
From the 1Department of Behavioural Sciences and Learning, 2HELIX Competence Centre, 3Department of Health, Medicine and Caring Sciences and 4Pain and Rehabilitation Centre, and Department of Health, Medicine and Caring Sciences, Linköping University, Linköping, Sweden
Objective: The activity ability assessment is a Swedish method for assessing general work ability, based on self-reports combined with an examination by specially trained physicians, and, if needed, extended assessments by occupational therapists, physiotherapists and/or psychologists. The aim of this study was to analyse the predictive validity of the activity ability assessment in relation to future sick leave.
Design: Analysis of assessments in 300 case files, in relation to register data on sick leave.
Subjects: People on sick leave (n =300, 32% men, 68% women; mean age 48 years; assessment at mean sick leave day 249).
Methods: Univariate and multivariate statistics.
Results: Self-rated work ability was the only factor with predictive value related to future sick leave. Physicians’ evaluations lacked predictive value, except where the person had a limitation in vision, hearing or speech that was predictive of future decisions by the Social Insurance Agency. No sex differences were identified.
Conclusion: The predictive value of the activity ability assessment for future sick leave is limited, and self-rated work ability is more accurate compared with an extensive insurance medical assessment. Self-rated work ability may be more holistic compared with insurance medicine assessments, which may be overly focused on individual factors. A practical implication of this is that the inclusion of contextual factors in assessment procedures needs to be improved.
Key words: social security; sick leave; return to work.
Accepted Jan 28, 2021; Epub ahead of print Feb 17, 2021
J Rehabil Med 2021; 53: jrm00177
Correspondence address: Christian Ståhl, Department of Behavioural Sciences and Learning, Linköping University, Linköping, Sweden. E-mail: christian.stahl@liu.se
Doi: 10.2340/16501977-2798
This study investigates whether assessments of general work ability (i.e. a person’s ability to work in any job) can predict future sick leave. The assessment method was developed in the Swedish sickness insurance system, and consists of a self-assessment, and assessments by physicians and other healthcare professionals. The results show that assessments generally fail to predict sick leave, with the exception of the person’s own assessment, which is broader and takes more aspects into account. These results can be used to improve assessment methods, where it is especially important to pay attention to a person’s whole situation.
This study investigates whether assessments of general work ability (i.e. a person’s ability to work in any job) can predict future sick leave. The assessment method was developed in the Swedish sickness insurance system, and consists of a self-assessment, and assessments by physicians and other healthcare professionals. The results show that assessments generally fail to predict sick leave, with the exception of the person’s own assessment, which is broader and takes more aspects into account. These results can be used to improve assessment methods, where it is especially important to pay attention to a person’s whole situation.
Assessing peoples’ functioning and work ability is a concern for most sickness insurance or workers’ compensation systems, in order to determine eligibility for benefits (1) and for rehabilitation needs (2). Methods for such assessments exist in various forms, ranging from relatively simple sick notes from physicians, to extensive evaluations by multiple professionals. It is also common that a system utilizes a variety of methods, depending on the situation, the complexity of the case, or the time-point.
Work ability is a complex concept, and there is not always consensus among actors in the rehabilitation process about how it should be conceptualized or measured (3). It is also not always clear to what extent work ability assessments give accurate descriptions of a person’s ability to work, since assessment methods may have flaws regarding both their validity and their reliability (1). Furthermore, it is not always clear whether assessments give an accurate prediction of a person’s future abilities, or whether they can provide information about the expected length of the person’s sick leave. These aspects are related to the internal validity of the method, e.g. their consistency and accuracy, but also their external validity, e.g. whether the results are representative in relation to the context of the assessment. Contextual aspects will also be influential for whether the assessments have predictive value, e.g. depending on regulations or internal procedures for granting benefits. For return to work, complex multi-disciplinary interventions and cooperation between several actors are often required (4), the outcomes of which medical assessments are unlikely to predict well. Furthermore, the predictors for return to work are not always the same as those for whether sickness benefits are granted, as insurance regulations and policies are not necessarily adapted to evidence from research on rehabilitation (5).
