
From the 1Department of Orthopaedics, and 2Rehabilitation Centre, Eksjö, Region Jönköping County and Department of Biomedical and Clinical Sciences, Linköping University, Linköping, Sweden
Objective: To compare the effects of two postoperative regimens following carpal tunnel release; plaster casting and elastic bandaging.
Design: A randomized controlled study.
Patients: Patients with carpal tunnel syndrome and planned surgical carpal tunnel release were invited to participate.
Methods: A total of 94 patients were randomized to either plaster casting or elastic bandaging to be used 2 weeks postoperatively. Muscle strength, pain rated on a visual analogue scale, range of movement, sensibility, oedema, and different scores regarding symptoms and function were measured before and 2, 4, 6, 8 and 26 weeks after surgery.
Results: No differences were found between the 2 groups for any measurement, except for the DASH (Disability of the Arm, Shoulder and Hand) Health Score and daily function, rated 2 weeks postoperatively, in which the bandage group scored better. Both groups improved significantly over time for all measurements, sensibility was improved after 2 weeks, while strength was not fully recovered until week 26.
Conclusion: Following carpal tunnel release no benefits were found in using plaster casting, compared with elastic bandaging. Among these patients there was more discomfort during plaster casting compared with elastic bandaging; therefore plaster casting is not recommended following this type of surgery.
Key words: carpal tunnel syndrome; hand strength; range of motion; rehabilitation; self-assessment.
Accepted Dec 21, 2020; Epub ahead of print Jan 14, 2021
J Rehabil Med 2021; 53; jrm00168
Correspondence address: Björn Alkner, Department of Orthopaedics, Höglandssjukhuset District Hospital, SE-575 81 Eksjö, Sweden. E-mail: bjorn.alkner@liu.se
Doi: 10.2340/16501977-2788
No clear consensus exists regarding benefits of use of plaster casting following carpal tunnel release. This study aimed to compare two different postoperative regimens in a randomized controlled study. A total of 94 patients were randomized to either plaster casting or elastic bandage to be used for 2 weeks after surgery for carpal tunnel release. Muscle strength, rated pain, range of movement, sensibility, oedema, and different scores regarding symptoms and function were measured before and 2, 4, 6, 8 and 26 weeks after surgery. No differences were found between the 2 groups for any measurement, except for health score and rated daily function 2 weeks postoperatively, in which the bandage group scored better. Both groups improved significantly over time for all measurements, sensibility was improved after 2 weeks, while strength was not fully recovered until week 26. This study found no benefits, but some disadvantages, of plaster casting following carpal tunnel release, and therefore plaster casting is not recommended for these patients.
Following open carpal tunnel release surgery, volar or dorsal plaster casting is sometimes used for a few weeks. However, the use of plaster casting is questioned and, frequently, an elastic bandage alone is used (1, 2). The benefit of casting is considered to be unloading of the surgical site and the nerve, thus facilitating healing and promoting pain relief (3). On the other hand, an elastic bandage is thought to enable early movement training to counteract stiffness and promote more rapid restoration of hand function (2).
Previous studies have found no significant difference between the postoperative methods concerning function (4, 5), pain (6, 7), hand strength (7), sensibility (8), complications (5, 7, 8), and continuing symptoms using self-assessment (3, 4, 8, 9), while more pain and impaired strength with plaster casting in the short term was indicated in one study (5). Many previous studies had a limited number of patients and showed wide disparity regarding the number of days with a cast (2–21 days), the degree of mobilization of patients without a cast, treatment procedures, follow-up time-points and outcome measures (4–8, 10). Hence, a need for a prospective randomized multifactorial study that evaluates rehabilitation with or without cast treatment following carpal tunnel release has been proposed (9, 11). As the evidence is not clear, and plaster casting following carpal tunnel surgery is still in use at hospitals in Sweden, a randomized controlled study was necessary. In fact, the differences in clinical practice among hospitals in our region led to the initiation of this study.
