
From the 1Lund University, Department of Health Sciences, Research Group Rehabilitation Medicine, 2Skåne University Hospital, Department of Neurosurgery, and Pain Rehabilitation, Lund, 3Department of Community Medicine and Rehabilitation, Rehabilitation Medicine, Umeå University, Umeå, 4Karolinska Institutet, Department of Clinical Sciences, Division of Rehabilitation Medicine, Danderyd Hospital and 5Department of Rehabilitation Medicine, Danderyd University Hospital, Stockholm, Sweden
Objective: To describe the organization, content and dosage of interdisciplinary pain rehabilitation, and the differences in degree of severity of problems of patients admitted to clinical units reporting to a Swedish national quality pain registry, grouped according to unit size and possible affiliation with a university hospital.
Methods: Reports from 31 out of 39 clinical units in Sweden, on inclusion processes, organization, content and dosage of interdisciplinary pain rehabil-itation, and patient-reported data from a Swedish national quality pain registry at assessment for interdisciplinary pain rehabilitation were analysed.
Results: the number of patients treated annually at each unit ranged from 3 to 340. In 17 units, teams comprised 5 professionals. Dosage of interdisciplinary pain rehabilitation ranged from 20–180 h per patient in total. Patients at the university-hospital units scored the highest levels of symptoms and lowest levels of health-related quality of life. Units used similar sets of inclusion criteria, and several treatments, such as education, self-training and psychological interventions, were used by most units.
Conclusion: When interpreting outcome data from registries, aspects other than rehabilitation outcomes must be considered. The interpretation of outcomes from quality registries would be facilitat-ed if data, in addition to assessments and patient-reported outcomes, also includes standardized descriptions of the reporting clinical units.
Key words: chronic pain; multimodal rehabilitation; pain registry; treatment dosage; treatment duration; inclusion criteria; team composition; rehabilitation organization.
Accepted Oct 21, 2020; Epub ahead of print Nov 6, 2020
J Rehabil Med 2020;52: jrm00128
Correspondence address: Marcelo Rivano Fischer, Skåne University Hospital, Lasarettsgatan 13, 221 85 Lund, Sweden. E-mail: marcelo.rivanofischer@skane.se
Doi: 10.2340/16501977-2765
The increasing interest in the contribution of quality reg-istries to clinical quality development demands satisfactory descriptions of input, i.e. clinical services delivered, for outcome comparisons. Interdisciplinary pain rehabilitation is a team-based coordinated intervention, with several professions delivering care for patients with chronic pain, which has shown better results than treatment by a single profession. There is a lack of knowledge about content and intensity of activities, and which professions are involved. This study shows that more than 50% of the clinical units in Sweden included the same 5 professions (physicians, physiotherapists, psychologists, social workers, and occupational therapists). Even though the units used similar inclusion criteria, and some treatments were alike, e.g. education, self-training and cognitive behavioural therapy, the number of patients treated and the length of treatment varied largely. Several admission criteria were used simultaneously, suggesting complex assessment processes. This study shows that when interpreting outcome data from registries, other aspects than those related only to rehabilitation interventions must be considered. We suggest that the interpretation of outcomes from quality registries would be facilitated if the data, in addition to assessments and patient-reported outcomes, also includes standardized descriptions of the reporting units.
There is increasing interest in the contribution of quality registers to clinical quality development (1, 2). Thus, it is important that input, i.e. clinical services delivered, is described clearly. Input description depends partly on the medical area targeted by the register. In rehabilitation medicine the concept “interdisciplinary pain rehabilitation” (IPR) is often used to describe services delivered to patients with chronic pain who are not benefiting from standard care (3).
Evidence favours IPR compared with less comprehensive treatments (4). Delivery of IPR usually includes cognitive behavioural therapy-based interventions (CBT), exercise therapy and education on pain and coping skills (5). IPR is a team-based coordinated intervention with a biopsychosocial approach to chronic pain (6). Patients are encouraged to participate and actively direct their plan and goals (7), making the approach both interdisciplinary (8) and patient-centred. In a systematic review of 27 studies (4), significant variations regarding settings, patient groups and interventions were described. All reviewed studies provided CBT, while exercise therapy was used in 63%, patient education in 60%, vocational or occupational therapy in 37%, and progressive relax-ation in 30% of studies. Biofeedback, ergonomic training, and nutrition counselling were used less frequently (4). Studies evaluating IPR have also included performing activities of daily living (ADL), group discussions (9, 10) and workplace interventions (11).