In the Swedish sickness insurance system, work ability is initially assessed in relation to the workplace where the person is employed (specific work ability, in Tengland’s (6) terminology), based on a medical certificate from a physician, and information from the person and the employer about the characteristics of the job. Sickness benefits can be granted at 25, 50, 75 or 100% of the person’s work hours, which is compensated to a level of 80%. Unemployed people are assessed in relation to any job normally available on the labour market (general work ability) and, after 180 days, this type of assessment is also made for employed people. After 365 days, compensation is reduced to 75% if the illness is not considered severe.
For assessment of general work ability, it is common to use more extensive assessment procedures. Since 2018, the Swedish Social Insurance Agency (SSIA) has applied an insurance medical method for assessments of general work ability, called activity ability assessment (AFU). Although the AFU is a model used in a specific national context, it is of international interest, since it is an example of an assessment method that focuses on general work ability, and which is designed to fit all types of diagnoses.
The AFU aims to offer a holistic assessment of a person’s functional and activity limitations, with a specific focus on remaining abilities, containing a self-assessment by the person on sick leave, an examination by a physician (including physical and mental status; physical strength and endurance; balance and coordination; and a neuropsychiatric interview if there is a psychiatric diagnosis, a suspicion of such a diagnosis, or a psychological condition), and, if needed, an extended assessment by occupational therapists, physiotherapists and/or psychologists. Based on the assessment, the SSIA official makes a statement about the person’s general work ability, which is used for determining eligibility for continued benefits. The method has been described in more detail in a previous publication (7).
Aim
The aim of this study was to analyse the predictive validity of the AFU in relation to future sickness benefits.
The material analysed in this article is part of a larger project, also involving qualitative case material, which has been reported in a separate article (7), in which the experiences of the methods, collected from officials, physicians and persons on sick leave, were analysed.
Statistical analysis of whether the AFU can predict future sick leave was performed. For this purpose, the first 300 case files in which AFU was applied were collected from the SSIA, entered into a database, and analysed in relation to register data from the SSIA on sickness benefits for the same individuals. In these cases, AFU was conducted during the period July 2013 to February 2014.
The case files included all documentation from the AFU assessment, including journal entries by the SSIA official for the current case. Journal entries were examined to determine the occupation of the individual, whether the assessment led to granted or withdrawn sickness benefits, and continued planning. Professional descriptions were encoded in accordance with Standard for Swedish Occupational Classification (SSYK). The case files were summarized in an Excel file, which initially included all information from the assessments and journals for 20 cases to gain an overview of the content of the documentation and to determine what was relevant to include in the analysis. The file was then examined and the entries shortened, excluding information that was not considered relevant for the analysis. Of the outcome measures, 1 (SSIA decision following assessment) has been retrieved from the case files, and 2 (sick leave 6 months after AFU and number of sick leave days after AFU) from register data.
Independent variables
Age was grouped into 4 categories: 20–34, 35–44, 45–54, and 55–65 years. Occupational status indicated whether the person was employed, unemployed, self-employed, or other. For those in employment, the educational demands for the job were classified into 4 categories, based on the SSYK: (i) profession requiring long theoretical education; (ii) profession requiring short theoretical education; (iii) profession not requiring theoretical education; and (iv) unemployed.
Diagnosis groups were based on the information in the medical certificate in the case file, indicating on which diagnosis the sick leave is based. Diagnoses are based on the International Classification of Diseases (ICD)-10 and are coded based on the diagnosis groups given there (e.g. F for mental disorders, M for musculoskeletal disorders).
The activity ability profile is based on 4 sections from the AFU, in which the physician uses a scale for each question (0 = no/insignificant activity limitation; 1 = light; 2 =moderate; 3 = large; 4 = very large/total activity limitation). Indices were created for the sections for physical and mental function. The physical function index was calculated as the mean of the 2 questions included in this category in the AFU (activity limitation for strength and physical endurance). The index for mental function was calculated as the mean of the 4 questions included in this category of AFU (activity limitation regarding memory, affective and executive ability; and mental endurance). The sections vision, hearing, speech, and balance, coordination, fine motor skills had only one question each, so no indices were required. Extended assessments were coded dichotomously, as yes/no. The person’s self-assessment of their work ability today and in 6 months were reported on a scale from 0 to 10 and coded as such. The person’s expectation about return to work was coded dichotomously, as yes/no; the unemployed were coded separately for this variable as they did not have an employer to return to.
