14). Patients without apparent serious complications, such as paralysis due to cerebrovascular disease or intermittent claudication secondary to obstructive arteriosclerosis, were not eligible for the study.
Patients from Kaikoukai Josai Hospital, Japan were carefully diagnosed using the inclusion criteria described above and 23 patients were enrolled in the study. The study was approved by the ethics committee of Kaikoukai Josai Hospital, with informed consent being obtained from all participants prior to enrolment.
Hand grip strength. After explaining the procedure to each patient HGS was measured in kgf (15). Patients either sat on a chair or were bedridden, with their arms by the side of their body and one side of forearm at a flexion angle of 90° and the elbows unsupported (12, 16). The maximum of 3 consecutive measurements in the non-dominant arm was recorded using a mechanical hand grip dynamometer (TKK 5401 hand grip dynamometer, Takei Scientific Instruments, Nigata, Japan), registered to the lowest kilogram (kgf). A brief pause was taken between measurements. Patients used their dominant hand when they were unable to perform the HGS test with their non-dominant hand. Exclusion criteria were upper limb deformities or an incapacity to perform the HGS measurements. The maximum data for each patient were used in the analysis.
Isometric knee extension muscle strength. Isometric knee extension muscle strength (IKES) was measured in kgf (kilograms force) using a mobile MT-100, hand-held dynamometer with a belt (Sakai Medical Co. Tokyo, Japan) (15). Knee extension strength was measured using a Biodex isokinetic dynamometer (IKD) with the participants seated and stabilized by straps in an IKD test chair with their knees at 90°. The measurements were repeated 3 times. The ratio of maximum score to body weight (kgf /BW) was used in the statistical analysis.
Timed Up and Go test. The TUG is used to evaluate basic functional mobility. During the test, the participants get up from a chair, walk 3 m, make a 180° turn, return to the chair, and sit down (15). The time (in s) taken to accomplish the test was recorded. The best of 3 measurements was used in the analysis.
Short physical performance battery. The SPPB has emerged as one of the most promising tools for evaluating functional capability and providing a measure of the biological age of an elderly individual. It is an objective tool for measuring the physical performance status of the lower extremities (17). The SPPB is based on 3 timed tasks: standing balance, walking speed, and chair stand tests. The timed results of each subtest are rescaled according to predefined cut-off points to calculate a score ranging from 0 (worst performance) to 12 (best performance). The best score of 3 measurements was used in the analysis.
All the data were expressed as mean and standard deviation (SD), unless otherwise specified. All the statistical analyses were carried out using R version 3.2.4 software (18). A p-value < 0.05 was considered statistically significant.
The data for the 23 enrolled patients are summarized in Table I. The mean age was 73.9 (SD 13) years, which indicates that a large number of the participants were elderly. Mean serum creatinine level was 4.6 (SD 3.7) mg/dl and mean eGFR 19.1 (SD 16) ml/min, indicating the majority of patients were classified as CKD stage 4. More than half of the patients had been diagnosed with diabetes mellitus. There was no significant correlation between both HGS and eGFR or age (r =0.3, p = 0.21; r =0.1, p = 0.56), respectively. Although there was no significant correlation between IKES/BW and age, the correlation between IKES/BW and eGFR was statistically significant (r =0.5, p = 0.007).
Table I. Baseline characteristics of the patients enrolled in the study
The results of the multiple regression analysis are shown in Table II. It was hypothesized that the variables that correlated with IKES/BW, such as eGFR and age, may be predictors of sarcopaenia or frailty. As a result, the model was a significant predictor for IKES/BW (F [2,19] = 8.38, p = 0.002) and explained 47% of the variability in IKES/BW. While eGFR contributed significantly to the model (β = 0.006, p = 0.00068), age did not (β = 0.0003, p = 0.94) (Table IIA).
Table II. (A) Multiple regression analysis showing the association between isometric knee extension strength/body weight (IKES/BW) and predictive factors, such as glomerular filtration rate (eGFR) and age. (B) A similar analysis between Timed Up and Go test (TUG) and predictive factors, such as eGFR and age
Multiple regression analysis was also carried out to investigate whether eGFR and age were significant predictors of the participants’ TUG score. The results indicated that our model explained 35% of the variance and was a significant predictor of TUG score (F = 4.98 [2,18], p = 0.02). As shown in Table IIB, although eGFR contributed significantly to the model (β = –0.2, p = 0.02), age did not (β = 0.4, p = 0.05).
There is increasing evidence that sarco-paenia or frailties are prevalent in patients on maintenance dialytic therapy (7, 18). There is also evidence that these conditions may be associated closely with deterioration in muscle function and that several clinical factors, such as ageing, protein-energy wasting, and lower activities of daily living (ADL), can cause muscle weakness in dialysis patients (19, 20). In addition, frailty or sarcopaenia may increase the risk for hospital admission and mortality (6), and therefore clinical research on the assessment of physical performance related to muscle function in patients with CKD is extremely important. Despite this situation, there is no consensus on the definition of sarcopaenia or frailty in Japanese patients. We therefore carried out further analysis of our previously published data on a Japanese population (21). As shown in Table I, the patients with CKD in our study were elderly and, despite having a mean CKD stage of approximately 4, indicating advanced CKD disease, they had no major symptoms related to the uraemic syndrome, such as anorexia, nausea, respiratory distress, or fatigue. However, the mean HGS of the patients was in the sarcopaenic range. In addition, IKES/BW, a reliable parameter of lower limb muscle function, was marginally decreased. It was also observed that the mean score of both TUG and SPPB were below the cut-off values used in previous studies (22).
