
From the 1Faculty of Health Sciences, OsloMet, 2Department of Physical Medicine and Rehabilitation, Oslo University Hospital, 3Research Centre for Habilitation and Rehabilitation Models and Services (CHARM), Institute of Health and Society, Faculty of Medicine, University of Oslo and 4Sunnaas Rehabilitation Hospital, Nesodden, Norway
Objective: Secondary analysis, testing the effect on change in health-related quality of life of group-based vestibular rehabilitation in patients with mild-moderate traumatic brain injury, dizziness and balance problems.
Design: A single-blind randomized controlled trial.
Subjects: A total of 65 patients aged 16–60 years with a Rivermead Post-concussion Symptoms Questionnaire dizziness score ≥ 2, and Dizziness Handicap Inventory score > 15 points. Data collection was performed at baseline 3.5 (standard deviation (SD) 2.1) months post-injury, end of intervention, and 4.4 (SD 1.0) months after baseline.
Methods: Quality of Life after Brain Injury was the main outcome. Independent variables were demographic and injury variables, Hospital Anxiety and Depression Scale, changes on the Rivermead Post-concussion Symptoms Questionnaire (RPQ3 physical and RPQ13 psychological/cognitive), and Vertigo Symptom Scale-Short Form.
Results: Mean age of participants was 39.4 years (SD 13.0); 70.3% women. Predictors of change in the Quality of Life after Brain Injury were receiving the vestibular rehabilitation (p = 0.049), baseline psychological distress (p = 0.020), and change in RPQ3 physical (p = 0.047) and RPQ13 psychological/cognitive (p = 0.047). Adjusted R2 was 0.399, F=6.13, p < 0.001.
Conclusion: There was an effect in favour of the intervention group in improvement in health-related quality of life. Changes on the Rivermead Post-concussion Symptoms Questionnaire were also associated with change on the Quality of Life after Brain Injury.
Key words: quality of life; traumatic brain injury; dizziness; randomized controlled trial; psychological distress; patient-reported outcome measure.
Accepted Mar 12, 2021; Epub ahead of print Mar 31, 2021
J Rehabil Med 2021; 53: jrm00181
Correspondence address: Helene L. Soberg. Faculty of Health Sciences, OsloMet – Oslo Metropolitan University, PO Box 4 St. Olavs plass, N-0130 Oslo, Norway. E-mail: helus@oslomet.no; uxheob@ous-hf.no
Doi: 10.2340/16501977-2823
This paper is the first to present results of a vestibular rehabilitation intervention study on changes in health- related quality of life in patients with dizziness and balance problems after mild-to-moderate traumatic brain injury. The intervention group received exercises and guidance aimed at self-efficacy and how to cope with their dizziness and balance problems. In addition, both the intervention and control groups received treatment as usual, comprising multidisciplinary rehabilitation at a university hospital. The main result was measured as change on the Quality of Life after Brain Injury questionnaire. Post-concussion symptoms, vertigo and psychological distress were also measured. The study showed that the group receiving the vestibular rehabilitation intervention underwent more improvement in health-related quality of life than the group receiving usual treatment alone. Other factors that influenced the improvement in quality of life were psychological distress at the start of the study and fewer post-concussion symptoms.
Sustaining a traumatic brain injury (TBI) affects patients’ functioning and health-related quality of life (HRQL) (1). TBI is defined as an alteration in brain function, or other evidence of brain pathology, caused by an external force (2). Research shows that HRQL is often reduced after a TBI, independent of the severity of the injury (3). Problems in cognitive, emotional, or physical functioning are associated with HRQL after TBI (4). Systematic reviews emphasize the multifactorial aetiology of post-concussion syndrome/symptoms (PCS), and that pre- and post-injury mental health are predictors of post-injury functioning after mild TBI (5, 6). Furthermore, both psychological and physical post-concussion symptoms, including dizziness, show significant correlation with the physical and mental aspects of HRQL (7).
Dizziness is a subjective experience that is often described as vertigo and balance problems, or light-headedness and disorientation (8). The aetiology of dizziness after a TBI can be caused by injuries in the vestibular system (9, 10), or have a non-vestibular origin (10). Zeldovich et al. found that 46% of patients with mild or moderate TBI and persistent PCS experienced dizziness post-injury and, at 6 months post-injury, dizziness was reported by approximately 30% of patients with complicated mild TBI (4). After 1 year, dizziness was reported in 25% of patients (11). Challenges caused by dizziness may hamper return to physical activities and work and increase the patients’ perception of post-concussion symptom pressure (12). There is, however, a lack of intervention studies on dizziness and balance problems after TBI (13). We have shown previously that self-reported dizziness-related disability, measured by the Dizziness Handicap Inventory (DHI), is associated with vertigo symptoms, balance problems, and psychological distress (14). These findings showed that a group-based adjusted programme for vestibular rehabilitation (VR) had an immediate, but not long-term, effect on dizziness-related disability (15). However, to our knowledge, there are no studies into how HRQL is affected in the subgroup of the TBI population having dizziness and balance problems.
