
From the 1Department of Rehabilitation Medicine, Tokyo Medical and Dental University and 2Department of Pediatrics, Akitsu Ryoiku-en, Tokyo, Japan
Objective: To determine bone quality in adults with severe motor and intellectual disabilities.
Design: A retrospective cohort study.
Patients: Bone quality of 60 patients with severe motor and intellectual disabilities (28 men, 32 women; mean age 57 years) at a long-term care facility for adults was examined retrospectively.
Methods: Quantitative ultrasonography was used to measure the stiffness index, T-score and Z-score of the calcaneus. A multiple linear regression model, including sex, age, anti-epileptic drug use, tube-feeding status, and current and peak physical abilities, was used to identify significant predictors of T-scores.
Results: Quantitative ultrasonography revealed that all patients had lower bone quality (based on T-scores, Z-scores, and stiffness index), and all patients had T-scores with standard deviations (SD) below 1.8. Current physical ability, age, and anti-epileptic drug use were significant factors in T-score determination, while tube-feeding and peak physical ability were not. The ability to walk without assistance was the most significant predictor in quantitative ultrasonography.
Conclusion: Severely low bone quality is observed in patients with severe motor and intellectual disabilities; and it is strongly associated with current physical activity. It is important that patients with severe motor and intellectual disabilities preserve their physical abilities to prevent osteoporosis- related fractures.
Key words: osteoporosis; disabled person; physical ability; ageing; bone quality; fracture; anti-epileptic drug; ultrasound.
Accepted Dec 29, 2020; Epub ahead of print Jan 15, 2021
J Rehabil Med 2021; 53: jrm00152
Correspondence address: Tomoko Sakai, Department of Orthopedics, Tokyo Medical and Dental University, Tokyo, Japan. E-mail: t_sakai.orth@tmd.ac.jp
Doi: 10.2340/16501977-2789
Fractures are common in adults with severe motor and intellectual disabilities. This study assessed the bone quality of 60 individuals from young adult to advanced age. All patients had low bone quality from a young age, and current physical ability, age, and anti-epileptic drug use were factors affecting bone quality, while tube- feeding and peak physical ability were not. Severely low bone quality in patients with severe motor and intellectual disabilities is strongly associated with current physical activity levels. It is very important for patients with severe motor and intellectual disabilities to increase and preserve their physical activities and abilities, respectively, to prevent osteoporosis-related fractures.
The high rate of osteoporosis in children and adults with severe motor and intellectual disabilities (SMID) is an established problem, with a reported yearly incidence of fractures of approximately 2–3% among institutionalized patients, with differences among institutions (1,2). In cases involving primary osteoporosis, lower levels of female hormones during the postmenopausal stage in female patients increase the rate of bone resorption, resulting in decreased bone density (3). In patients with SMID, bone quality examined by quantitative ultrasonography (QUS) does not increase with growth and remains low throughout the person’s lifetime (4).
Use of anti-epileptic drugs, palsy type, gait dysfunction, and low bone density have been reported as risk factors for fractures in patients with cerebral palsy (CP) (5). Stevenson et al. observed that higher body fat, gastrostomy, and previous fractures also increased the risk of future fractures (6). Mergler et al. observed that eating disorders, previous fractures, and thinness of subcutaneous fat were risk factors for fractures in patients with CP (7). Secondary osteoporosis in the context of SMID is modulated by factors other than those affecting primary osteoporosis; the most probable cause of low bone quality in such patients is physical ability related to skeletal unloading (8).
Progressive medical advances and increasing knowledge of the management of CP have helped individuals with CP to live longer with their impairments (9, 10). The mean age of patients with SMID in Japan has increased steadily as a result of patient ageing under the advanced medical care that became well-established in many institutions in the 1960s, although the individual survival rate of patients housed in public and private institutions in Japan has not improved since the 1960s (11). Throughout an individual’s lifespan, physical abilities change, not only in the growth stage, but also in the ageing stage. This suggests the need to consider possible changes in the bone quality of patients with SMID.
There is limited research on osteoporosis in elderly patients with SMID. The aim of this study was to measure the bone quality of elderly adults with SMID and identify factors associated with bone quality, in order to determine the appropriate treatment approach to prevent fractures in patients with SMID.
Participants
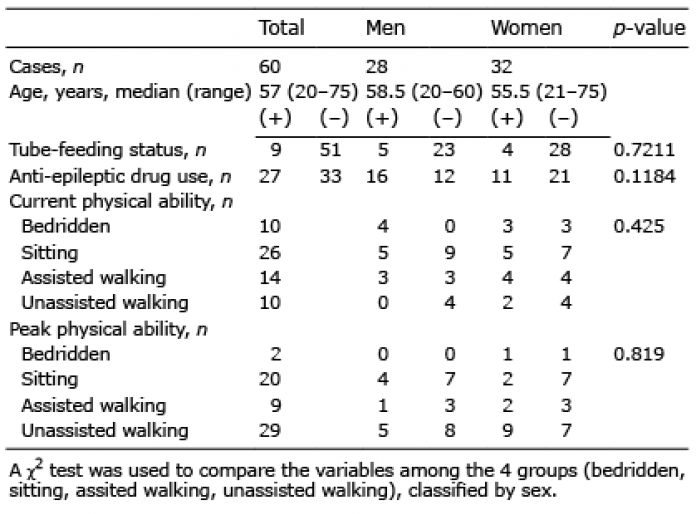
This study included 60 patients (28 men, 32 women; median age 57 years [range 20–75 years]) who were residents at the Akitsu Ryoiku-en (Tokyo, Japan), a facility that provides long-term care for individuals with SMID from childhood through adulthood (Table I).
Table I. Patients’ characteristics
Measurements
Quantitative ultrasonography (QUS) was used to evaluate each patient’s bone quality and bone mass in the annual health check held in the spring of 2020, and these data were used for the analysis. The osteoporosis guidelines recommend the use of dual-energy X-ray absorptiometry (DXA) to evaluate bone mass, and QUS to evaluate bone quality and bone mass. QUS devices supposedly represent an acceptable alternative method to DXA to assess bone health, and most QUS parameters are significantly correlated with DXA outcomes (12, 13). Because we did not have access to DXA, calcaneal QUS parameters were used to assess bone health.
The non-dominant foot is recommended for testing; however, people with SMID found it difficult to conclusively identify their non-dominant foot. Therefore, bilateral calcaneal QUS parameters were measured, and the mean value between the left and right sides were measured using an A-1000 EXP II (GE Health Care Japan, Tokyo, Japan). The angle of the device that held the patient’s heel could be changed to position the heel as horizontally as possible; this is because the ankle joints of patients with SMID are sometimes deformed or display contractures. In the few cases with one-sided joint deformity, the affected side could not be measured.
Ultrasound devices routinely measure 2 parameters: broadband ultrasound attenuation (BUA) and speed of sound (SOS). BUA is determined by mechanisms of diffraction, scattering, and absorption in the bone, marrow and soft tissue. Furthermore, SOS is influenced by the elasticity of the bone as well as its density. The additional ultrasound variable derived from the mathematical combination of both BUA and SOS is defined as the stiffness index (SI). The SI is associated with bone density obtained using bone-density measuring equipment with conventional DXA methods (14). The acquired value of SI was correlated with that of a young sex-matched population with peak bone mass or the mean age of the population.
In addition to SI, QUS-derived T-scores and Z-scores were calculated. The T-score scale considers the mean value of a young sex-matched population with the peak bone mass as 0 with 1 standard deviation (SD), whereas that of the Z-score considers the mean age of a population as 0 with 1 SD. The T-score is defined as the number of SDs from the mean for healthy young adults, whereas the Z-score is the number of SDs compared with the mean for healthy adults of the same age. The T-score level of ≥ 1 by DXA was defined as “normal” by the World Health Organization (WHO); the T-score level of −2.49 to −1 by DEXA was defined as osteopaenia, and the T-score level of ≤ −2.5 by DEXA was defined as osteoporosis (15). For the 3 QUS parameters used in this study, a T-score threshold of −1.80 would result in the same percentage of postmenopausal women classified as osteoporotic as the WHO threshold for bone quality measurements (16).
Statistical analyses
Patients were categorized into male and female groups. The χ2 test was used to compare variables, including tube-feeding status, anti-epileptic drug use, and current and peak physical ability, among these groups.
Patients were separated into 4 groups according to current physical ability: bedridden, ability to sit, ability to walk with assistance, and ability to walk without assistance. The analysis of variance (ANOVA) test was used to compare the SI, T-scores, and Z-scores among the 4 groups. A post hoc analysis was conducted using the Tukey method to determine significant differences. A multiple linear regression model, which included sex, age, anti-epileptic drug use, tube-feeding status, and current and peak physical ability, was used to identify significant predictors of T-scores. Values of p < 0.05 were considered statistically significant, and all statistical analyses were performed using BellCurve for Excel 2016 (Social Survey Research Information Co., Ltd, Tokyo, Japan).
Ethics statement
This study was conducted with approval from Akitsu Ryoiku-en’s board of ethics in January and February 2020, and it conformed to the principles of the Declaration of Helsinki. Written informed consent was obtained from the guardians of all subjects.
The clinical diagnoses leading to the SMID classification were CP (n = 28), developmental disability (n = 14), encephalitis (n = 10), genetic abnormalities (n = 4), intracerebral haemorrhage (n = 3), and neurodegenerative disease (n = 1). In all patients, SMID began in the neonatal period, infancy, or adolescence. The following categories of physical ability were used: bedridden, ability to sit, to walk with assistance, and to walk unassisted. In our cohort, 10 patients were bedridden, 26 required a wheelchair, 14 could walk with assistance, and 10 could walk unassisted. The peak physical abilities of patients were as follows: 2 were bedridden, 20 were able to sit, 9 could walk with assistance, and 29 could walk unassisted. In total, 9 patients were tube-fed. In cases of combined oral and tube feeding, the primary mode was recorded. Overall, 27 patients used the following anti-epileptic drugs: phenobarbital (n = 19), phenytoin (n = 4), carbamazepine (n = 12), and primidone (n = 1). Of the 27 patients who used anti-epileptic drugs, 18 used singular drugs, and 9 patients combination drugs. None of the subjects had previously been treated for osteoporosis with vitamin D, vitamin K, bisphosphonates, or teriparatide.
The use of tube feeding and anti-epileptic drugs did not differ significantly between men and women (Table I). QUS parameters were extremely low. The QUS revealed that all patients had low bone quality evidenced by the T-scores, Z-scores, and SI, and all patients had a T-score with an SD below 1.8.
Regarding SI, Z-scores, and T-scores, significant differences were observed among the 4 groups according to current physical ability (p < 0.001) (Table II). The post-hoc test revealed that the QUS values were significantly higher in patients who could walk (with or without assistance) than those who could sit or who were bedridden.
Table II. Stiffness, Z-score, and T-score determination by physical ability grouping
Multiple regression analysis was performed, with T-score as the dependent variables; and sex, age, tube feeding status, current or peak physical ability, and anti-epileptic drug use as independent variables (Table III). The adjusted R2 was 0.4602, and the significant difference was p < 0.001. After controlling for sex, age, the use of anti-epileptic drugs, tube-feeding, and current and peak physical ability, current physical ability (p < 0.001, partial regression coefficient: 5.3311) showed significantly positive β-coefficients for T-score and age (p < 0.01, partial regression coefficient −0.0253) and anti-epileptic drug use (p < 0.01, partial regression coefficient: –0.4469). Sex, tube-feeding, and peak physical ability were not significant factors.
Table III. Multiple linear regression analysis, using T-score as a dependent variable, and sex, age, anti-epileptic drugs use, tube feeding, current loading, and peak loading as independent variables
This study investigated calcaneal QUS measures of osteoporosis in patients with SMID. In a cohort of bedridden patients from a different institution, we had previously reported that the bone quality examined by QUS of patients with SMID was consistently low from a young age (4).
All calcaneal QUS parameters differed significantly among the groups according to current physical ability; they were significantly higher in patients who could walk (with or without assistance) than in the ability to sit or bedridden groups. In multiple regression analysis, current physical ability, age, and anti-epileptic medications use were probable predictors of bone quality, and current physical ability was the strongest predictor.
To obtain higher bone quality during growth and to maximize peak physical ability, it is important to remain physically active. In the growth period at the end of adolescence, bone metabolism normally has high turnover, and BMD increases gradually to the peak in children and adolescents (17). Exercise is necessary for maintaining good bone quality during the growth period (18). Non-walkers with CP have been observed to have lower mean BMD Z-scores than walkers with CP, and among CP walkers, BMD Z-scores of the distal femur were lower depending on the degree of neuromotor impairment. Furthermore, the bone quality of the affected limb in children with hemiplegia was lower than that of the non-affected limb (8).
Because patients with SMID are living longer at present, it is necessary to maintain their physical ability for as long as possible and to continue bearing weight on the lower extremities to maintain high bone quality. To accomplish this, it is essential to provide rehabilitation therapy to maximize peak bone mass and maintain peak physical ability to maximize bone quality, as old age approaches. For patients who can only sit or were bedridden, daily stimulation using anti-gravity or sitting devices may be essential.
Age was a predictor of bone quality, and current physical ability was the strongest predictor. We reported previously that bone resorption markers in female patients with SMID increased beyond 50 years of age, possibly representing a sign of primary osteoporosis (4). The existence of primary osteoporosis could be an influencing factor, although it is unclear in this study. The loss of physical ability, and primary osteoporosis, may be related to age. Hence, further research is necessary to investigate primary osteoporosis with SMID to identify bone metabolic markers and follow the course of bone quality in patients with SMID.
Anti-epileptic medication use was a probable predictor of bone quality. It has been reported that all anti-epileptic drugs (new and old) affect bone mineral status in children who have received therapy for more than 6 months, and children taking anti-epileptic drugs for longer durations (≥ 2 years) showed more severe side-effects in terms of bone quality (19, 20). Abnormalities of calcium metabolism supposedly result from the cytochrome P450 enzyme-inducing properties of some anti-epileptic drugs and the resultant reduction in vitamin D levels; however, the effect of many medications (e.g. valproate) cannot be readily explained by vitamin D metabolism, and vitamin D administration is recommended in children with epilepsy receiving anti-epileptic drugs for more than 24 months (21, 22). It is not only older P540 cytochrome antiepileptic drugs that affect bone quality (23). Further research is needed to assess vitamin D deficiency in SMID patients by measuring serum 25(OH)D levels and evaluating the effectiveness of vitamin D supplements in the treatment of osteoporosis in patients with SMID to prevent related fractures.
No significant differences were observed among the groups regarding the tube feeding status. We reported previously that tube feeding was a substantial predictor for low bone quality in bedridden patients with SMID (4). Many reports have found that tube feeding is a risk factor for low bone quality in patients with CP (7, 8). The current study did not have sufficient data to investigate the relationship between low bone quality and tube feeding, because physical ability was the major factor affecting QUS in our study.
This study has some limitations. First, we could not measure BMD directly using DXA since the analytical equipment required was not available. Nevertheless, most QUS parameters are significantly correlated with DXA outcomes; therefore, the results can be considered accurate. Secondly, this was a single-centre study and may be subject to selection bias. Therefore, multi-centre studies are needed to validate the current findings. Thirdly, this study did not differentiate groups based on tube-feeding status, and this may have different effects on bone metabolism. It is necessary to obtain more samples regarding tube-feeding, as this study included only 9 cases of tube-feeding patients out of 60 cases. Finally, SMID is a Japanese social welfare concept and may be an inappropriate concept for medical science. It includes a wide range of encephalopathies, from severe brain damage to profound intellectual disability with light motor disability. It is, therefore, necessary to conduct further studies on the classification and the separate examination of the types of encephalopathy in patients with SMID.
In conclusion, reduced physical ability was the strongest risk factor for low bone quality in patients with SMID. Regarding skeletal unloading, institutionalized patients need to engage in as much physical activity as possible and maintain a high level of activity for as long as possible, particularly because the lifespans of patients with SMID are increasing.
The authors thank Ms Eriko Tamura, Ms Miki Ohtake and Ms Masayo Morisawa, who kindly helped collect data. We also express our deep gratitude to Ms Masako Akiyama, URA, Research Administration Division, Tokyo Medical and Dental University, who performed the statistical review and commented on the data.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize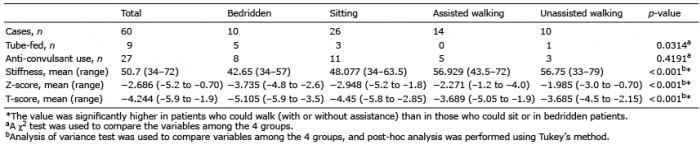 Click to show fullsize
Click to show fullsize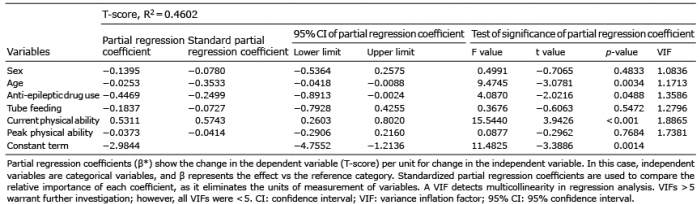 Click to show fullsize
Click to show fullsize