Taken together, these results suggested that the patients with CKD in the current study had impaired physical functions, including mobility and performance capacity and physical activity. Thus, we investigated the association between eGFR and muscle function indices, such as HGS and IKES/BW. As shown in Fig. 1, there was a significant correlation between IKES/BW and eGFR, indicating that muscle strength of the lower limbs was associated with impaired kidney function. On the other hand, no significant association was found between HGS and eGFR. Interestingly, contrary to our expectations, there was no significant correlation between ageing and muscle function of the lower limbs.
Fig. 1. Correlation analysis of isometric knee extension strength/body weight (IKES/BW) and estimated glomerular filtration rate (eGFR) ml/min (r = 0.5, p = 0.007), IKES/BW and age (r = 0.1, p = 0.51), hand grip strength (HGS) (kgf) and eGFR ml/min (r = 0.3, p = 0.21), and HGS and age (r = 0.1, p = 0.56).
To determine whether impaired kidney function was an independent risk factor for the deterioration of muscle strength of the lower limbs, multiple regression analysis was used to predict IKES/BW based on age and eGFR. As shown in Table IIA, a significant equation was found, i.e. F (2,19) = 8.38, p = 0.002 with an R2 of 0.47. It was also confirmed that eGFR was a predictor of TUG score (F = 4.98 [2,18], p = 0.02, R2 = 0.35) (Table IIB). Both of these analyses confirm that eGFR is a stronger predictor than age for disability of physical function. It was already known that both IKES/BW and TUG were associated closely with lower limb muscle function.
Although it is possible that sex may affect the development of sarcopaenia (23, 24), similar results were obtained in data adjusted for sex (data not shown).
In summary, based on these analyses, it may be speculated that impaired physical functions, especially lower limb muscle function, developed following deterioration of kidney function in the participants in the current study.
There were several limitations to this study. First, despite the cross-sectional design, the study was carried out in a single centre and the sample size was small. Secondly, the patients were mostly elderly, and therefore the results could be different in a younger generation. Thirdly, we did not take other clinical risk factors into account, such as medications considered to be related to sarcopaenia (25), daily diet or exercise habits. Despite these limitations, currently there is no consensus or clinical evidence regarding sarcopaenia or frailty in the Japanese population with CKD. We therefore consider that our results may help to draw the attention of healthcare providers of patients with CKD to these serious comorbidities.
In conclusion, this study found a significant association between impaired kidney function and deterioration in muscle strength, especially the lower limbs, in Japanese patients with CKD. The results are consistent with those of a previous study (26). It is therefore necessary to be aware of the potential risk of sarcopaenia or frailty, even in stable outpatients (3). Thus, integration of effective physical therapies, nutritional support, and other healthcare services, such as rehabilitation in daily life, is worth considering in order to prevent or improve this situation (27–29).
Availability of data and materials. The datasets used and/or analysed during the current study are available from the corresponding author on request.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize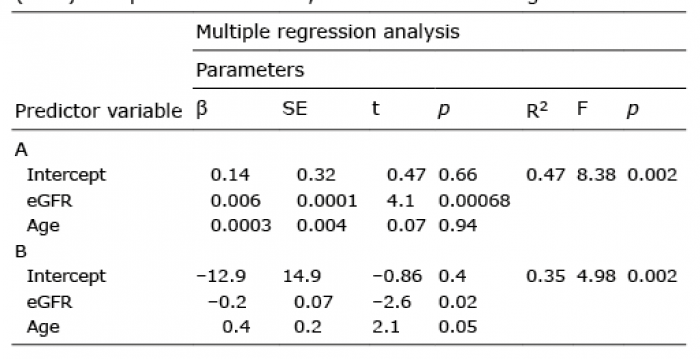 Click to show fullsize
Click to show fullsize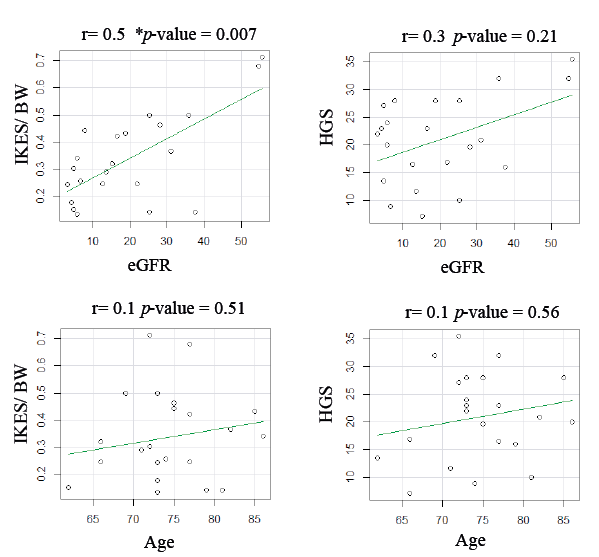 Click to show fullsize
Click to show fullsize