The current study reports results for HRQL from a randomized controlled trial (RCT) that tested the efficacy of an individually modified, group-based VR intervention designed specifically for reducing dizziness and balance problems after TBI (15, 16). It is not known how HRQL change was in this subgroup of patients with TBI, and whether injury-related factors and changes in post-injury functioning had an effect on change in HRQL reported on a TBI-specific outcome measure. Hence, the main objectives of this secondary analysis of a RCT was to test the effect on changes in HRQL of a group-based VR programme in addition to routine multidisciplinary rehabilitation on patients with mild-to-moderate TBI and dizziness and balance problems. Secondarily, the current study aimed to describe the HRQL over time. It was hypothesized that mental health at baseline, improved persistent PCS and functioning, and reduced dizziness would have significant positive effects on changes in HRQL, and that the intervention group would show significantly more improvement in HRQL than the control group.
The study was a single-blind RCT. The study is registered with the Clinical Trials Registry (#NCT01695577) and approved by the Regional Committee for Medical Research Ethics, Norway (#2012/195b 20120306). In the current secondary analyses, the focus is on the patients’ HRQL. Written informed consent was obtained from all participants.
The patients with TBI were included between January 2013 and October 2015 and were followed up for 2 months post-intervention. Inclusion criteria were: patients with a TBI diagnosis (International Classification of Diseases 10th revision (ICD-10) diagnosis S06.0–S06.9); aged 16–60 years; reporting mild, moderate, or severe feelings of dizziness on the Rivermead Post-concussion Symptoms Questionnaire (RPQ) (17) (dizziness score ≥2) and/or had a positive Romberg’s test. All included patients had a score on the DHI >15 points, which was considered the cut-off for benefitting from a VR intervention. Exclusion criteria were severe psychological disease or substance abuse reported on the medical record, insufficient command of Norwegian and/or cognitive impairments (unable to follow instructions and/or complete forms), and comorbidities affecting mobility and independent gait. In addition, a cut-off point ≤15 points on the DHI was an exclusion criterion, because a total score of > 15 indicates a disability in the functioning of patients with peripheral or central pathology (18).
Procedure
A specialist in physical and rehabilitation medicine at the Department of Physical Medicine and Rehabilitation at Oslo University Hospital referred patients to the physical therapist (IK) who performed the group intervention. First, clinical assessments of the patients were performed, and those who fulfilled the inclusion criteria received oral and written information about the study.
The procedure has been described in more detail in a previous publication (15, 16). Briefly, all patients were assessed prior to allocation, and then were randomly assigned to the intervention group or the control group. Both groups received the usual multidisciplinary outpatient rehabilitation (TAU) delivered at our hospital (19). The focus of the outpatient rehabilitation was to strengthen the patients’ self-efficacy and facilitate their return to activities of daily living and work. Patients with a positive positioning test (Dix-Hallpike and Roll test) indicating Benign Paroxysmal Positional Vertigo (BPPV) were subject to repositioning manoeuvres after the baseline assessments (Epley and BBQ Roll manoeuvres) (14), independent of group allocation.
In addition, patients allocated to the intervention group received an individualized group-based VR programme, which was described more thoroughly in a previous publication, that consisted of 16 sessions over 8 weeks aimed at reducing dizziness-related disability (15, 16). Briefly, the intervention consisted of guidance and individually tailored VR exercises (adaptation, substitution, habituation/compensation components, and balance/gait exercises) offered twice a week by 2 physiotherapists (IK and KAB). The guidance emphasized self-efficacy and a salutogenic perspective. After the 8-week intervention period, all patients could participate in the outpatient rehabilitation programme at the hospital with 4 weekly psychoeducational group sessions that addressed strategies to reduce post-concussion symptoms and facilitate return to work (19).