The aim of this study was to examine the rehabilitation process with or without the use of plaster casting, following carpal tunnel release, regarding strength, pain, flexibility, sensibility, swelling and self-rated function, with grip strength as the primary outcome measure. It was hypothesized that there would be no significant differences between the groups regarding any of these parameters.
Subjects
The study was performed at the Orthopaedic Department, Höglandssjukhuset Regional Hospital, Eksjö, Region Jönköping County, Sweden. Patients scheduled for surgical carpal tunnel release, after fulfilling inclusion, but not exclusion, criteria, and after receiving written and oral information about the study were invited to participate by the orthopaedic surgeon. Inclusion criteria were: carpal tunnel syndrome diagnosed by an orthopaedic surgeon by clinical assessment with or without neuro-physiology tests and planned surgical carpal tunnel release. Exclusion criteria were: other pain disorders involving the forearm or hand, such as fibromyalgia, rheumatic disorders or osteoarthritis. Patients gave their oral and written informed consent to participate in the study. The study was approved by the ethics committee in Linköping, Sweden, was conducted according to the principles of the Declaration of Helsinki, and was subject to the laws of Sweden. The study design was not changed during the course of the study.
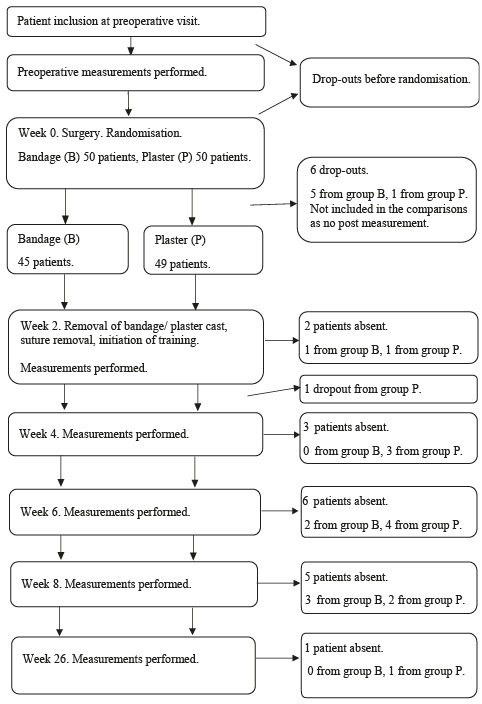
Subjects dropped out due to comorbidity, moving to another area and administrative failures. Dropouts before randomization, which occurred during surgery, were replaced. A total of 100 patients were randomized to the 2 groups; 50 in each group. After dropouts, a total of 94 patients were included in the comparisons. A few patients in each group missed some of the measurements, as shown in the study flowchart (Fig. 1). The time-points for these subjects were not included in the comparisons and no imputation of data was performed.
Six included patients were also operated for carpal tunnel release on the contralateral hand (2, 2, 4, 6, 6 and 9 months postoperatively) and were registered as new included patients. Three of these patients had a plaster cast bilaterally, 1 had an elastic bandage both times and 2 had a plaster cast the first time and an elastic bandage the second time.
Fig. 1. Study flowchart. B: elastic bandage group; P: plaster casting group.
Intervention
The patients underwent surgery using standardized open surgery. Randomization was performed in the operating room during wound closure, thus the surgeon was blinded to the randomization during surgery. All wounds were sutured with single stitches (5.0 Ethilon®, Ethicon, Johnson & Johnson, New Brunswick, NJ, US) and covered with Atrauman® (Hartmann, Heidenheim, Germany), folded gauze and a sterile elastic wrap. In addition, the bandage group had a regular elastic bandage, while the plaster cast group had a dorsally placed plaster cast, which locked the wrist, but not the metacarpophalangeal (MCP) joints, and was wrapped with an elastic bandage (Fig. 2). A nurse at the orthopaedic outpatient ward removed the cast, dressings and sutures 2 weeks postoperatively. Measurements were performed consecutively by an occupational therapist who was blinded to the groups. This therapist also gave the patient instructions on how to train and use their hand in daily activities following the surgery. This included flexibility training and instruction not to load the hand heavily until 6 weeks, except during isometric testing.