Missing data on all scales were replaced according to the convention in the Short Form 36 (SF-36) Health Survey (8), where a total score was calculated for a person if they had answered at least half of the questions on the scale. Missing items in these cases were given the mean score of the other items in the scale, i.e. the individual mean. This was done since the intercorrelations of the items of each scale lead to more realistic estimations of the missing values within that scale. This replacement of missing items in a scale was done to take care of dropouts and the uncertainty they entrain. Cronbach’s alpha was calculated for each index, and was 0.88 for physical function and 0.88 for mental function.
Dependent variables
For the variable “Number of sick leave days after completion of AFU”, negative values (n = 5, indicating that the sick leave period ended prior to the assessment) were coded as 0, and the number of days after AFU was grouped in number of months prior to regression analysis. The variable “Sick leave after 6 months after AFU” is dichotomous (yes/no) and describes whether the person receives sickness benefit 6 months after completion of AFU. This time-point was considered long enough to determine whether the person was still on sick leave after the assessment. The variable “SSIA’s decision after AFU” includes 0, 25, 50, 75, and 100% reduced work ability in relation to jobs normally available on the labour market.
Statistical analysis
Data were analysed using the computer programs SPSS 24.0 (Armonk, NY: IBM Corp. 2016) and Stata 14.0 (College Station, TX: StataCorp LP. 2015). Descriptive statistics are presented as frequencies for categorical variables or mean values and standard deviations for continuous variables. Differences between the groups were examined with χ2 test or Fisher’s exact test for categorical variables, and with Student’s t-test for continuous variables.
The binary outcome “Sick leave 6 months after AFU” was analysed by logistic regression and the results presented as odds ratios (ORs) and 95% confidence intervals (95% CIs). The outcomes “Number of sick leave days” (grouped in number of months) and “SSIA’s decision after AFU” were analysed by ordered logistic regression and the results presented as ORs and 95% CIs. In these analyses, the variable “SSIA’s decision after AFU” was coded dichotomously, where 0 indicated not being assessed as having reduced work ability, and other options as being assessed as having reduced work ability. The analyses were performed to calculate odds ratios for age, sex, employment, diagnosis, physical and mental functions, balance/coordination, vision/ hearing, extended assessment, self-assessed work ability (present and 6 months) and the expectation of return to work. Continuous variables were used as predictors in the regression analyses, and were standardized with the mean 0 and standard deviation 1 in the study population to allow comparisons. The analyses were adjusted for age and sex.
A Varimax-rotated factor analysis was performed for the various capacity scales (self-assessed of work ability, self-assessed work ability in 6 months, physical function, mental function, balance/coordination and hearing/sight) to develop and test simplified components, thereby reducing the risk of reporting statistical significance due to multiple testing. The extraction method was principal component analysis with rotation method varimax with Kaiser normalization using the option of replacement of missing values with the mean in SPSS (9). Finally, a multivariate regression analysis was made to examine the independent effect of the 3 factors found in the factor analysis as determinants for each of the outcome measures.
A matrix of pairwise correlation coefficients between different capacity scales was performed to check for multicollinearity in performing multivariate logistic regression analysis. The Pearson correlation coefficient between physical function and balance/coordination was 0.457, which is moderately strong. There was no evidence of multicollinearity between different variables used in the multivariate logistic regression analysis.
The results comprise descriptive data on the study group, after which descriptive findings from the AFU assessments are reported, followed by univariate and multivariate analyses of the predictive value of the AFU assessments in relation to the outcomes. Results were considered statistically significant at p ≤ 0.05 with 2-sided tests.
Ethical considerations
The study was approved by the Regional Ethics Review Board in Linköping, Sweden (dnr. 2014/16-31).
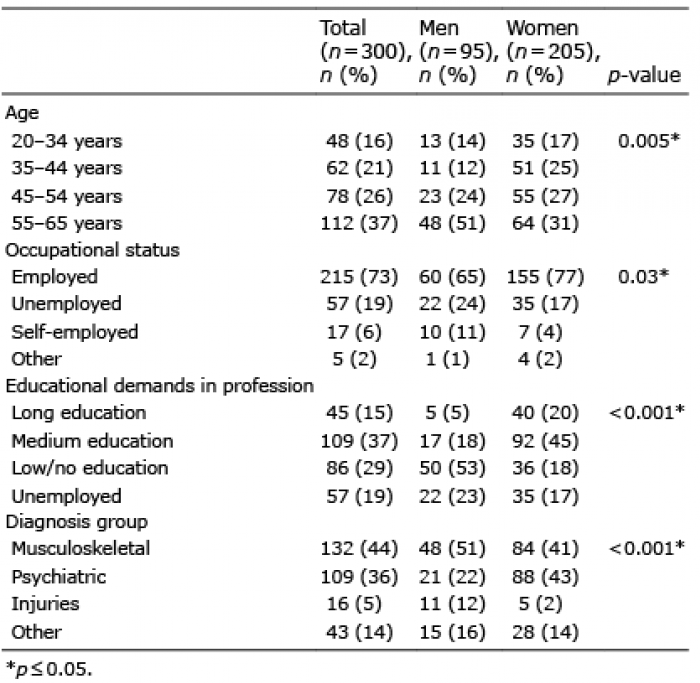
Of the 300 persons examined in the case files, 68% were women and 32% men (Table I). The mean age was 48 years, range 21–65 years. The men were significantly older (mean age 51 years), compared with women (mean age 47 years), p = 0.005. The majority was employed (73%), while 19% were unemployed, 6% self-employed, and 2% were students or on parental leave. Women had occupations with significantly higher educational demands than men.
Women had psychiatric diagnoses to a higher extent than men, while musculoskeletal diagnoses were most common for men. Injuries were more commonly reported among men than among women. These numbers are in line with the general distribution of diagnoses among people on sick leave in Sweden (10).
The AFU had been conducted on a mean of 249 days into the sick leave case (median 211 days), with a large range, between 59 and 1,052 days. A majority of the persons (89%) had at least one previous case of sick leave.
Table I. Demographic information for study participants. p-values indicate differences between sexes
Findings at the time of AFU
The estimated activity limitation in the 4 categories included in the AFU is shown in Table II. Men had significantly higher activity limitations than women in physical function (p < 0.001), and in balance, coordination and fine motor skills (p = 0.008).
People considered themselves able to return to work in 26% of cases. Self-assessed work ability was 2.81, on mean, (on a scale of 0–10), and the self-assessed work ability in 6 months was 5.14. No significant differences were noted between the sexes for these variables.
Extended assessments were used in 34% of cases. In cases where an extended assessment had been conducted, usually only one other profession had been involved (in 66% of cases), usually a psychologist (27%) or occupational therapist (24%). In some cases, several professions had been involved, most commonly, a combination of a psychologist and an occupational therapist.
Table II. Assessment in the activity ability assessment (AFU), where measures of physical/mental function, balance/coordination and vision/hearing/speech are assessed on a scale from 0 (no/insignificant limitation) to 4 (significant/total limitation). Work ability is rated on a scale from 0 to 10. p-values indicate sex differences
Decisions after the AFU
The SSIA’s assessment of the person’s general work ability after the AFU varies, but 51% were considered to have a fully reduced work ability, i.e. implying that sickness benefits of 100% will be granted. Most persons (79%) were assessed as having either a completely reduced work ability, or no reduction in work ability (indicating that benefits will be completely withdrawn); the alternatives between them (25, 50 or 75% reduced work ability) together represent 21% of the sample. There were no significant differences between the sexes for these assessments.
Of those having undergone an AFU, 58% were sick listed in the same case, with a mean of 316 days after the AFU, with no significant differences between the sexes. People with psychiatric diagnoses were, however, on sick leave significantly longer (384 days) than those with musculoskeletal diagnoses (280 days, p = 0.001). Of those assessed as not having a reduced work ability after the AFU and who had their benefits withdrawn, 39% were later on a new period of sick leave, indicating that a substantial number of those assessed as able to work, in fact, have a limited work ability.
Predictive properties of the AFU
This section presents regression analyses of the predictive properties of the AFU in relation to the 3 independent variables.
Concerning the outcome “Sick leave 6 months after AFU”, self-employed persons appear to be less likely to remain on sick leave than employees, and persons in professions with lower educational demands are less likely to remain on sick leave (Table III). Persons with psychiatric diagnoses also appear to have a higher risk of remaining on sick leave than those with other diagnoses, as shown by the fact that those assessed as having more mental limitations in the AFU have an increased risk of remaining on sick leave. The results also show that people who estimate their work ability as high at the AFU are less likely to remain on sick leave 6 months after the assessment. It is noteworthy that the person’s own estimation of their work ability at the time of the AFU is more accurate in relation to actual outcomes compared with the self-assessed future work ability, indicating an exaggerated expectation of recovery.
Table III. Logistic regression analysis for the dependent variable Sick leave 6 months after activity ability assessment (AFU), adjusted for age and sex
The outcome “Number of sick leave days after AFU” shows a similar pattern as the above results, where people in professions with lower educational demands had a significantly lower risk for longer periods of sick leave compared with those in professions with higher educational demands (OR 0.43 for medium education, p=0.008, OR 0.41 for short/no education, p=0.01), and people with psychiatric diagnoses have a significantly higher risk compared with those with musculoskeletal diagnoses (OR 2.08, p = 0.002). A higher self-rated work ability indicates a shorter future sick leave (OR 0.68, p <0.001).
The outcome “SSIA decision after AFU” shows that unemployed people are at higher risk of being assessed as having a reduced work ability compared with those who are employed, while no significant differences were found regarding educational demands in the profession (Table IV). Those with psychiatric diagnoses have a higher risk of being assessed as having reduced work ability compared with those with musculoskeletal diagnoses. Those with limitations in physical or mental function, or in balance, coordination or fine motor skills, have a higher risk of being assessed as having reduced work ability. Those with high self-rated work ability have a lower risk of being assessed as having reduced work ability.
Table IV. Ordered logistic regression analysis of the dependent variable “SSIA’s decision after AFU” (being assessed as having reduced work ability), adjusted for age and sex
Factor analyses of predictive properties of the AFU
A factor analysis identified 3 distinct factors in the AFU, which together explain 73% of the variance: (i) self-rated work ability, (ii) limitations in physical and mental function, and balance, coordination and fine motor skills, and (iii) limitation in vision, hearing or speech limitation (Table V).
Self-rated work ability is the only factor that significantly predicts all of the 3 outcomes (Table VI). The factor vision, hearing or speech limitation also predicts future decisions by the SSIA. Apart from this, there are no aspects related to the physician’s evaluation that have predictive properties for the outcomes.
Table V. Factor analysis. Factor loadings < 0.5 are not reported
Table VI. Multivariate analysis of continued sick leave after activity ability assessment (AFU), adjusted for other variables in the table, age and sex
The main finding of this study is that only self-rated work ability had any predictive value related to future sick leave, which is in line with earlier research indicating that self-reported work ability is a predictor of long-term sick leave (11, 12). The physician’s evaluation in the AFU did not have such a predictive value, expect for cases where the person had a limitation in vision, hearing or speech, which was predictive of future decisions by the SSIA. The results show no differences between men and women in self-rated work ability or level of sick leave after the assessment, but men were assessed as having slightly higher limitations of physical function and balance, coordination and fine motor skills. A notable result is also that a large portion of those assessed as able to work and who had their benefits withdrawn (39%) will have a new period of sick leave after the decision, which adds to the result that the person’s own assessment has the strongest predictive value of future sick leave.
That self-rated work ability has high predictive value can be interpreted differently. One interpretation is that, since work ability is a complex construct dependent on complex interactions between individual, organizational and societal factors (3, 6, 13), it is difficult to provide an objective assessment that captures all its dimensions, and that is consistent over time. Work ability is contextual and situational, and prone to change when conditions change, and it is therefore likely that the person in question will have a more holistic approach to their own situation and is likely to provide a more reasonable account of their future work ability. Another interpretation of the strong predictive validity of self-rated work ability is that these assessments have a “Pygmalion effect”, i.e. that they become self-fulfilling prophecies. There is no inherent contradiction between these interpretations: a holistic self-assessment can be assumed to also have an influence both on how people consider their future abilities, and how these actually develop.
For assessments to be valid, they need to include a broad range of factors, and an assessment is bound to become irrelevant if the conditions change. General work ability (6) is more difficult to assess, given that there is no specific job task to which to relate the assessment, which implies that assessment of the individual abilities need to include not only medical factors, but also the person’s skills, educational background and work experience. Although the AFU was designed to assess general work ability (i.e. not relating it to a specific job), the method does not have to be limited to medical factors, but could take the person’s occupational status, education and experience into account to make an assessment that is more relevant. Employment opportunities, and thereby a person’s actual work ability, are affected by both individual factors and contextual factors, such as the labour market conditions. When the AFU was developed, it was accompanied by a description of work demands in 40 common occupations, which was to be used as a reference when performing the assessments; this material, however, had no legal status, and the insurance officials did not use it to any great extent, as reported in a previous study (7).