Data collection at baseline (T0) was conducted 3.5 (SD 2.1) months after the TBI with the first follow-up (T1) at 2.7 (SD 0.8) months after baseline. The second follow-up (T2) was 4.4 (SD 1.0) months after baseline. A blinded tester administered the patient-reported outcome measures (PROMs), which were completed at T0 before group allocation, and then again at T1 and T2. The participants and the interventionist were not blinded for the group allocation. However, an uninvolved research assistant entered the data into the database, and the group allocation was not disclosed until after the initial analysis of the primary RCT was completed (15).
Methods
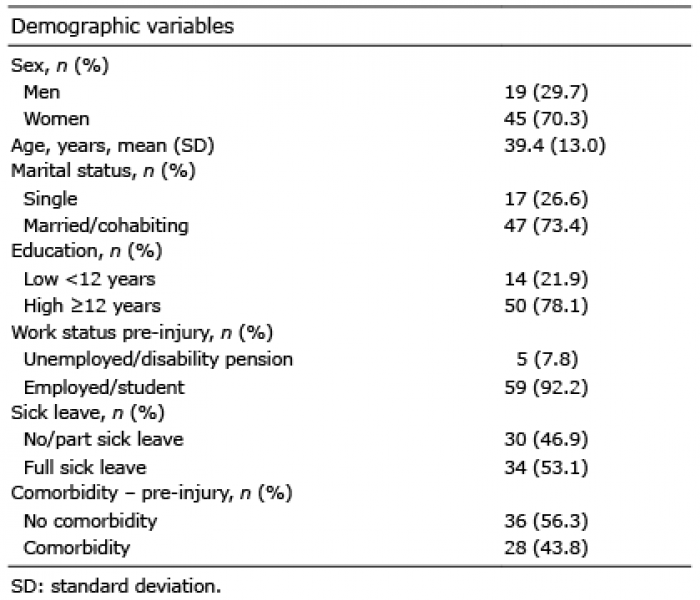
Information relating to personal factors, cause of injury, and severity of injury was obtained from the medical records. The personal factors comprised age at the time of injury, sex, married/cohabiting status (yes or no), level of education (low or high, with cut-off >12 years), pre-injury employment/studies (yes or no), and pre-injury comorbidities (yes or no). The injury severity parameters were the Glasgow Coma Scale score (GCS) (20), loss of consciousness (LOC) (yes or no/not reported), post-traumatic amnesia (PTA) (yes or no/not reported) and positive imaging findings on magnetic resonance imaging (MRI) or computed tomography (CT) (yes or no/not reported).
Outcome measures
The PROM Quality of Life after Brain Injury (QOLIBRI) was the main outcome measure in the current study (1, 21). The QOLIBRI is applicable to people with TBI of all severities and at all time-points after the injury. It consists of 2 parts with a total of 37 items, and assesses 6 dimensions of HRQL (21). The first part assesses the patients’ satisfaction in 4 domains (subscales) comprising Cognition, Self, Daily life and autonomy, and Social relationships. The second part relates to how bothered the responders rate themselves to be after the TBI in the 2 domains (subscales) of Emotions and Physical problems. Each item is scored on a 5-point scale, from 1 (not-at-all) to 5 (very), with reverse scoring on the bothered subscales. The QOLIBRI was scored according to an algorithm published by von Steinbüchel et al. (21). Missing item scores for each subscale were imputed by the scale mean if less than one-third of the responses were missing. The raw scores were transformed to a score ranging from 0 (lowest) to 100 (highest). Individual subscale scores and a total score were calculated. A score below 60 points has been suggested to represent poor HRQL (22).
The metric properties of the Norwegian QOLIBRI version have been tested and found satisfactory (23). In the current study, the internal consistency of the subscales and the total score at all time-points were measured with Cronbach’s α. They were between 0.94 and 0.80 for the Satisfaction subscales and the Bothered subscale for Emotion, and from 0.54 to 0.69 for the Physical subscale. For the QOLIBRI total scores, the Cronbach’s α values were between 0.88 and 0.93 for the 3 respective measurement time-points.
Patient functioning: independent variables
The Rivermead Post-concussion Symptoms Questionnaire (RPQ) assesses self-reported post-concussion symptoms (17). This 16-item standardized questionnaire captures the severity of post-concussion symptoms following TBI. The RPQ has 2 subscales, Physical (RPQ 3: headaches, dizziness, nausea) and Psychological/Cognitive (RPQ 13: noise sensitivity, sleep disturbance, fatigue, irritability, depression, frustration, forgetfulness, poor concentration, taking longer to think, blurred vision, light sensitivity, double vision, restlessness). The 5-point ordinal scale ranges from 0 (no problem) to 4 (severe problem). The RPQ summed score consists of the symptom scores excluding the ratings of 1, as 1 point signifies a level like that of pre-injury. The total score ranges from 0 to 64 (best–worst).