Fig. 2. Elastic bandage (left) and plaster cast (right) performed pos-surgery
Data collection
Measurements were performed before and 2, 4, 6, 8 and 26 weeks following surgery, in the order listed below. Two licensed occupational therapists conducted all the tests.
Strength. All strength tests were performed 3 times and the best effort was chosen for further comparisons. The test leader used a standardized verbal instruction to encourage the subject to make maximal effort.
Grip and pinch strength was measured with the upper arm resting against the upper body, the elbow at 90° flexion, the hand in a neutral position, and with the test leader holding a hand under the dynamometer. Grip strength was measured using a Jamar dynamometer (Pattersson Medical, Warrenville, IL, USA) (12). Tip pinch using the thumb and digit 2, palmar pinch using the thumb vs digit 2 and 3, and key pinch using the thumb and the middle phalanx of digit 2 were measured using a pinch gauge (PG-60 Mechanical pinch gauge, B&L Engineering, Santa Ana, CA, USA). The measurements were performed in accordance with the manual of the Swedish national hand surgery registry (Handkirurgiskt Kvalitetsregister; HAKIR) (13).
Flexibility. Active range of motion (ROM) was assessed using a manual goniometer according to HAKIR. Wrist flexion and extension were examined with the elbow flexed, the lower arm in a neutral position, and the fingers relaxed. The fixed shank was placed radially and parallel to the radius and the moveable shank was placed radially and parallel to the second metacarpal bone.
Ulnar and radial deviation over the wrist were examined with the forearm resting in a pronated position against the surface of the table, with 0° extension/flexion. The fixed shank was placed dorsal, parallel to the forearm, and the moveable shank was placed dorsal and parallel to the centre of the third metacarpal bone.
The distance between the finger-tips and the palm of the hand when maximally flexing the fingers was measured using a ruler with flexion of fingers, the lower arm in a neutral position, and the wrist in 0–30° extension (14).
Swelling. Hand oedema was measured according to the figure-of-eight method (15). A tape measure was placed distally and obliquely across the dorsal side of the hand, over the midpoint of the second metacarpal head. Then the tape measure was drawn in an ulnar direction across the palmar surface with the distal edge aligned with the palmar digital crease of the fifth digit. The distal edge of the tape measure was realigned with the distal crease and directed back to the starting point dorsally, near the tendon of the abductor pollicis longus.
Sensibility. Sensibility was tested using Semmes-Weinstein monofilament (North Coast Medical, Inc., Morgan Hill, CA, USA), including 5 standardized filaments, numbered 1–5 where 1 represents normal sensibility and 5 no protective sensibility. Starting with the thinnest monofilament, each filament was applied 3 times at the fingertip. The number of the thinnest monofilament that the patient could detect was registered (16, 17). The radial and ulnar sides of all digits were tested and the mean value of all these was used for further comparisons.
Scar. The width of the scar was measured using a ruler.
Self-evaluation. Patients answered the following questionnaires in the order described.
Patients rated pain during loading, pain during motion without load, pain during rest, stiffness, weakness, numbness/tingling, sensitivity to cold and ability to perform daily activities using a visual analogue scale (VAS) (18, 19) in accordance with the HAKIR manual. Patients placed a mark on a line measuring 100 mm, where 0 represented absence of symptoms and 100 the most possible symptoms. The distance from 0 to the mark was measured in mm using a ruler.
The EQ-5D (EuroQol five-dimension scale) health status thermometer was used (but not the other EQ-5D questions). Patients were asked to grade their health on a scale ranging from 0 to 100, with 100 representing the best possible sense of health (20).