These results show that people who rate their work ability as high have a lower risk of future sick leave, which is unsurprising. In agreement with previous research (10), the results also show that people with psychiatric diagnoses have a higher risk of long periods of sick leave. The AFU seems to have a larger impact on sick leave case when the SSIA decides to withdraw benefits, where it contributes to legitimizing the decision (7). The results from the qualitative study also indicate that the social validity of the AFU, i.e. whether the method can be considered acceptable in relation to goals, procedures and outcomes, seems quite low in cases where it is used to legitimize withdrawn benefits.
Another finding was that people who have lower education or are self-employed have a lower risk of remaining on sick leave. This may appear to be a surprising finding, if we were to assume that they have returned to work. A previous Swedish study has shown that people with lower education and jobs with poor work conditions return to work faster than others (14), which was suggested to be related to stronger needs to secure their job. Other studies have shown that people with lower education or in blue-collar jobs tend to have a higher risk of sick leave and fewer opportunities to return to work (15, 16), and that there is a social inequality aspect to the prospects for rehabilitation. However, the current study only measured whether people are receiving benefits, and not if they returned to work, which are two outcomes that are sometimes falsely considered as synonymous. It is possible that these people have returned to work (possibly to jobs with poor work conditions), or they could be supported by other means, such as partners or relatives. Our data only shows that this group has a higher risk of having their sickness benefits withdrawn.
As the AFU assessment is designed to determine eligibility for benefits, it is strictly limited to the individual abilities, aspects related to the person’s job or employment situation are not considered in the assessment procedure. Given the findings that self-rated work ability is predictive of future sick leave, while the assessment is not, it can be argued that the person will take such aspects into account when rating their work ability, where the results indicate that this provides a more accurate assessment. It also indicates that the social inequalities in return to work are not accurately adjusted for in eligibility assessments, which may imply a risk of exacerbated inequalities in cases where assessments are overly strict.
The results are also interesting in relation to what factors influence decisions about sickness benefits. The finding that a substantive number of those who are denied benefits after the AFU return with a new period of sick leave indicates that the assessments are made based on a too-narrow definition of work ability, where aspects that are not included could prove to influence the person’s actual ability to work (3). Another aspect of decision-making is the regulatory and managerial influence on insurance officials’ work, where it has been shown how directives toward lowering sick leave numbers have had a strong influence on officials’ assessment procedures, promoting a stricter interpretation of regulations (17). Such aspects are of importance for whether an assessment, such as the AFU, will be used for legitimizing withdrawn benefits.
Methodological considerations
The data collection comprises AFU assessments from the period 2013 to 2014 (i.e. during a testing period), which means that the results are not necessarily reflective of how assessments are carried out today. However, the method, as such, is fundamentally intact, although the experience of using it in practice was limited at the time of study. The results were presented to the SSIA at around the time when the method was made permanent, and it is possible that the results had an influence on later applications of the model. These results are, therefore, relevant as a benchmark for future studies of the method, where replication studies could be carried out to study how it develops in practical use.
The register data only contains information about sick leave, which makes any conclusions about return to work speculative at best. It is possible that people who are assessed as having work ability do or do not return to work. The current analyses, therefore, relate only to whether people are being assessed as having their work ability reduced, and whether they continue receiving sickness benefits. In the analyses we have not differentiated between whether people are granted sick pay or disability pension, as both of these benefits require reduced work ability; it is hence the reduced ability, as such, that is in focus of the study.
The use of SSYK classifications to determine educational demands in different jobs was used in lieu of register data on the educational level of the people in the study. This may have impacted the analyses, e.g. the finding that people in jobs with lower educational demands have a lower risk of remaining on sick leave, which could be attributed to differences between the SSYK classification and actual labour market conditions of different social groups.
Conclusion
In conclusion, the predictive value of the AFU for future sick leave is limited: the self-rated work ability of the person on sick leave was the only factor that had predictive value related to the outcomes. As such, the results point to the self-rated work ability as more accurate compared with an extensive insurance medical assessment. An interpretation of these results is that a person’s self-rated work ability is more holistic, while insurance medicine assessments of general work ability are too focused on individual factors. A practical implication of this is that the way assessment procedures include contextual factors needs to be improved.
This study was funded by a research grant from the SSIA. The funding agency had no role in study design, data analysis, data interpretation, writing of the report, or the decision to submit for publication. The authors had full access to all the data in the study and had final responsibility for the decision to submit for publication.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize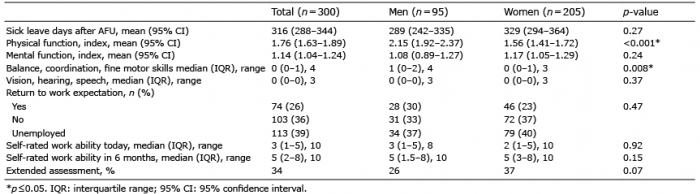 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize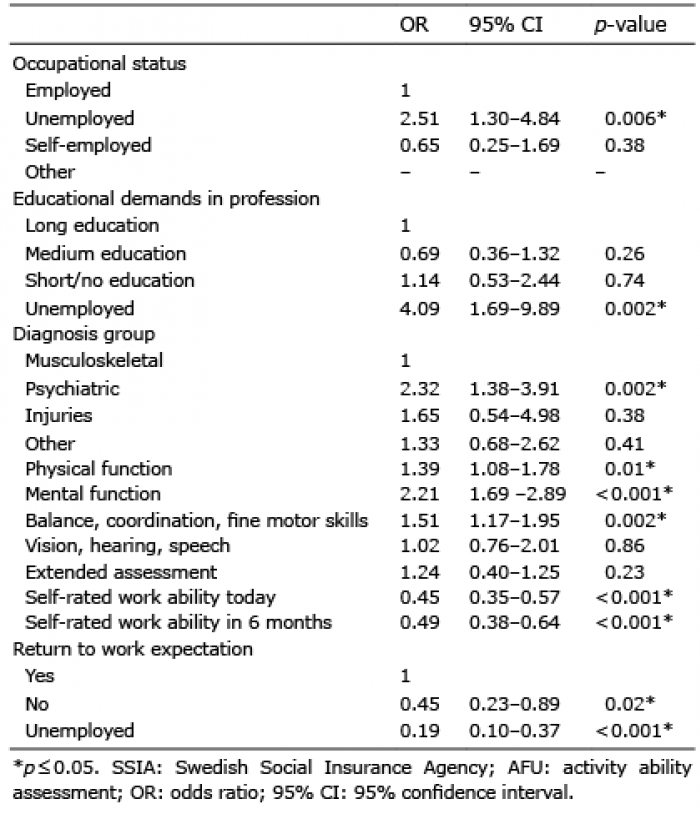 Click to show fullsize
Click to show fullsize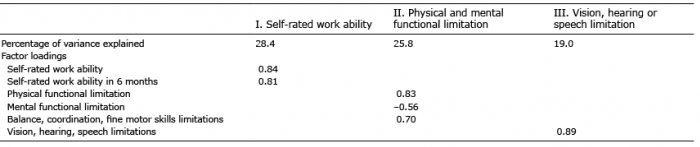 Click to show fullsize
Click to show fullsize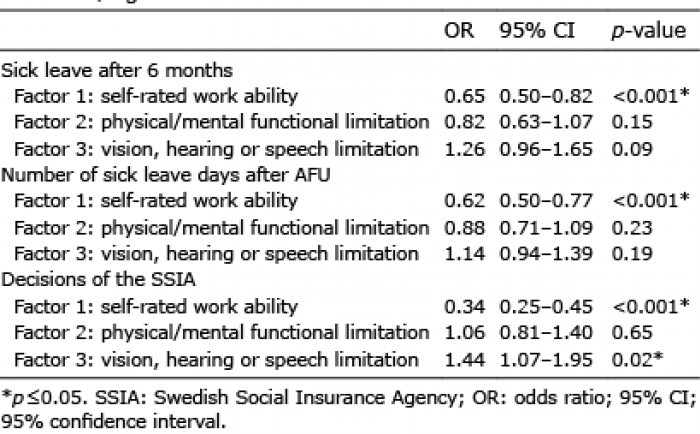 Click to show fullsize
Click to show fullsize