The Hospital Anxiety and Depression Scale (HADS) assesses psychological distress (24, 25). The HADS is a self-report questionnaire that comprises 14 items on 2 subscales (anxiety and depression). Each item is rated on a 4-point ordinal scale, from no distress (0) to too much distress (3). The total score is 42 points, with 21 points for each sub-scale. A cut-off was set at 8 points for possible anxiety and depression, respectively, and 11 points was the cut-off for probable anxiety or depression (24, 25).
The Vertigo Symptom Scale-Short Form (VSS-SF) measures symptoms of dizziness on 2 subscales, vertigo-balance symptoms (VSS-V) and autonomic-anxiety symptoms (VSS-A) (26) (27). It has 2 subscales, 1 relating to vertigo-balance symptoms (VSS-V) and 1 to autonomic-anxiety symptoms (VSS-A). It is scored on a 5-point ordinal scale (range 0–4), with an overall scale range from 0–60 points (best–worst), and 0–32 points on the VSS-A and 0–28 points on the VSS-V. The Norwegian version of the VSS-SF has satisfactory reliability in patients with vertigo (27).
The DHI is a 25-item self-report questionnaire assessing dizziness-related disability (28). A total score of 0–100 (best–worst) is reached by summing the ordinal scale responses (yes = 4, sometimes = 2, no = 0). The Norwegian version of the DHI has demonstrated satisfactory reliability and internal consistency (18).
Statistical analysis
For the demographic, injury-related, and functioning variables, between-group comparisons were performed using independent samples t-tests for the continuous data, and χ2 tests for the categorical data. An intention-to-treat analysis was performed when comparing the changes in HRQL on the QOLIBRI between the intervention group and the control group.
To evaluate the treatment effect on HRQL measured by the change in the QOLIBRI from baseline to T2 at 4.4 months after baseline, a linear regression model was used to assess the differences between the intervention and control groups. The independent variables were injury severity by the PTA (no/unsure or yes), baseline psychological distress measured by the HADS to account for baseline mental health, and changes in the condition-specific outcome measures RPQ3, RPQ13, VSS-V, and VSS-A from baseline to T2 at 4.4 months after baseline months post-injury. Change scores in the condition-specific outcome measures were used in the analyses to capture the impact of process-related factors of functioning on the change in HRQL. The included independent variables were associated with change in the QOLIBRI with a p-value < 0.2 in the univariate analyses. The assumptions for all the statistical tests were analysed and found to be satisfactory. The multicollinearity, residuals, and influential data point checks showed that the assumptions of the regression models were not violated (Cook’s distance (D < 0.1); centred leverage value (< 0.2)). Overall model performance was assessed by performing a bootstrapping validation with a 95% confidence interval (95% CI) using 1,000 bootstrap simulations. The results of the final regression model are presented with R2, adjusted R2 and F, and standardized β. The results are presented as mean differences with 95% CI and p-values. IBM SPSS Statistics 26 was used. All statistical tests were 2-sided and assumed a 5% significance level.
The study population comprised 45 (70.3%) women and 19 (30%) men. The mean age was 39.4 years (SD 13.0). The mean score on the DHI for dizziness-related disability at baseline was 44.6 (SD 17.9) points, which is categorized as moderate (29). Mean GCS score was 14.5 (SD 1.3) points. At T2, only 30% of the participants reported a score below the cut-off for inclusion in the study, which was 15 points. Information about the personal and injury-related factors is shown in Table I and Table II. There were no significant differences between the intervention and control groups at baseline regarding personal and injury-related factors, functioning, or participation in the multidisciplinary rehabilitation (15).
Table I. Demographic factors and injury-related characteristics of the 64 participants
Table II. Injury-related characteristics of the 64 participants
Post-injury functioning is presented for all participants in Table III. At baseline, RPQ was 31.6 (SD 10.5), VSS-SF was 18.6 (SD 9.9), and HADS was 15.6 (SD 7.8) points. The QOLIBRI scores were 53.2 (SD 17.5) points at baseline, 59.3 (SD 19.1) at T1, and 61.4 (SD 20.2) at T2. There was a significant improvement in the QOLIBRI total score from baseline to T1 of 5.2 points (95% CI 2.2–8.3), baseline to T2 of 7.7 points (95% CI 3.7–11–6), and T1 to T2 of 3.1 points (95% CI 0.02–6.1). At baseline, 65.6% of the patients had QOLIBRI scores below the suggested cut-off for poor HRQL at 60 points, and this improved to 49.2% at T1 (p < 0.001), and to 41.8% at T2 (p < 0.001) (not shown in the table).
Table III. Health-related quality of life and post-injury functioning
The results of the univariate regression analyses and the multivariate analysis are shown in Table IV. In the multivariate model adjusted for psychological distress by HADS at baseline and for changes in disease-specific functioning on the RPQ3 and RPQ13 from baseline to T2, the intervention group had a mean 6.5 points higher than the control group for the change scores on the QOLIBRI. The model explained 40% of the variance in the change in QOLIBRI from baseline to 6 months post-intervention. The bootstrapping analysis supported all the statistically significant results (group p = 0.049, HADS baseline p = 0.020, change in RPQ3 p = 0.002, and RPQ13 p = 0.047).
Table IV. Results of univariate and multivariate analyses between changes (mean improvements) in outcome measures assessing condition-specific functioning and improved health-related quality of life (HRQL) on the Quality of Life after Brain Injury (QOLIBRI) from baseline (T0) to second follow-up (T2)
To our knowledge, this is the first RCT to examine HRQL in patients with TBI with dizziness and balance problems in need of VR by applying a condition-specific self-report questionnaire (30). This study showed that the VR intervention produced significant improvements in HRQL from baseline to the end of follow-up, which was 4.4 months later, on average. There was a group effect on the change in HRQL in favour of the intervention group. The study also showed that, for all participants, independent of group allocation, reduced post-concussion symptoms measured by the RPQ3 and RPQ13 contributed to the improved HRQL. Interestingly, changes in self-reported vertigo on the VSS subscales were not associated with change on the QOLIBRI, even though dizziness was still a problem for 70% of the participants with a DHI score >15 points, which was the cut-off for inclusion in the study (14). Some of the change in symptom pressure might have been captured in the RPQ3 (nausea, headache, dizziness); however, the changes over time in the RPQ3, VSS-V, and VSS-A were only moderately correlated, and did not violate the inter-correlation criterion of Spearman’s ρ ≤ 0.7. Furthermore, the current study shows that the patients with more symptoms of psychological distress on the HADS at baseline showed significantly higher improvement in HRQL, independent of group allocation.
Few RCTs have tested interventions on HRQL in patients with TBI (30). In the current study, all participants received the routine outpatient rehabilitation offered at the specialized rehabilitation clinic to patients with a protracted course of recovery after mild to moderate TBI (19). As this programme comprises individual assessments and addresses activity pacing, self-efficacy, and a timely return to work, it may well capture and reduce the emotional distress and post-concussion symptoms associated with HRQL reported in non-randomized studies.
There is conflicting evidence on the effect of different aspects of cognitive interventions after TBI. A Cochrane review on cognitive rehabilitation interventions showed no effect of cognitive rehabilitation compared with conventional rehabilitation, and 1 RCT with moderate evidence quality concluded there was no effect on HRQL (31). However, in a RCT that tested a cognitive behavioural therapy (CBT) intervention in patients with mild and moderate TBI and PCS, improvements on the HRQL were found in the CBT group (32).
Contrary to our hypothesis, the change in self-reported dizziness on the VSS subscales capturing vertigo and anxiety symptoms were not associated with the change in HRQL, even though there was significant reduction in vestibular symptoms over time. In another study on dizziness, patients with BPPV without TBI reported improved function on the SF-36 mental health and social function subscales one month after the repositioning manoeuvre (33). The patients had initial symptom pressure similar to the participants in the current study, but a somewhat larger reduction in dizziness-related disability, even though all participants with BPPV in the current study also received manoeuvre treatment (14). However, studies have shown that patients with TBI often have more than one cause of dizziness, and the exact causes of dizziness and balance problems may be unclear, as a combination of disorders is often present (9, 34). The complexity of central and peripheral factors may make recovery from dizziness after TBI/trauma to the head more complex, which may explain why the dizziness on the VSS subscales was not a significant predictor of HRQL. Another perspective might be that the VR intervention, in addition to focusing on motor control and balance, also included general strength and conditioning exercises, which have been found to improve HRQL in patients with TBI (30). In addition, the reduced psychological distress and improved self-efficacy that are associated with HRQL might have influenced how dizziness is managed in daily life.
Pre-injury mental health status is a predictor of persistent PCS in general (6). Furthermore, psychological distress in patients with dizziness of heterogeneous aetiology explained more than 60% of the variance in mental health on the generic HRQL measure, the Mental Component Summary in SF-36 (35). Hence, mental health issues can pre-exist, but also emerge as a consequence of an injury (6, 36), and have an independent impact on HRQL independent of rehabilitation programmes (7). Karr et al. reported that the patients did not differ in their self-reported change in PCS severity, i.e. pre-injury mental health problems were not associated with short-term change in PCS (6). In the current study, we adjusted for psychological distress at baseline post-injury in the multivariate regression analysis. We could not determine whether the psychological distress at baseline was caused by pre- or post-injury factors; however, the findings of other studies may also pertain to HRQL in addition to PCS (5, 6). In the current study, sex was not a significant predictor for change in HRQL; however, we have in a previous publication pointed to the fact that women tend to report more PCS and psychological distress than do men (14).
Changes in PCS, as measured by the RPQ, also predicted change in HRQL independent of group allocation. It is well known that PCS attenuates over time in the natural course of recovery, even in patients with a protracted course of recovery. Moreover, a reduction in PCS is the goal of most rehabilitation programmes, as it was in the current study for this subgroup of patients with TBI having dizziness as one of their symptoms.
Strengths and limitations
The strength of this study is that, by including the patient-reported secondary outcome (HRQL) changes across the follow-up time, a more complete picture emerged of the multifaceted nature of TBI recovery. The importance of assessing HRQL in TBI subgroups called for further exploration of accessible data from this larger project. The current study provided significant results on the effect of the intervention and the effects of baseline mental health and change in functioning. The regression model and hence, the findings, were robust, and the bootstrapping procedure validated the results. However, some limitations should be discussed. The power calculations were based on the main outcome measures (15), and not on the QOLIBRI; thus, we cannot disregard the possibility of type II errors. For example, the impact of PTA, which is a parameter of injury severity, approached significance with a p-value of 0.068. Another limitation is the skewness in the total number of therapy sessions. The control group received TAU, which was delivered by a multidisciplinary team (19), whereas the intervention group received TAU and VR intervention.
There was a significant group effect in favour of the intervention group in improvement HRQL on the QOLIBRI. The changes in PCS on the RPQ were also associated with change on the QOLIBRI, whereas self-reported dizziness on the VSS-SF was not.


 Click to show fullsize
Click to show fullsize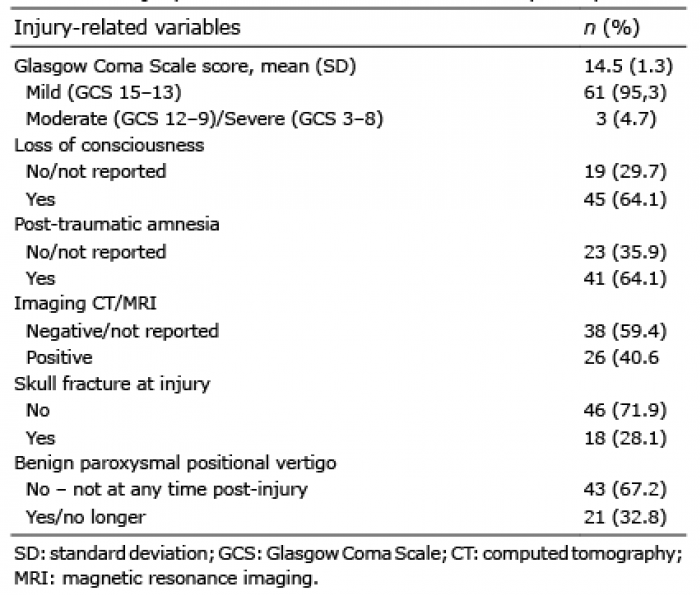 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize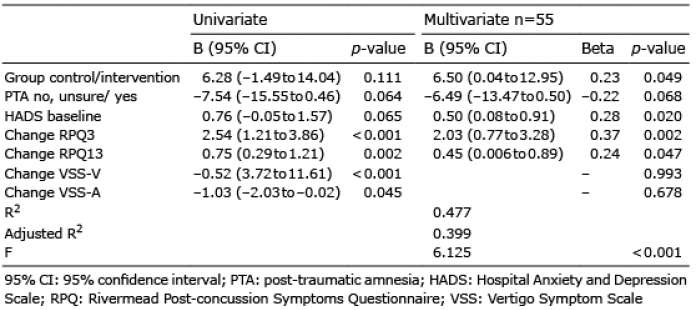 Click to show fullsize
Click to show fullsize