Disabilities of the Arm, Shoulder and Hand (DASH) Health included questions concerning everyday activities, pain and numbness during the past week (21, 22). Symptoms were graded on a scale of 1–5, with 1 representing no difficulties or symptoms, and 5 representing grave dysfunction. The sum of all the 11 answer ratings was used for further statistical evaluation.
Patient-Related Wrist Evaluation (PRWE) included questions concerning pain and function during everyday activities during the past week (23–25). The sum of 5 answer ratings concerning pain and 10 answer ratings regarding function were analysed separately; in addition the sum of all answer ratings was weighed and analysed.
The carpal tunnel syndrome (CTS) questionnaire concerned daily function during common activities, as well as symptoms such as pain and numbness during the past week (26, 27). The mean values for the different questions regarding function and symptoms are presented, as well as the total mean values.
Statistical analysis
The number of patients was decided after a power calculation on the primary outcome measure grip strength. It was calculated based on reported normal values in the estimated year span (28). A difference of more than 5 kg was considered clinically relevant and implied a 5% risk of a type I error and a 20% risk of a type II error with 31 patients in each group. To compensate for dropouts, and for possible larger variation in the study material, 50 patients were included in each group. This number of patients was estimated as sufficient even for the other outcome measures and was in accordance with similar studies.
Strength, flexibility, sensibility and swelling data were analysed with a repeated measure analysis of variance (ANOVA) using a statistical Software (Statistica, TIBCO Software Inc., Palo Alto, CA, USA). Data are shown as mean (standard deviation; SD). The difference between groups regarding scar width at week 26 was analysed with a Student’s t-test.
For the DASH, PRWE and CTS questionnaires non-parametric statistical methods were used, also using Statistica. A Mann–Whitney U test detected differences between groups and Wilcoxon matched paired tests were used to detect differences over time from initial values. Data are shown as median values.
For VAS and EQ-5D, data changes between the different time-points were analysed using Svensson’s method for analysing paired ordered nominal data (29). An Excel macro was used to perform the analyses (30). In short, the results are presented as follows: percentage agreement (PA): the percentage (proportion) of answers that are identical at baseline and follow-up among the patients. Relative position (RP): the systematic change in the cumulative frequency of answers between baseline and follow-up. Relative concentration (RC): this determines if the marginal distribution at follow-up has a higher concentration of central response alternatives than the marginal distribution at baseline. Relative rank variance (RV): a variance measure of the individual variation, in ranks between baseline and follow-up 0 ≤ RV ≤ 1. Higher values of RV, over 0.20 can be seen as a sign of more individual deviation from a common change pattern. RP, RC and RV are shown with 95% confidence intervals (95% CI). If the CI for RP and/or RC does not contain 0, then RP and RC are considered to be statistically significant. If the confidence intervals for groups E and C are not overlapping, a significant difference between groups is assumed. For a more detailed description, see the references quoted above. These data are shown as median values.
Group characteristics are shown in Table I.
Strength, flexibility, swelling, sensitivity and scar width
All results are shown in Table II. There were no significant group-by-time interactions regarding any of the measurements of strength, flexibility, swelling or sensitivity. However, time factors were significant. Thus, subjects are treated as a single group to determine differences over time.
Grip and palmar pinch strength were still significantly lower 8 weeks postoperatively compared with pre-surgery, while key pinch and tip pinch strength were recovered at 8 and 6 weeks, respectively. At week 26 they were slightly stronger than before surgery measurements.
Table I. Group characteristics
Table II. Physical measurements
All flexibility measures were significantly impaired postoperatively, radial and ulnar deviation ROM was recovered after 6 weeks, and wrist flexion and wrist extension ROM after 8 weeks. Hand oedema increased modestly following surgery, reaching statistical significance compared with pre-surgery after 8 weeks, but the modest change is of no clinical relevance.