Detailed descriptions on the content and dosage (duration and intensity) of the interventions and degree of severity of the participants’ chronic pain conditions are usually lacking (4). In a recent study (7), patients and professionals from different centres in the Netherlands were interviewed regarding dosage and satisfaction with dosage received in IPR. Patients were satisfied with dosage and results, although dosage varied across the centres. Patients and staff agreed regarding the importance of individual levels of dosage of treatment. Nevertheless, these considerations led to different intensities of treatment across the centres. According to personnel, the dosage mainly depended on traditions and the available clinical expertise (7).
Most pain rehabilitation units in Sweden report data on patients receiving IPR to a national quality registry (12). Significant variations in patients’ characteristics have been mentioned in an earlier study based on this registry (12). Information on which interventions are included, their intensity and which professions are delivering services in clinical practice is meagre. No conclusions about the role of these factors can be drawn from existing reviews, due to shortcomings in inclusion criteria, small populations, heterogeneous settings and different instruments used in the selected studies (13).
Furthermore, studies investigating these factors in real-life settings serving clinical populations are scarce. Valuable knowledge can be acquired by studying input to registers; in particular, the concept of IPR and its variability regarding patient selection and clinical performance, to increase the usefulness of output data for clinical improvements.
Aims
The aims of this study were to describe: (i) the organization, content and dosage (duration and intensity) of interdisciplinary pain rehabilitation in Sweden, and (ii) differences in the degree of severity of problems of patients admitted to clinical units reporting to a national quality pain registry, grouped according to unit size and possible affiliation with a university hospital.
Swedish national quality registry for pain rehabilitation
A national quality registry for pain rehabilitation was launched in Sweden in 1998 (the Swedish Quality Registry for Pain Rehabilitation; SQRP). In 2014, 39 units in Sweden registered data on 6,022 patients in 2 categories: (i) patients who were only assessed by pain rehabilitation teams (professionals with pain medicine expertise and pain-related expertise in psychological, physical and social areas), by means of individual professional assessments, followed by discussion of findings and discussion of recommendations (other than IPR) with the patient; and (ii) patients who after assessment and discussions were recommended IPR (12). Information in the registry is, to a large extent, based on patient-reported outcome measures (PROM) on functioning, disability and health, with a focus on chronic pain. Clinical questions on pain, diagnoses and other clinical factors are assessed and answered by health profession-als. A primary aim of the registry is to facilitate comparisons of units offering IPR (national data), international comparisons and enable audits of single units, and to promote research on outcome studies. General inclusion criteria for participating in IPR are: (i) disabling chronic pain (on sick leave or experiencing major interference in daily life due to chronic pain); (ii) age 18 years and above; (iii) no further medical investigation needed; and (iv) written consent to participate and attend IPR. General exclusion criteria are: severe psychiatric morbidity; abuse of alcohol and/or drugs; and state of acute crisis.
The SQRP is a unique national database for patients with severe problems resulting from non-cancer chronic pain, managed by a board of rehabilitation professions only, with 90% of the rehabilitation units in Sweden reporting data, as described in detail elsewhere (12).
Procedure and analysis
This study analysed 2 sets of data:
Data from a questionnaire sent to all units about inclusion processes, IPR organization, content and dosage (duration and intensity) of their IPR programmes (n = 31 units).
Data from the registry collected at the initial assessment of the patients participating in the rehabilitation during the same time-frame (2014) as the questionnaires, in order to assess the degree of severity of the patients’ problems (n = 31 units).
Data from the questionnaire. A questionnaire that included 15 variables was developed by the board of the registry in collaboration with the clinical units reporting data (Appendix 1) and was sent to all units included in the registry in 2014. The questionnaire was sent to 39 units, of which 31 answered in a satisfactory manner (response rate 79%).
Nine variables were used in this study:
admission criteria for inclusion for IPR (1 variable with 9 possible choices);
number of patients receiving services (1 variable);
time spent in IPR (3 variables);
professions delivering services (1 variable with 11 possible choices);
interventions in IPR (1 variable with 11 possible choices);
follow-up of IPR (1 variable with 7 possible choices);
dosage of IPR at each unit (described as a composite of the total number of days in rehabilitation, number of days per week, hours per day, hours per week, total number of hours in rehabilitation, and professions involved, in accordance with the recommendations of Waterschoot et al. (13).
Data from the registry. The 39 units that participated in the national registry in 2014 differed in number of registered patients and in occurrence of affiliation with research centres. To analyse whether the number of patients registered at a unit or a unit’s affiliation to a university, were associated with the degree of severity of problems reported to the registry at baseline, the units were grouped as follows: “small”: 21–50 registered patients; “medium”: 51–100 registered patients; “large”: > 100 registered patients; and “university hospital units”. Six units registered 20 or fewer patients in 2014 and were excluded from the analyses. Furthermore, 2 units were excluded due to a high percentage of missing data (30–65%), leaving 31 out of the original 39 units fit for analysis. Ten units were included in the “small” category, 10 in the “medium” category, 5 in the “large” category and 6 in the “university hospital units” category. The number of patients receiving IPR registered in the database in 2014 was 3,511.
University hospitals are under regional jurisdiction in Sweden. These hospitals attend severe cases and complications besides delivery of standard care for patients within their geographical reach. They collaborate with medical faculties at the universities and have agreements with the universities regarding scientific clinical research and education. In a region, clinical rehabilitation units of different size can operate simultaneously. Pain rehabilitation often begins in primary care and, when not successful, patients can be referred to clinical units that work mainly with patients with chronic pain problems.
Eleven variables from the registry were selected from the database to describe the degree of severity of problems present-ed by patients at first contact with a unit. The selection of the variables was based on clinical professional consensus and the IMMPACT recommendations for trials (14, 15). A recent study by Zidarov et al. (16) aimed at finding the key areas to measure in chronic pain clinical settings and focused on clinicians’ choices, patient preferences and current guidelines. They propose a list of variables in accordance with those chosen in the current study.
The variables selected here were: “Pain last week” (Numeric Pain Rating Scale (NPRS) (17); Number of pain locations (18); “Life interference” (Multidimensional Pain Inventory) (19); “Difficult/very difficult to return to work”; “Experienced health (EQ-5D, Thermometer and EQ5D index) (20); “Native country is Sweden”; “Degree of depression” and “Degree of anxiety” (Hospital Anxiety and Depression Scale; HADS) (21); “ Physical function” (PF); and “Vitality” (VT) (Short Form; SF-36) (22).
Statistical analysis
Descriptive analyses were used for describing the units’ IPR based on the information received from the units that answered the questionnaire (n = 31) and for the degree of severity of the problems presented by patients at first contact according to data from the national registry in 2014 (n = 31). Differences between categories of units (based on volume and research affiliation) were analysed using the independent samples Kruskal–Wallis test. Effect sizes were calculated for the differences in degree of severity of problems between categories of units, and Cohen’s d are presented. The absolute Cohen’s d was insignificant for <0.20, small for 0.20–0.49, moderate for 0.50–0.79, large for 0.80–1.29, and very large for ≥1.3 according to Cohen (23). The Mann–Whitney U test was used for further post-hoc analyses of differences between university hospital units and the other categories of units. For statistical significance a level of p≤0.05 was chosen.
Ethical considerations
For data collection in the national registry, the ethical princi-ples of the World Medical Association Declaration of Helsinki were adopted. Informed consent is always granted, and participation is voluntary. The data are collected as part of the ongoing quality control of clinical care activities in the participating departments and the data are stored with the consent of the Swedish Data Inspectorate (permission number 1580-97).
World Medical Association Declaration of Helsinki. (24) Ethical principles for medical research involving human subjects.
Data from the questionnaire
Thirty-one out of 39 units answered the questionnaire (response rate 79%).
Admission criteria for IPR. All clinical units included “personal factors” as admission criteria; 30 units reported screening for “relevant symptoms” and making decisions based on a “medical rehabilitation assessment”; 29 units included “age”; and 28 units used “physical function and activity level” as admission criterion. “Language proficiency” was included by 26 units; “return to work or continue working” by 24 units; “organizational factors” by 22 units; and 11 units (28%) used all 9 criteria-items as admission criteria.
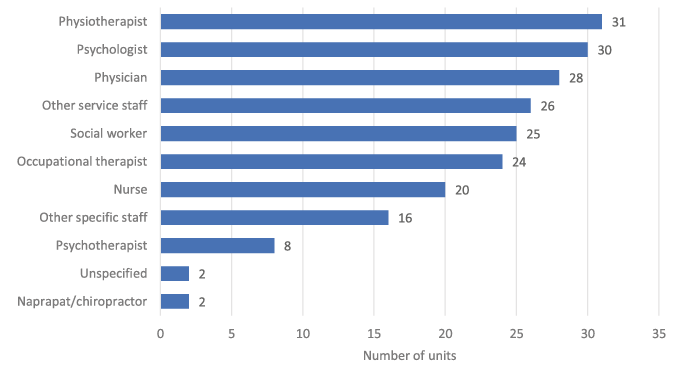
Professions delivering services. Most units reported that the members of the rehabilitation team included physio-therapists (n = 31), psychologists (n = 30) and physicians (n = 28), trained social workers (n = 25) and occupational therapists (n = 24). In 17 out of 31 units, IPR was delivered by teams of physicians, physiotherapists, psychologists, social workers and occupational therapists (Fig. 1).
Fig. 1. Number of clinical units reporting the indicated profession in their rehabilitation teams. “Other specific staff” includes, e.g. work counsellor, diet counsellor and sports leader. “Other service staff” includes secretary, receptionist and kitchen staff.
Interventions in IPR. There were 11 possible choices to describe the type of interventions used. All 31 units reported using interventions included in “dialogue and education” (e.g. education, training in wellness and healthy living habits, meetings with families, video feedback, couples’ therapy) and “self-training” (e.g. home lessons, activity diary, physical self-training, reflection time and self-analysis). Twenty-nine units reported using methods of “activity training” (activ-ity training, graded activity training and exposure training), “meetings” (conferences with patients, rehabilitation team, vocational guidance, rehabilitation coordinator, goal-setting meetings and meetings to check on goal achievement) and “cognitive behaviour-al therapy” (CBT). Twenty-seven units reported using “other psychological treatment” (e.g. supervised group therapy, pain or stress coping course, psychological and social aspects, post-traumatic stress disorder (PTSD) treatment, psychodynamic methods) and “acceptance and commitment therapy” (ACT) (e.g. goal compass, training in ACT principles, mindfulness). Twenty-six units reported using “relaxation” techniques, 24 units different methods of “physical training” and 18 units reported “specific treatments” (e.g. techniques used by chiropractor/naprapath, transcutaneous electric nerve stimulation, problem-based learning, orthoses, tactile massage, medicines, nerve blocks, etc.). Only 14 units reported using interventional “measures in the workplace”. All units reported having follow-ups (one-year follow-up by post or at the unit for filling in the registry’s questionnaires). Usually, an extra follow-up meeting was scheduled 2–3 months after discharge from rehabilitation (21 out of 31 units).
Dosage and intensity of IPR. Thirty-one units answered the 3 questions about dosage. There was a large variation in the number of days in rehabilitation (7–46 whole days), number of days per week (1–5 days per week) and number of hours per day (1–7 h per day). The number of hours per week varied from 1 to 30 h and the total number of hours in rehabilitation varied from 20 to 180 h. Applying proposed intensity cate-gories (24) to our study, 17 units provided a high-intensity IPR with more than 100 h of rehabilitation, 12 units provided IPR on a mid-intensity level of 30–99 h, and 2 units provided IPR on a low-intensity level of less than 30 h. Five out of 6 university-hospital units delivered high-intensity IPR to each patient. All but 2 units serving more than 100 patients a year delivered high intensity IPR. Six out of the 7 units that reported 20 or fewer patients per year to the registry delivered low-to-medium intensity IPR (Table I).
Interventions in IPR. There were 11 possible choices to describe the type of interventions used. All 31 units reported using interventions included in “dialogue and education” (e.g. education, training in wellness and healthy living habits, meetings with families, video feedback, couples’ therapy) and “self-training” (e.g. home lessons, activity diary, physical self-training, reflection time and self-analysis). Twenty-nine units reported using methods of “activity training” (activ-ity training, graded activity training and exposure training), “meetings” (conferences with patients, rehabilitation team, vocational guidance, rehabilitation coordinator, goal-setting meetings and meetings to check on goal achievement) and “cognitive behaviour-al therapy” (CBT). Twenty-seven units reported using “other psychological treatment” (e.g. supervised group therapy, pain or stress coping course, psychological and social aspects, post-traumatic stress disorder (PTSD) treatment, psychodynamic methods) and “acceptance and commitment therapy” (ACT) (e.g. goal compass, training in ACT principles, mindfulness). Twenty-six units reported using “relaxation” techniques, 24 units different methods of “physical training” and 18 units reported “specific treatments” (e.g. techniques used by chiropractor/naprapath, transcutaneous electric nerve stimulation, problem-based learning, orthoses, tactile massage, medicines, nerve blocks, etc.). Only 14 units reported using interventional “measures in the workplace”. All units reported having follow-ups (one-year follow-up by post or at the unit for filling in the registry’s questionnaires). Usually, an extra follow-up meeting was scheduled 2–3 months after discharge from rehabilitation (21 out of 31 units).
Dosage and intensity of IPR. Thirty-one units answered the 3 questions about dosage. There was a large variation in the number of days in rehabilitation (7–46 whole days), number of days per week (1–5 days per week) and number of hours per day (1–7 h per day). The number of hours per week varied from 1 to 30 h and the total number of hours in rehabilitation varied from 20 to 180 h. Applying proposed intensity cate-gories (24) to our study, 17 units provided a high-intensity IPR with more than 100 h of rehabilitation, 12 units provided IPR on a mid-intensity level of 30–99 h, and 2 units provided IPR on a low-intensity level of less than 30 h. Five out of 6 university-hospital units delivered high-intensity IPR to each patient. All but 2 units serving more than 100 patients a year delivered high intensity IPR. Six out of the 7 units that reported 20 or fewer patients per year to the registry delivered low-to-medium intensity IPR (Table I).
Table I. Dosage and intensity of interdisciplinary pain rehabilitation (IPR) programmes in the included units (n = 31). Intensity based on total number of hours in rehabilitation (low < 30 h; medium 30–100 h; high > 100 h)
Data from the registry
Degree of severity of patients’ characteristics in small, medium and large clinical units and in university-hospital units. The median and quartile values in the variable “average pain last week” were almost the same for all 31 included units that registered data at the time of the study. Thus, the variable was not included in further analyses of degree of severity of the patients’ problems.
Native country. Seventy-nine percent of the total number of patients registered in 2014 reported being born in Sweden. Among the unit categories there was a significant difference (p < 0.001) in the proportion of native Swedish patients that were admitted. The “medium” clinical units had the highest proportion of native Swedish patients (86%), the large clinical units had the lowest (74%). The university-hospital units had 80% Swedish native patients and the “small” clinical units had 84%. Compared with the university-hospital units, the “large” clinical units had significantly fewer native Swedish patients (p = 0.001), the “medium” clinical units had significantly more native Swedish patients (p = 0.001) and there was no difference compared with the “small” clinical units.
Description and differences in degree of severity of problems between categories of units. Regardless of category of unit, all patients had a high number of pain locations (Table II, The median value ranged from 11–14). Furthermore, the median values for both anxiety and depression in HADS were in the range 8–11, indicating a probable presence of a mood disorder. The units in the “university-hospital” category had the highest median values for HADS Anxiety and the lowest median values for the EQ5D index, Health status (EQ-5D, Thermometer), SF-36 Physical function and SF-36 Vitality (Table II).
Significant differences between categories of units were observed in “Number of pain locations” (p < 0.001), “HADS Anxiety” (p < 0.001), “HADS Depression” (p < 0.001), “MPI Life interference” (p < 0.001), “EQ5D index (health-related quality of life)” (p = 0.018), “EQ-5D, Thermometer (health status) (p < 0.001), and “SF-36 Vitality” (p < 0.001).
Table II. Pain intensity, Number of pain locations, Hospital Anxiety and Depression Scale (HADS) Anxiety and Depression, Multidimensional Pain Inventory (MPI) Life Interference, EuroQoL 5 Dimensions (EQ5D) Index, EuroQoL Visual Analogue Scale (EQ-5D, Thermometer), Short Form-36 (SF-36) Physical Function and Vitality by unit category
Differences in patient’s degree of severity of problems between university-hospital units and other units. In the variable SF-36 Vitality, the patients at the “university--hospital units” showed significantly lower vitality than the “small” (p = 0.019), “medium” (p < 0.001) and “large” units (p < 0.001) (Cohens’ d = 0.19) (Fig. 2). Significant lower values were also observed in the EQ5D index at the “university-hospital units” compared with the “medium” units (p = 0.004) (Cohens’ d = 0.33) and in EQ-5D, Thermometer (health status) compared with the “large” units (p < 0.001) (Cohens’ d = 18).
Fig. 2. A comparison with medians and percentiles between categories of clinical units in the variables EuroQoL Visual Analogue Scale (EQ-5D, Thermometer) (health status), Short Form-36 (SF-36) Vitality, and EuroQoL 5 Dimensions (EQ5D) Index.
In the variable HADS Anxiety, patients at the “university-hospital units” showed significantly higher anxiety than the “large” (p = 0.002) and “medium” (p < 0.001) units (Fig. 3) (Cohens’ d = 0.25). Also, in HADS Depression, patients at the “university-hospital units” showed significantly higher degree of depression than both the “large” (p < 0.001) and “medium” units (p = 0.001) (Cohens’ d = 0.16). Significantly higher scores were reported on the MPI life interference subscale at the “university-hospital units” compared with the “large” (p < 0.001) and “medium” units (p = 0.006) (Cohens’ d = 0.29). The number of pain locations was significantly higher in the “university-hospital units” than in the “large” units (p < 0.001) (Cohens’ d = 0.09).
Fig. 3. A comparison of medians and percentiles between categories of clinical units in the variables HADS Anxiety, HADS Depression, number of pain locations, and MPI Life Interference (measuring the degree to which pain interferes with life).
This study found large variations in the size of pain rehabilitation units in Sweden, the number of patients treated per year, and the “mix” of professions in the rehabilitation teams, indicating probable variations in clinical experience and ways of delivering services. Fifty percent of the units used the “standard” mix of IPR staff, which reflects the biopsychosocial framework of pain rehabilitation: physician, physiotherapist, occupational therapist, social worker, and psychologist. The results (Table II) show that university-hospital units admit patients with slightly more severe degree of problems than other units, for example in SF-36 vitality and physical function and EQ-5D health-related quality of life and health status. The effect sizes found are small; however, the trend that the university-hospital units are handling more severe patients is probably clinically relevant. Further studies including subgroups of patients are suggested. There are similarities be-tween the pain rehabilitation units. Similar sets of criteria were used when selecting patients for admission to IPR. The categories of interventions used by almost all units were education, self-training, activity training, CBT and meetings. However, despite a growing body of evidence regarding its importance, less than half of the units reported interventions in the workplace.
Admission criteria may influence outcomes. In the current study, admission of patients to IPR was guided by many criteria, grouped into 9 major areas. All pain rehabilitation units used personal factors (e.g. potential for change, motivation, relevant goals) as admission criteria and most units also reported relevant symptoms, medical rehabilitation assessment, age, physical function and activity level. Skjutar et al. (25) used a multidisciplinary expert panel to explore indicators for IPR. The panel identified 20 indicators, indicating that assessments for IPR are complex. The indicators were well aligned with the findings of the current study on admission criteria, including patient issues, such as activity problems, catastrophizing, fear avoidance, motivation, psychosocial problems and reduced physical function; and other issues, such as sick leave, current situation in primary healthcare, work situation, and tacit knowledge of personnel. We cannot conclude which of the reported criteria are most critical for admission. Nevertheless, the high number of reported criteria might indicate variability in their use, due to factors that are difficult to measure, such as background of staff making decisions, changing priority of criteria, demands from stakeholders, etc.
Team composition has been identified as another factor that could influence interventions and therefore outcomes. In many studies teams are defined as consisting of 2 or more collaborating professionals, as stated in a Cochrane review (26). A study by Salathé et al. (27), specifies that a team for treating low back pain should include at least a medical doctor and a clinical psychologist or a physiotherapist. The teams delivering IPR reported in the current study were much more comprehensive; no unit had fewer than 4 professionals per team. Most units reported 5–7 professionals in their team. The current results on team composition are in accordance with a review of 4 large centres in the USA (28). This indicates that the requirements for team composition in pain rehabilitation may differ. In published studies, IPR is usually defined as a complex intervention based on a biopsychosocial framework (29), suggesting that medical, physical, social and psychological aspects should be considered. The team composition reported here reflects the biopsychosocial framework necessary for IPR.
Interventions such as education, self-training, activity training, CBT and meetings were reported by almost all units. A range of psychological interventions was delivered, units reported using CBT, ACT and other psychological treatments. In this context we emphasize that the patient’s assessment by and contact with the different professionals of the team assures that preferences and needs of the individual patient can be given priority, irrespective of the character of the intervention. Individual needs can be managed even if the patient receives rehabilitation together with other patients. It was sometimes complicated to interpret information about activity training, since training was delivered by either physical and/or occupational therapists. Studies show that the focus of activity training in physical therapy is often on increasing muscle strength, range of motion of joints, musculoskeletal functional impairments, and instructing patients in developing their own home exercise programmes (9, 28). Activity training in occupational therapy focuses on identifying functional deficits, improving body mechanics, ergonomics, activity tolerance, as well as pacing in meaningful everyday activities (9, 28). In the current study most units included physical activation in some way. A study about the components of IPR concluded that a key to successful outcomes was the degree of shared attributes of the team members. This helped patients to unlearn maladaptive behaviours, foster optimism, combat demoralization, and promote a self-management approach (28). It might be argued that the kind of professional expertise in the teams and the type of interventions delivered interact in complex ways influenced by characteristics of the team members. Typically, specific interventions aiming directly at pain reduction are not included in IPR described in the research literature (4, 9, 10, 11). Nevertheless, more than half of the units in the current study used some pain-reducing intervention, suggesting that the content of IPR in clinical practice, to some extent, differs from that delivered in clinical trials. The rationale for excluding pain-reducing interventions is that IPR aims to return the subject to normal life in spite of pain, not a repetition of previous failed attempts at pain reduction by means of specific interventions. The current results show that, to some extent, different approaches are mixed in clinical practice, perhaps altering the expected results of IPR. Since a recent study based on data from the SQRP has shown medium-effect sizes for pain intensity variables after IPR (30) further research on this is necessary.
Only 14 of 31 units reported interventions focused on the workplace, in spite of consistent research indicating that these interventions are crucial for successful outcomes (29, 31, 32). In a previous study of return to work (RTW) 1 and 2 years after IPR, positive changes in sick-leave patterns were reported after IPR (32, 33). Improvements in RTW may be bolstered if more of IPR, as a standard, includes workplace interventions when relevant.
According to the current results, units delivering IPR differed in both content of interventions and staffing of professionals in the teams. IPR is defined as a framework that contains “a synchronized combination of physical, educational, or psychological treatments in combination with measures for returning to work/studies” (34), suggesting that interventions are cohesive and homogeneous, with experts in many areas, raising questions about the assumptions behind many studies on IPR, namely, that interventions and staffing are similar.
Considerable variation was reported in the variables used in this study to describe dosage (Table I), which illustrates that patients are subject to different degrees of intensity and duration of interventions. Similar results are presented in other studies (7). In a recent study of dosage no difference in improvement was found between more and less extended pain rehabilitation. The authors conclude that the optimum dosage of IPR is unknown and scarcely studied (35). There are no conclusive results in the literature regarding the relationship between dosage and outcome and studies that analyse rehabilitation’s outcome in relation to different levels of dosage are scarce and often of low quality (4). Regarding intensity categories, according to Kamper et al. (26) the current study found that 17 units provided a high-intensity IPR with more than 100 h rehabilitation, 12 units provided IPR on a mid-intensity level of 30–99 h and 2 units provided IPR on a low-intensity level of less than 30 h. In the USA, IPR has been described by accessing information in 4 well-established units, within large hospitals, centres of excellence or large health organizations. In these settings IPR usually lasts 3–6 weeks, 6–8 h per day (28), following Guzman et al. recommendations (36).
The current study found variations in “degree of severity of problems of patients admitted” to the pain rehabilitation units. Reported “health and functioning at admission” are thought to influence outcomes (14, 16). The current findings indicate that patients admitted to units affiliated to university hospitals presented a higher degree of severity of problems at admission than patients in other units. There are many potential explanations for this finding, ranging from staff competency, to knowledge about referral pathways. This could relate to the usual role of university hospitals in accepting patients with the most severe conditions. University hospital units also reported higher dosage, perhaps indicating that the complex needs of the patients admitted to these units required a larger investment, reflected in the duration and intensity of IPR.
The outcomes of pain rehabilitation are currently a pressing issue, both at the individual and at societal level. This study paves the way for a research arena that focuses on areas largely ignored, or just briefly mentioned, by previous research, i.e. content and dosage of IPR, inclusion criteria and degree of severity of the problems affecting people in need of pain rehabilitation, within a biopsychosocial framework. Comparisons of research on IPR without information on these issues might be misleading. Furthermore, this study describes differences in aspects of IPR that should be considered whenever attempts are made to evaluate pain rehabilitation.
Study limitations and advantages
Studies based on national quality registries are influenced by the representability of the regularly reporting units. In the current study, 90% of all units reported data; a satisfactory proportion, with 3,511 patients registered during the study year. Nevertheless, there were missing data. For example, in order to analyse the issue of “degree of severity of patients’ problems”, 2 units were excluded due to a large amount of missing data. However, the percentages of missing values for each instrument in the registry were low, ranging from 0% to 9% (Table II).
The questionnaire’s response rate (31/39; 79%) was satisfactory. The units were geographically spread, situated in both major and minor cities, differing in size and type of organization, ensuring that the sample reflected the delivery of IPR at a national level.
This study shows that, when interpreting outcome data from registries, aspects other than those related to rehabilitation interventions only must be considered. We suggest that the interpretation of outcomes from quality registries would be facilitated if the data, in addition to assessments and patient-reported outcomes, also include standardized descriptions of the reporting units. The degree of problems presented by patients attending university-hospital units may differ from that presented by patients attending other units.
Appendix 1. Construction of the questionnaire.


 Click to show fullsize
Click to show fullsize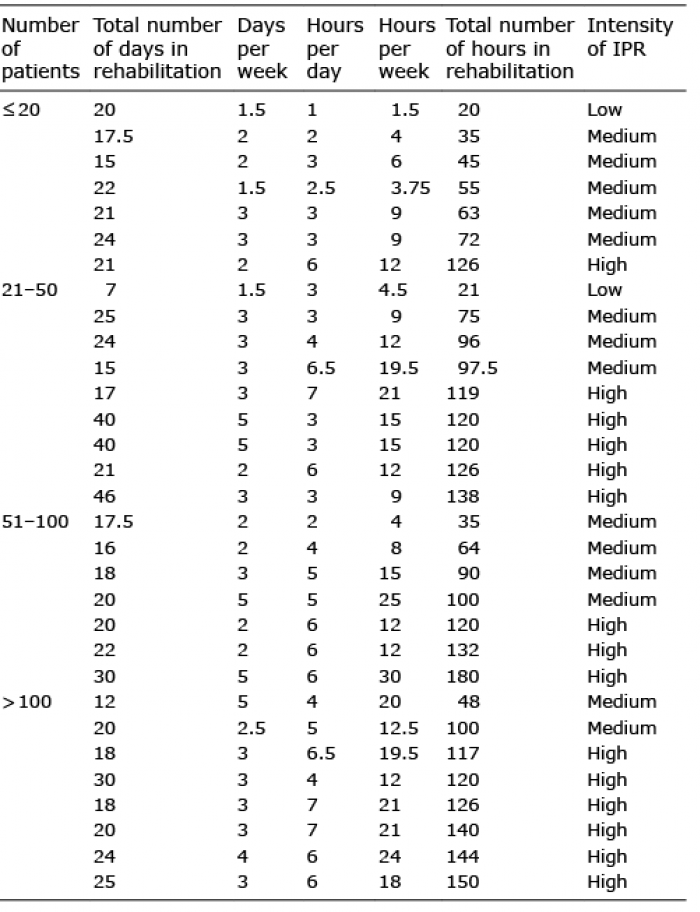 Click to show fullsize
Click to show fullsize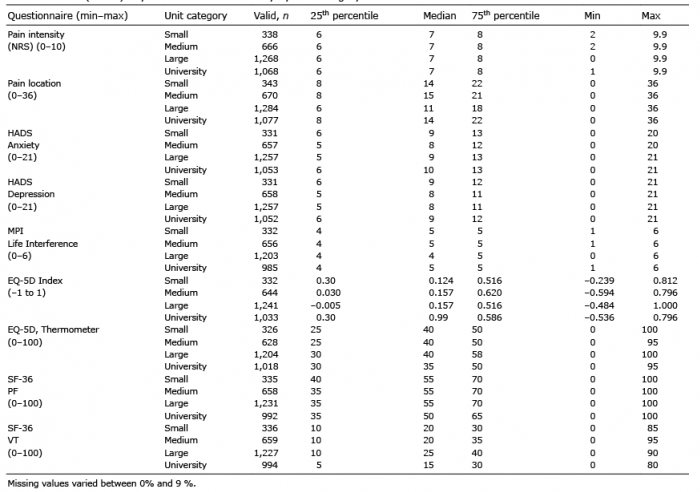 Click to show fullsize
Click to show fullsize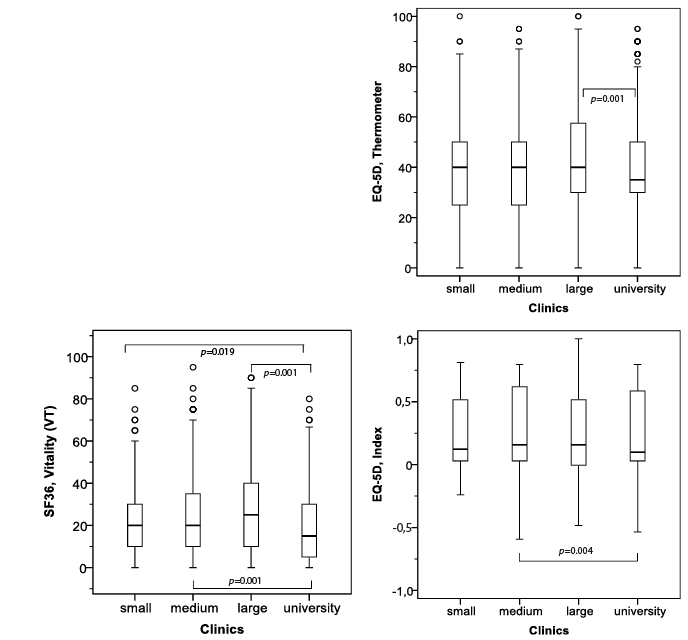 Click to show fullsize
Click to show fullsize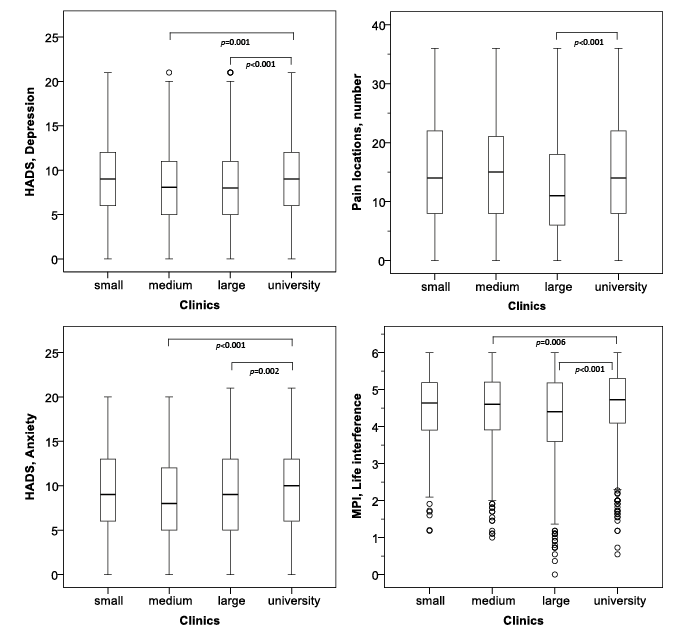 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize