
From the 1Radboud University Medical Center, Nijmegen, Donders Institute for Brain, Cognition and Behaviour, Department of Rehabilitation, 2Department of Rehabilitation, Sint Maartenskliniek, 3Research Department, Sint Maartenskliniek, 4Department of Orthopaedics, Sint Maartenskliniek, Nijmegen, The Netherlands, 5Department for Foot and Ankle Surgery, Orthopedic Clinic of the Hannover Medical School, Hannover, Germany, 6Klimmendaal Rehabilitation, Arnhem, The Netherlands and 7Department of Orthopaedic Surgery and Traumatology, Inselspital, Bern University Hospital, University of Bern, Bern, Switzerland
Gait impairments in people with Charcot-Marie-Tooth disease are the combined result of ankle-foot deform ities, muscle weakness, and somatosensory impairments. People with Charcot-Marie-Tooth disease often experience pain and difficulties when walking, especially barefoot. They also trip and fall frequently and have a lower than normal gait speed and distance. Because these gait impairments and related complaints are disabling, clinical management aimed at improving gait is important. Management involves both conservative and surgical treatment options, each with limited scientific evidence. However, a treatment algorithm that describes both conservative and surgical treatment options is currently lacking. This study sets out a step-wise treatment algorithm, based on evidence, if available, and otherwise reflect ing practice-based experience. The treatment algorithm will be of value in daily clinical practice, and will serve as a template for future research.
Key words: Charcot-Marie-Tooth disease; gait; rehabilitation; surgery.
Accepted Mar 29, 2021, Epub ahead of print Apr 21, 2021
J Rehabil Med 2021; 53: jrm00194
Correspondence address: Jorik Nonnekes, Radboud University Medical Centre, PO Box 9101, 6500 HB Nijmegen, The Netherlands. E-mail: jorik.nonnekes@radboudumc.nl
Doi: 10.2340/16501977-2831
Treatment of gait impairments in people with Charcot-Marie-Tooth disease is crucial, because it is a source of great disability. However, many clinicians find it difficult to treat these gait impairments in their daily clinical practice. This challenge is compounded by a lack of clear treat ment protocols that take the whole spectrum of treat ment options into account. As a result, there is wide variation in clinical practice. To address the widely felt need for a treatment algorithm, we present here a step-wise approach to the management of gait impairments in patients with Charcot-Marie-Tooth disease.
Charcot-Marie-Tooth disease (CMT), is a group of inherited polyneuropathies characterized by slowly progressive distal muscle weakness and distal somatosensory impairments (1). These symptoms are the result of axonal degeneration or demyelination of the peripheral nerves, depending on the type of disorder (2). In addition, due to distal muscle weakness, hand and feet deformities emerge over time in most people with CMT (3). Gait and balance impairments are common and disabling in people with this disorder, and are considered the combined result of ankle-foot deformities, muscle weakness, and somatosensory impairments. Patients often complain about pain when walking (typically in the plantar metatarsal region and at the lateral border of the foot) with or without pres sure sores, and about difficulties walking barefoot. They also tend to frequently trip and fall, and demonstrate a lower gait speed and walking distance than their healthy age-matched peers. Furthermore, their gait requires enhanced attention, leading to problems with dual-task performance when walking. Due to progression of the disorder, some patients become unable to walk (4). Gait and balance impairments frequently hamper full participation in society, and impact nega tively on the quality of life of affected individuals.
Hence, treatment of gait and balance impairments in people with CMT is important. Clinical management aimed at gait improvement in people with CMT is, however, challenging. Both conservative and surgical treatment options exist, but scientific evidence is inconclusive for most approaches. Surgical treatment guide lines have been published (5–8), but guidelines that combine both surgical and conservative approaches are lacking. Because the degree of somatosensory impairment, muscle weakness, and type and severity of ankle-foot deformities differ between patients, a therapeutic algorithm should not only combine different treatment options, but also facilitate a personalized approach.
This viewpoint paper, presents a step-wise clinical algorithm for the treatment of gait impairments in people with CMT. This treatment algorithm can be applied to all types of CMT. The algorithm describes both conservative and surgical interventions, allows a personalized approach, and is based on evidence when available, or otherwise reflects practice-based experience. Importantly, the focus is on the management of gait impairments in adults and adolescents from skeletal maturity onwards (girls and boys from the ages of, on average, 12 and 14 years, respectively), not on children with CMT who are still developing.
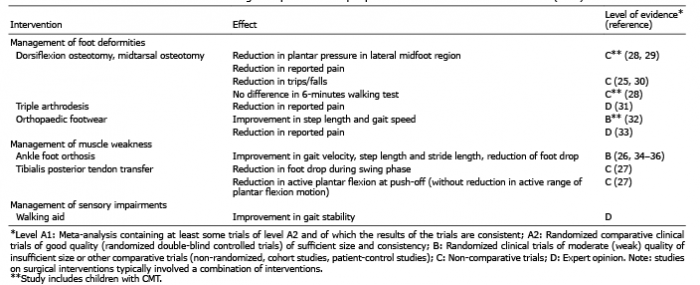
PubMed, CINAHL and Embase were searched for relevant articles published in English, German or Dutch from database inception to January 2020. Potential papers were identified with the terms “Charcot-Marie-Tooth Disease” or “Foot” or “Ankle”. Papers were included when a conservative or surgical treatment was described. Relevant studies were classified by level of evidence, based on study design; studies with the highest level of evidence for each treatment option are shown in Table I. Using this scientific evidence, and our practice-based experience, a step-wise treatment algorithm was created, as decribed below.
Table I. Level of evidence of interventions for gait impairments in people with Charcot-Marie-Tooth disease (CMT)
From impairments to gait limitations
Impairments in people with CMT can be categorized into 3 groups: (i) ankle-foot deformities, (ii) muscle weakness, and (iii) somatosensory impairments. These impairments result in primary, secondary and compensatory changes in the gait pattern (Fig. 1). In a small subgroup of patients, hip dysplasia may occur (6–8% of cases), which may further impact the gait pattern (9).
Fig. 1. Impairments in people with Charcot-Marie-Tooth disease can be categorized into 3 groups (lefthand column). These impairments result in primary, secondary and compensatory changes in gait pattern (righthand column). Compensatory changes in gait pattern are depicted in a dotted box.
Ankle-foot deformities
The most characteristic foot deformity is equinus of the first metatarsal bone, leading to pes cavus. The more prominent and rigid the plantarflexed position of the first metatarsal becomes, the more it will impact on the position of the foot during standing and walking. Ultimately, rigid metatarsal-I equinus deformity forces the hindfoot into varus tilt during loading. Hindfoot varus reduces ankle stability in the frontal plane, with the risk of ankle sprain and subsequent falls during walking. Moreover, pes varus will increase the plantar pressure on the lateral edge of the foot, resulting in pain and skin problems (e.g. callus formation and ulcers). In the long-term, varus deformity of the hindfoot may become rigid, resulting in a structural pes cavovarus. Such a rigid varus deformity further reduces ankle stability in the frontal plane, and increases lateral foot pressure and fall risk. To minimize the risk of ankle sprain, patients frequently walk wide based, and with increased homolateral trunk flexion during the single-support phase of gait. This compensatory trunk movement reduces the external varus moment at the hindfoot, but results in loss of gait efficiency, and may lead to secondary complaints of the musculoskeletal system, for example lower back pain.
In most patients, another characteristic foot deformity is observed, i.e. the emergence of claw toes (which is related to decreased function of intrinsic muscles of the foot). During normal gait, the foot winds over the heads of the metatarsal bones, while contraction of the calves provides a push-off. Due to claw toes, this winding is hampered and painful, resulting in reduced “push-off” power, which is often compensated by a stronger “pull-off” movement generated by the hip flexors.
In some patients, limited passive range of motion at the ankle (talocrural) joint is seen in addition to forefoot and hindfoot deformities. Shortening of the calf muscles may result in equinus deformity at the ankle joint. Due to pes equinus and forefoot cavus, the so-called ankle plantarflexion – knee extension couple emerges, which predisposes to knee hyperextension during plantigrade loading (10). This may result in difficulties during roll-off and push-off and, in the long-term, increases the risk of secondary complaints, such as knee pain. Although pes cavovarus deformity is most common in people with CMT, pes planovalgus can also be seen. This seems particularly prevalent in patients with rapid disease progression and pronounced muscle weakness (5).
Muscle weakness
Weakness of the ankle dorsiflexors results in a foot drop during the swing phase of gait, which is usually compensated by increased hip flexion (see Fig. 1). During loading, mild-to-moderate weakness will lead to rapid plantarflexion movement after heel contact (accelerated first rocker), whereas more pronounced weakness of the dorsiflexors will result in a midfoot or forefoot landing. When there is also weakness of the plantarflexors, this may result in excessive knee flexion during the stance phase of gait, as the calf muscles are the main stabilizers of the knee joint during midstance (10). Some patients may control excessive knee flexion by prolonged activation of the quadriceps (mainly the vasti), but others may compensate for this flexion tendency by adopting knee hyperextension during the early stance phase of gait. A limited ankle dorsiflexion range of motion (still allowing a plantigrade foot position) may sometimes be beneficial to prevent excessive knee flexion in the presence of calf muscle weakness. During the late stance phase of gait, calf muscle weakness will result in reduced push-off power, which adds to the loss of push off due to claw toes and causes an even greater necessity for compensatory pull-off power by the hip flexors (11).
Somatosensory impairments
Sensory impairments typically lead to loss of proprioception from the joints in the ankle and the foot and loss of exteroception from the plantar foot sole. Both sources of sensory input are essential for normal postural control. Thus, somatosensory loss is likely to cause postural imbalance. Indeed, posturographic studies have shown that people with CMT tend to show increased body sway compared with healthy controls, particularly in the case of visual deprivation (12). Apparently, their balance control is characterized by an increased dependence on visual input. Thus, patients may find it difficult to stand and walk in the dark, in poorly illuminated environments, or in any other situation where visual input is limited. To compensate for their somatosensory impairments, patients typically walk with a widened base of support and tend to visually “anchor” to their environment. In addition, somatosensory impairments have been suggested to play an essential role in the problems that people with CMT have when making fast gait adjustments to sudden changes in the support surface (13). These problems limit their gait adaptability to complex daily life circumstances and may require a higher level of attention while walking compared with individuals without impairments.
Assessment of gait limitations
Assessment of gait in people with CMT starts with history taking, followed by clinical examination, including observation of the gait pattern. History taking is particularly important to evaluate the complaints and impairments experienced by the patient (i.e. the presence of pain, pressure sores, inability to walk barefoot, reduced walking distance, frequent falls, or perceived postural instability) as well as the impact of these complaints and impairments on activities of daily living. During clinical examination, the location and severity of muscle weakness, somatosensory impairment, and foot deformity should be assessed. In addition, passive range of motion of the forefoot, hindfoot and ankle joint should be assessed separately. It may be difficult to determine whether hindfoot varus during loading is primarily due to rigid metatarsal-I equinus (flexible hindfoot varus) or also due to rigid varus deformity of the hindfoot itself. In these cases, the Coleman block test can help to evaluate the impact of a rigid plantarflexed first metatarsal (14). This test requires the patient to place the heel and lateral aspect of the foot on a wooden block (2–4 cm thick) while standing, allowing metatarsal-I to make free plantarflexion. If then the hindfoot is corrected to a neutral position, varus deformity during loading is primarily due to the equinus deformity of the first metatarsal.
Clinical examination is completed by observation of stance and gait. Observation of standing posture in the sagittal plane focuses on whether a plantigrade position of both feet can be maintained with the knees, hips, and trunk in a neutral position. If not, this might be indicative of structural equinus deformity of the forefoot (pes cavus) and/or the ankle (pes equinus). Observation of standing posture in the frontal plane should focus on the degree of varus deformity at the hindfoot and the impact thereof on stance width and varus load on more proximal joints, in particular the knees. To properly observe the gait pattern, the patient needs to walk along a trajectory of approximately 10 m with and without footwear and/or orthosis (10, 15). Ideally, a video system is available to evaluate the gait pattern offline and in slow motion to be able to focus on key characteristics, such as foot strike during initial contact, ankle rockers, knee stability during midstance, foot clearance in swing phase, step length and symmetry. Especially when surgical treatment options are considered, the gait pattern should be assessed more profoundly using 3-D instrumented gait analysis, including foot pressure measurements and surface electromyography, to quantify ankle and knee kinematics (e.g. ankle-foot roll off), kinetics (e.g. dynamics of ground reaction forces and foot pressure distribution), and compensatory (prolonged) muscle activation (e.g. of the knee extensors).
Clincal management of gait impairments
After proper assessment of the impairments that impact on the individual gait deviations, clinical management should focus on treating, or compensating for, these impairments. To this end, a hierarchical approach to the management of gait deviations in people with CMT is proposed, starting with the treatment of ankle-foot deformities, followed by provision of support to weakened muscles, and ending by addressing compensation strategies for somatosensory impairments (see Fig. 2). Adequate treatment of ankle-foot deformities is considered key, given their profound influence on postural and gait control in addition to their effect on pain and dependence on adapted footwear. As shown in Table I, scientific evidence for both surgical and conservative interventions is sparse due to the lack of controlled studies. Nevertheless, clinical experience with both surgical and conservative treatment options is extensive and generally positive, if performed by a dedicated and experienced multidisciplinary team.
Fig. 2. Stepwise treatment algorithm for gait impairments in people with Charcot-Marie-Tooth disease.
Ankle-foot deformities
When varus deformity of the hindfoot during loading is primarily caused by a rigid deepened first ray or midfoot (pes cavus), in the presence of a flexible hindfoot, both conservative and surgical treatment options are possible. The best treatment option for an individual patient should be selected based on the principles of shared decision-making, taking personal goals and relevant activities into account. For example, surgical interventions are preferable when a patient aims to improve barefoot walking or wants to wear regular footwear, whereas conservative treatment options usually suffice as long as a patient is satisfied with orthopaedic footwear. The provision of (“low”) orthopaedic footwear should aim to bring the hindfoot into a neutral position, primarily by providing space to accommodate for the rigid deep ened first metatarsal (16). In addition, a stiffened heel fitting may be needed to maintain the hindfoot in the neutral position. Surgical interventions have a similar aim of restoring the alignment of the forefoot in order to allow the hindfoot to keep a neutral position when the foot is loaded (17). Surgical treatment primarily involves upheaving of the first ray by a dorsiflexion osteotomy of the first metatarsal. In the presence of a prominent midfoot cavus deformity, this can be combined with a midtarsal dorsiflexion osteotomy (18). A lateral displace ment osteotomy of the calcaneus can be added when dorsiflexion osteotomy is insufficient to fully correct the varus tilt of the hindoot during loading.
When varus deformity of the hindfoot cannot be corrected to a neutral position (pes cavovarus), surgical intervention should, in our opinion, be preferr ed over conservative treatment options. Surgical treatment involves a triple arthrodesis (i.e. fusion of the talocalcaneal, talonavicular, and calcaneocuboid joints) to correct the rigid varus deformity, combined with upheaving of the first ray by a dorsiflexion osteotomy of the first metatarsal to correct the rigid cavus deformity. Although some authors report that triple arthrodesis is associated with an increased risk of degenerative arthritis in other ankle and foot joints (19–22), our experience is that persistent malalignment after surgery (either persistent hindfoot varus deformity or inadequate correction of pes cavus) may primarily be responsible for this presumed association. Moreover, the risk of secondary degenerative arthritis may be even higher when the structural pes cavovarus remains uncorrected. This dilemma requires further study. When surgical correction is contraindicated or not preferred, (“high”) orthopaedic footwear is indicated with space to accommodate for the rigid deepened first ray, combined with a mediolateral ankle stabilizing orthotic element and lateral flare to provide stability to the hindfoot during loading. Inevitably, this treatment option comes with serious consequences for the weight, appearance, and ease of use of footwear.
In the presence of additional structural toe deform ities, the surgical procedures as described above can be combined with correction of the clawed hallux (modified Jones procedure) and/or lesser toes. When orthopaedic footwear is preferred, there should be enough space for the claw toe deformities and/or widened forefoot to prevent pain and pressure problems.
In the presence of a strong tibialis posterior muscle contributing to varus tilt of a flexible hindfoot, the above surgical procedures can be combined with a tibialis posterior tendon transfer to the lateral dorsum of the foot (23), with the aim of counteracting the inversion tendency. For this procedure to be effective, the tibialis posterior muscle should have sufficient strength (at least Medical Research Council (MRC) scale score 4 out of 5) during clinical examination.
In the presence of additional calf muscle shorten ing resulting in a rigid pes equinus and difficulties with maintaining a plantigrade foot position during loading, Achilles tendon lengthening (shortened soleus and gastrocnemius) or gastrocnemius slide (shortened gastrocnemius only) can be considered. However, we prefer to surgically correct the equinus deformity using a modified Lambrinudi triple arthrodesis (i.e. including a dorsiflexion wedge resection of the talus), because, with this procedure, the range of post-operative ankle dorsiflexion can be controlled more precisely and func tional strength of the calf-Achilles tendon complex is fully preserved. Thus, we aim for a plantigrade position of the foot, but with a limited ankle dorsiflexion range to prevent excessive tibia progression during the 2nd rocker when walking. Conservatively, a rigid pes equinus can be compensated by an increased heel lift integrated within the orthopaedic footwear.
In our centre (Gait Expertise Centre, Sint Maarten skliniek, Nijmegen, the Netherlands) we do not perform a release of the fascia plantaris in adults or adolescents with CMT. Severing the fascia plantaris is insufficient to correct the rigid deepened first ray or midfoot, and additional osteotomies are therefore needed. Maintaining the integrity of the fascia plantaris is preferable, as it helps to maintain the proper anatomy of the hallux and lesser toes through the reversed windlass mechanism (24). Moreover, we rarely perform a transfer of the peroneus longus tendon to the peroneus brevis tendon. Theoretically, this would enhance ankle-foot eversion and disarm the plantarflexing force of the peroneus longus muscle on the first metatarsal. Scientific proof for the efficacy of this treatment option is, however, lacking. Although we have published clinical improvements after this procedure, (25) we ceased to apply this treatment option, in order to reduce complications and operation time, without encountering any change in functional results.
Surgical procedures involving triple arthrodesis are preferably postponed until the age of skeletal maturity. However, in our centre (Gait Expertise Centre, Sint Maartenskliniek, Nijmegen, the Netherlands), we do perform forefoot osteotomies and soft-tissue surgery in adolescents who have not yet reached skeletal maturity, although more scientific evidence for these types of interventions is needed.
Muscle weakness
After optimal management of hindfoot varus deform ity or in the absence of varus tilt of the hindfoot during loading, clinical management should focus on the functional consequences of lower leg muscle weakness. Weakness of the ankle dorsiflexors may require mechan ical support with the aim of improv ing foot clearance during the swing phase of gait and promot ing heel strike and a normal first rocker. A flexible or articulated ankle-foot orthosis (AFO) with a dorsal shell is sufficient in the presence of dorsiflexor weakness without excessive knee flexion during stance (the latter either due to sufficient calf muscle strength, or due to limited ankle dorsiflexion range of motion). Indeed, it has been shown that AFOs reduce foot drop during swing and, thereby, reduce the need for a compensatory increase in hip flexion (26). As an alternative for an AFO, a tibialis posterior tendon transfer can be considered to reduce foot drop, irrespective of any concomitant varus tendency of the hindfoot (see above). Also for this indication, the tibialis posterior muscle should have sufficient strength (at least MRC score 4 out of 5) during clinical examination. Instrumented gait analysis in 23 people with CMT who had undergone a tibialis posterior transfer showed that this procedure was effective to reduce foot drop, but significantly reduced the active ankle plantarflexion moment during push-off (27). This is conceivable, as the tibialis posterior is an ankle plantarflexor besides an ankle-foot invertor. As most dorsiflexing AFOs that are effective for treating drop foot will also limit active ankle plantarflexion, they are likely to also reduce ankle plantarflexion power during push-off. Future studies should investigate which treatment option is preferable for which type of patient.
If foot drop coincides with excessive knee flexion during the stance phase of gait, a more rigid floor-reaction type of AFO with a ventral shell is recommended to reduce the degree of knee flexion and the need of compensatory knee extensor activity. In these cases, tibialis posterior tendon transfer is contraindicated, because the plantaflexors are already weakened.
When ankle-foot deformities are treated primarily with orthopaedic shoes, an AFO to reduce drop foot and/or excessive knee flexion should be fully integrat ed with this footwear, particularly in the presence of pronounced forefoot deformities and somatosensory impairments. In this case, a high shaft can be used in the orthopaedic shoes as an alternative form of AFO with limited plantarflexion and an individualized degree of stiffness toward dorsiflexion, depending on the degree and pattern of lower leg muscle weakness.
Somatosensory impairments
Unfortunately, reduced somatosensation cannot effectively be treated in any neurological condition. Yet, many of the surgical and conservative interventions described above are likely to have a beneficial effect on the residual exteroception, by enlarging the area of foot contact with the support surface and by reduc ing excessive pressure and pain. These interventions may also (indirectly) improve proprioception from the lower leg muscles and ankle joint by normalizing ankle-foot alignment and muscle length. If, nonetheless, disabling gait impairments persist despite optimal treatment and compensation for ankle-foot deformities and muscle weakness, a walking aid (e.g. a lightweight walking stick or wheeled walker) should be prescribed to compensate for somatosensory deficits. Indeed, besides delivering some degree of mechanical support, walking aids typically allow somatosensory information from the upper limbs to be used for postural control. Moreover, in our experience, AFOs with a ventral shell, in particular, may improve sensory feedback, as they stimulate the ventral skin over the shank during loading. As shown in Table I, scientific evidence for the efficacy of walking aids to improve gait stability is lacking in people with CMT, but clinical experience for this notion is abundant.
The step-wise treatment algorithm described here, combining both conservative and surgical treatment options for CMT-related gait impairments, is an attempt to set out a comprehensive clinical treatment guideline for this patient group. The treatment algorithm will be of value for today’s clinical practice, but more scientific evidence needs to be collected, for which Table I can serve as a template. Clinically relevant outcomes should include the attainment of personal goals, for instance pain reduction, better capacity to walk barefoot or wear regular footwear, and improve ment in personal activities and social participation. Ideally, surgical interventions should also be indicated and evaluated based on instrumented gait analysis, enabling the evaluation of kinematic and kinetic gait characteristics, including plantar pressure measure ments. Moreover, future studies should evaluate the added value of specific forms of functional gait training as an adjunct to surgical and/or conservative interventions for gait impairments in CMT.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize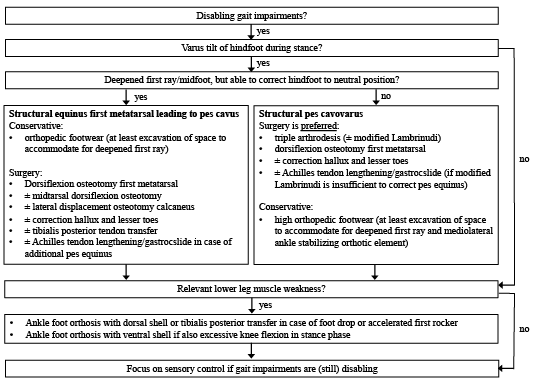 Click to show fullsize
Click to show fullsize