Fingertip-palm-distance was 0 mm for almost all subjects. Only 7 patients in the elastic bandage group (5–30 mm) and 4 patients in the plaster cast group (4.5–25 mm) had a distance > 0 mm, and in all cases, this had returned to 0 at the latest 8 weeks postoperatively.
At 2 weeks post-surgery there was already significant improvement in sensitivity compared with pre-surgery. Further significant improvement was shown between weeks 2 and 4 and also 6 and 8.
The width of the scar measured at week 26 did not differ between groups.
Self-evaluation
All results are shown in Table III.
VAS measurements. There were no differences between groups concerning pain during loading (Fig. 3), motion pain without load, resting pain, stiffness, weakness, numbness/tingling, or sensitivity to cold. The plaster cast group experienced significantly more difficulties in ability to perform daily activities 2 weeks post-surgery compared with the elastic bandage group, but no significant differences were detected between groups after that time-point (Fig. 4).
Table III. Self-evaluation
Fig. 3. Median visual analogue scale (VAS) scores for pain during loading, pre-, 2, 4, 6, 8 and 26 weeks after surgery. Pre: preoperative; Bandage: elastic bandage group; Plaster: plaster cast group. Median; box: 25–75%; whisker: non-outlier range.
Fig. 4. Median visual analogue scale (VAS) scores for ability to perform daily activities, pre-, 2, 4, 6, 8 and 26 weeks after surgery. Pre: preoperative; Bandage: elastic bandage group; Plaster: plaster cast group. Median; box: 25–75%; whisker: non-outlier range.
Both groups experienced significant improvement concerning numbness and tingling and sensitivity to cold 2 weeks post-surgery, and ability to perform daily activities was significantly better at 4 weeks post-surgery. The improvement persisted in all subsequent measurements. All 94 patients showed decreased symptoms of numbness/tingling at 26 weeks postoperatively (Fig. 5). Further statistical information from the Svensson method is shown in Table IV.
Fig. 5. Median visual analogue scale (VAS) scores for numbness and tingling pre-, 2, 4, 6, 8 and 26 weeks after surgery. Bandage: elastic bandage group; Plaster: plaster cast group. Median; box: 25–75%; whisker: non-outlier range.
Table IV. Statistical analyses of visual analogue scale (VAS) scores
Table IV. Cont.
Questionnaires. At week 2 EQ-5D health status thermometer scores were already improved for both groups, and the improvement persisted in all subsequent measurements. No differences were found between groups (for further statistics see Table V).
DASH scores were significantly better for the elastic bandage group at week 2, but not at the other time-points (Fig. 6). There were no differences between the groups regarding the PRWE and the CTS questionnaire. All scores improved over time for both groups.
Table V. Statistical analyses of EuroQol five-dimension (EQ-5D) scale scores
Fig. 6. Disabilities of the Arm, Shoulder and Hand (DASH) Health score during the past week pre-, 2, 4, 6, 8 and 26 weeks after surgery. Bandage: elastic bandage group; Plaster: plaster cast group. Median; box: 25–75%; whisker: non-outlier range.
This randomized, controlled study found no significant advantages of plaster casting following carpal tunnel release regarding any of the parameters measured, compared with elastic bandaging. These data are in agreement with previous studies, even though ambiguous results exist concerning strength and pain early after surgery when comparing the 2 methods (5–7, 31, 32). There were no significant differences between the 2 groups regarding muscle strength and pain in the current study. However, DASH health score, including questions about function and pain, and the VAS score of the ability to perform daily activities, were both compromised in the plaster group compared with the bandage group 2 weeks postoperatively. This shows that the cast has an inhibiting function during treatment, but no longstanding effect, as the groups were equal again at week 4. Nor was there any difference between groups regarding the width of the scars, suggesting no major positive effect of plaster casting on wound healing. However, no detrimental effect of casting on flexibility was shown. Thus, there are no benefits of plaster casting following carpal tunnel surgery, but there are negative effects on performance during casting. Plaster casting also takes extra time and entails extra cost. Therefore, we recommend that casting should not be used postoperatively. However, as some subjects stated that they felt safer with a plaster cast, there is no strong reason not to use plaster cast if a patient specifically requests one.
This study also provides a good picture of the rehabilitation process following carpal tunnel surgery. Full grip or palmar pinch strength had not been regained in the groups 8 weeks postoperatively, while tip and key pinch strength recovered after 6 and 8 weeks, respectively. These tendencies have also been implied by previous studies (5, 7). Why it takes this long for strength to recover to preoperative levels may depend on various factors, including weakening of the structures in the wrist after surgery, pain, and caution on both the training and measurement occasions, although patients are encouraged to use maximum force during tests. However, both groups experienced a significant improvement in ability to perform daily activities after only 4 weeks and the strength decrements after week 4 are probably not of major clinical importance. After 26 weeks, both groups were slightly, but significantly, stronger than before surgery. This can be explained by release of pain, healing of the structures and postoperative training, but also by improved stimulation of the muscles due to recovery of the nerve, as the median nerve-innervated thenar muscles greatly contribute to force production (33, 34).
Sensibility was improved postoperatively, with no significant differences between groups, in agreement with previous studies (7, 8, 35, 36). Postoperative sensibilty was significantly improved after 2 weeks and improved continuously up to week 8, suggesting early recovery of the nerve, in accordance with previous data (8, 33, 37). This also correlated well with the patients’ self-rating, in which both groups experienced significant improvement concerning numbness, tingling and sensitivity to cold 2 weeks after surgery. All patients experienced fewer of these cardinal symptoms of carpal tunnel syndrome at 26 weeks. There was also a successive improvement over time in all the self-evaluation scores used, in accordance with earlier data (35, 38). Altogether, these data suggest good results from surgical carpal tunnel release, in accordance with previous studies (11, 31, 39, 40), supporting the use of surgery for patients with carpal tunnel syndrome.
This study aimed to evaluate many different aspects of hand function in order to elucidate any possible differences between these postoperative regimens. The study also aimed to examine different time-points of early rehabilitation in order to obtain a better picture of the rehabilitation process for these 2 regimens. We are aware that by making so many measurements and comparisons, the risk of detecting differences that do not exist increases. However, almost no differences were found between the groups. Thus, this strengthens the hypothesis that there is no major difference between these 2 post-surgery treatments.
A bulkier post-surgery bandage is also in use at several places, and it could be argued that this should have been included in a third arm of the current study. However, this would have required the recruitment of many more patients, with small benefits for the study. As no major differences were found for any of the measured outcomes, it is extremely unlikely that a bulky bandage, which is in-between these regarding immobilization, would have resulted in a different response.
This study considered each carpal tunnel surgery as a single case, and a few included patients had surgery on both hands. In these cases, as the second surgery was performed before the last follow-up, it could potentially affect the answers regarding global health and daily function at this time-point. However, these patients were instructed to focus on the hand that most recently had surgery when answering the questionnaires, for the hand-specific measurements this circumstance should be of no importance. A large number of patients fulfilling the inclusion criteria declined to participate, most commonly due to the long distance of travel to the hospital or lack of time. However, we consider that the study sample is representative, and the sex distribution is equal to previous studies (41).
In conclusion, this study found no advantage of using a plaster cast compared with an elastic bandage after carpal tunnel release, as regards either functional measurements or the patients’ experiences. Plaster casting, however, provokes some negative effects on perceived performance and symptoms during the casting period. Therefore, the use of plaster casting following carpal tunnel release is not indicated.
The authors are grateful to Mats Nilsson for statistical support, Maj Nilsson for administrative assistance, all involved colleagues and other staff at Höglandssjukhuset District Hospital for their valuable contributions, and all the patients who participated in the study.
This project was funded by grants from Futurum – the Academy for Health and Care, Region Jönköping County, Sweden.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize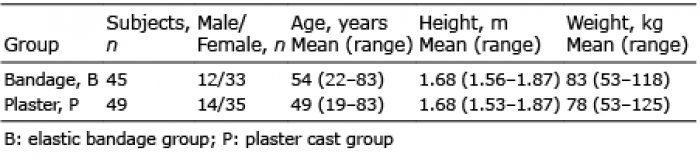 Click to show fullsize
Click to show fullsize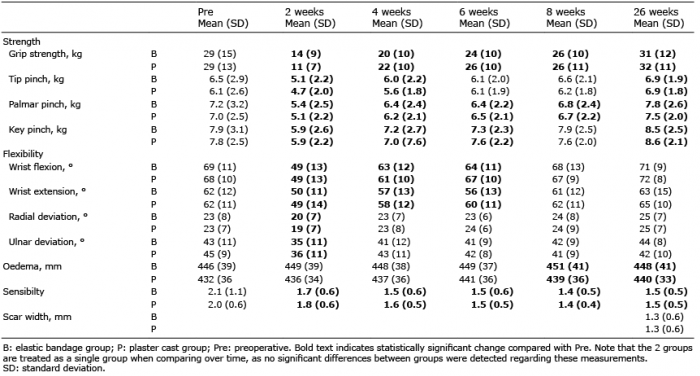 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize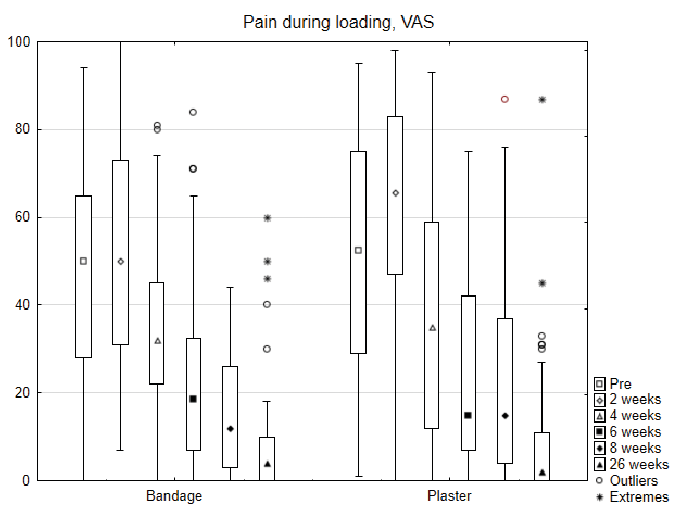 Click to show fullsize
Click to show fullsize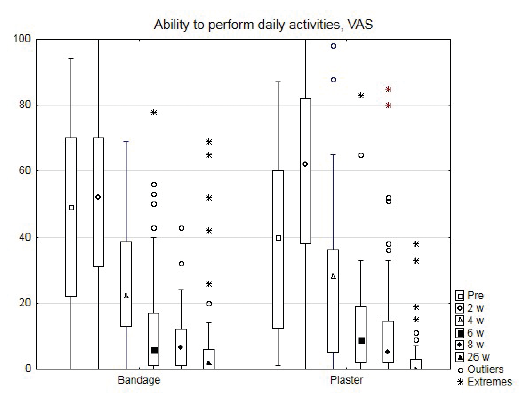 Click to show fullsize
Click to show fullsize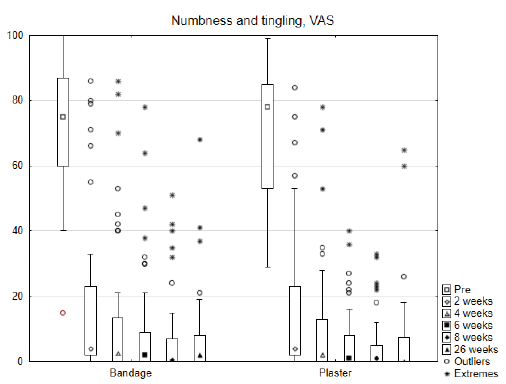 Click to show fullsize
Click to show fullsize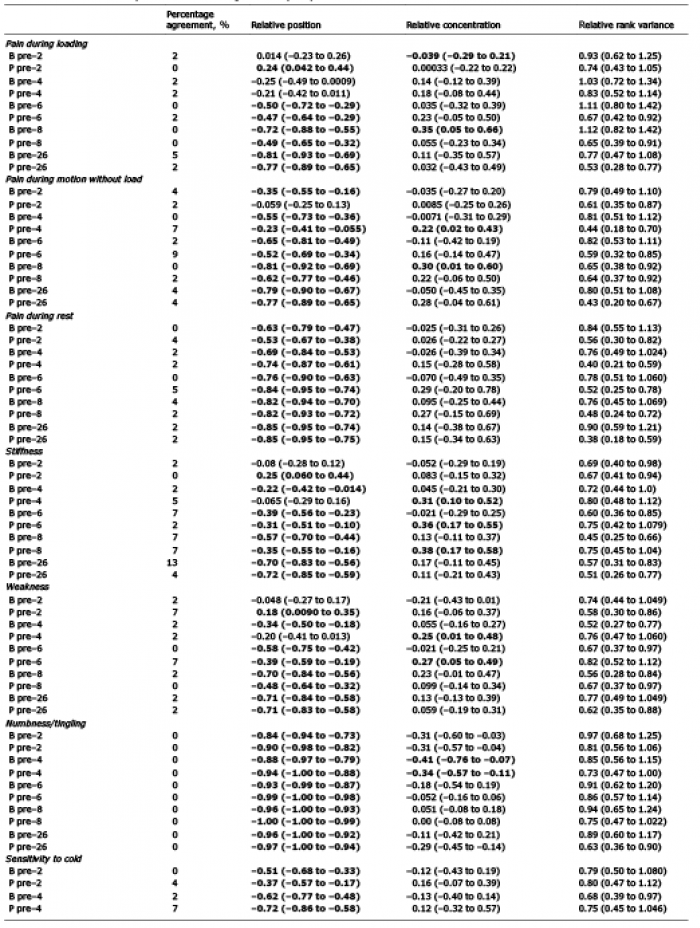 Click to show fullsize
Click to show fullsize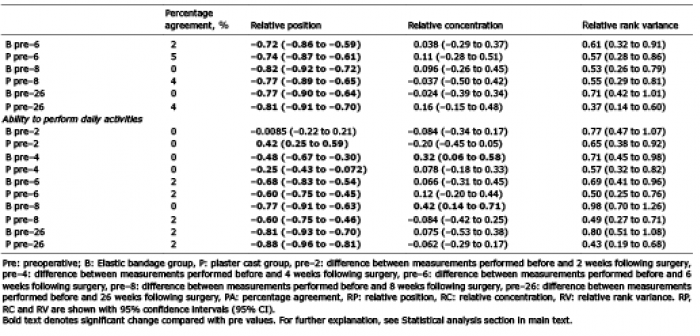 Click to show fullsize
Click to show fullsize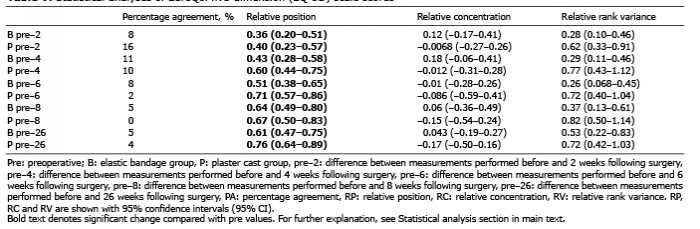 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize