
From the 1Department of Medicine, University of British Columbia, 2GF Strong Rehabilitation Centre, Vancouver, 3Hodgson Orthopedic Group, Coquitlam, BC, 4Vancouver Island Health Authority, 5Rehabilitation Research Program, Vancouver Coastal Health Research Institute, 6International Collaboration on Repair Discoveries (ICORD), Vancouver, 7Canadian Advances in Neuro-Orthopedics for Spasticity Congress, Study Location, New Westminster Rehabilitation Medicine 304-250 Keary St, New Westminster, BC, Canada
Objective: To investigate changes in hemiparetic gait parameters after treatment of elbow flexor spasticity with botulinum neurotoxin (BoNT) injection and adjunctive casting.
Design: Prospective case series.
Subjects: Ten participants with spasticity secondary to acquired brain injury (8 stroke, 2 traumatic brain injury).
Interventions: Participants received BoNT injections for their spastic elbow flexors under ultrasound guid-ance. Two weeks post-injection, an elbow stretching cast was applied for 1 week.
Outcome measures: Assessments using the Modified Ashworth Scale (MAS), Tardieu scale V1 angle of arrest at slow speed and V3 angle of catch at fast speed, 2-min walk test (2MWT), Edinburgh Gait Score scale (EGS) and video gait analysis for step-length symmetry were conducted pre-BoNT injection (t0) and at cast removal (t1). Goal attainment scale (GAS) was used to assess changes in spasticity and gait 3 months post-injection (t2).
Results: At t1, participants showed a mean increase of 16.7° (p < 0.01) on the Tardieu Scale V3 and a mean reduction of 0.5 points on the MAS (p < 0.05). There was also a mean reduction on EGS of 2.7 points (p < 0.05), and a mean increase on 2MWT of 3.1 m (p < 0.05). On the GAS, all participants report-ed improved gait at t2 and 80% reported a decrease in spasticity.
Conclusion: Combining BoNT injection with casting for treatment of elbow flexor spasticity without treat-ing the lower limb may improve hemiparetic gait parameters.
Key words: botulinum; spasticity; casting; gait.
Accepted Sep 3, 2020; Epub ahead of print Sep 17, 2020
J Rehabil Med 2020; 52: jrm00110
Correspondence address: Rajiv Reebye, GF Strong Rehabilitation Centre, 4255 Laurel St, Vancouver, BC, V5Z 2G9, Canada. E-mail address: Rajiv.Reebye@vch.ca
Doi: 10.2340/16501977-2743
Brain injury from stroke or trauma can cause spasticity, a disorder characterized by intermittent or sustained involuntary muscle activation. Spasticity contributes to gait abnormalities that may increase the risk of falls and, consequently, affect quality of life. Botulinum toxin injections are a widely accepted treatment for spasticity. Studies have suggested that applying a stretching cast after botulinum toxin injections may improve functional outcomes. This study investigated changes in gait after botulinum toxin injections and a stretching cast in a sample of 10 patients with spasticity secondary to brain injury. The results show that a combination therapy of botulinum toxin injection and casting may improve gait without treatment of the lower limbs in long-term sur-vivors of brain injury.
Acquired brain injury (ABI) secondary to stroke or trauma is a leading cause of adult disability worldwide (1, 2). Spasticity, a sensorimotor disorder characterized by intermittent or sustained involuntary muscle activation, is a common consequence of ABI. Over time, spasticity may lead to the development of contractures, which can have a devastating impact on function (3, 4). Spasticity is associated with adverse health outcomes and reduction in quality of life (2, 5).
Gait is a complex sequence of coordinated movements involving both the upper and lower extremities. Symmetrical arm swing during gait is important for creating a normal reciprocal gait pattern. This maintains the body’s equilibrium, contributing to balance and thereby increasing the efficiency of gait (6). Patients with ABI may experience associated reactions during gait, thereby triggering abnormal muscle activation in the upper extremities (7). A common pattern is that of excessive elbow flexion. These anomalies may ad-versely affect gait and increase risk of falls. Thus, managing upper limb spasticity may improve gait (2, 8).
Botulinum toxin (BoNT) is widely accepted as a safe and effective pharmacological treatment for spasticity (9). BoNT is a neurotoxin that inhibits the release of acetylcholine into the neuromuscular junction, thereby decreasing the involuntary muscle activation seen in spasticity (9). The effects of BoNT typically last up to 3 months (9). A large observational study found that BoNT A has a clinically significant effect on elbow flexor
spasticity (10). Furthermore, a prospective study and a recent systematic review support that BoNT injection of the spastic upper limb muscles improves gait (6, 11).
There is evidence for the use of adjunctive treatments following BoNT injection to improve outcomes of limb spasticity (12). Furthermore, a multimodal programme for contracture management in patients with ABI, including BoNT, casting and motor training, has been found to be useful in improving joint range of motion (13). A recent systematic review also concluded that adjunct casting may improve outcomes following BoNT injection (14). However, to date, the majority of research into casting has focused on the lower extrem-ities (14). We therefore sought to explore a multimodal approach to the treatment of arm spasticity as a means to improve gait, without treating the lower extremity.
The primary objective of this prospective study was to investigate the changes in gait parameters in patients with ABI after treatment of their elbow flexor spasticity with BoNT injection and subsequent casting. The sec-ondary objectives were to assess adverse events, effect on spasticity and the patient’s personalized goal attainment with regards to gait and use of the affected arm.
Participant selection
All participants were outpatients receiving therapy for their spasticity at a community-based spasticity clinic. Participants were screened for suitability for BoNT injections and casting, with patient history, physical examination, and goal setting using GAS. Contraindications, risks and benefits were reviewed, and informed consent was obtained for all patients. Creation of management protocols and BoNT injections were performed by a physical medicine and rehabilitation specialist (physiatrist) with 15 years of experience in spasticity management.
For the purpose of this prospective study, a convenience sample was obtained from patients presenting to clinic who were deemed suitable for the study by the clinic physiatrist.
Inclusion criteria were age > 18 years; hemiparetic spasticity following ABI; and elbow flexor spasticity with Modified Ashworth Scale (MAS) 1–3. Potential participants had to be independent ambulators with or without assistive devices and have a minimum 10° discrepancy between the angle of maximum passive range of motion at slow speed (Tardieu V1) and the angle of catch or clonus at fast speed (Tardieu V3). Patients who had previously received BoNT were not excluded as long as the last injections were administered more than 3 months previously. Patients were excluded if they had an open or erod-ed skin surface, significant oedema, a history of non-union fracture or recent fracture, known osteoporosis, painful arthritis, impaired circulation at the extremity to be casted, recent deep venous thrombosis, or poor home support.
Informed verbal consent was obtained before the com-mencement of the study. The study was approved by the Clinical Research Ethics Board of the University of British Columbia (UBC CREB reference number H20-00195).
BoNT injections
The physiatrist, who had more than 10 years of experience in ultrasound-guided muscle localization, performed all the injections using an ultrasound-guided (Esaote ultrasound machine with 13 Hz transducer, Esaote Canada; location: Fishers, Indiana, USA) and a non-touch clean technique. BoNT injection (Incobotulinum toxin type-A, Xeomin™, Merz Pharma Canada; location: Burlington, Ontario, Canada) were injected to the brachialis (range 50–100 IU, mean 78 IU (standard deviation (SD 22)) and brachioradialis (range 30–100 IU, mean 73 IU (SD 27) muscles for all the participants. Biceps brachii, flexor carpi radialis (FCR), flexor carpi ulnaris (FCU) and flexor digitorum superficialis (FDS) muscles were injected in some other participants if deemed indicated. The mean total dosage was 190.5 IU (SD 52.3) and total maximum dosage was 300 IU in a 2:1 dilution with preservative-free normal saline.
Casting protocol
Two weeks post-injection, participants received a single elbow cast application for a mean of 7 days (range 3–9 days). All participants were casted at the clinic by an orthotist who had more than 5 years casting experience. The casting technique required 1.5 h for application and 1 h for removal. Determination of casting angle was personalized, based on measurement of the elbow angle of motion in standing at slow speed (Tardieu V1) and fast speed (Tardieu V3) using a digital goniometer prior to casting. Cast was applied at participant’s submaximal tolerable stretch, which was approximately 70% of the difference between the V3 and V1 angles with the participant seated, to provide low load stretch to reduce spasticity (15, 16). Participants were consulted to ensure the position was tolerable. All casts were lined with cotton stockinette. Shear reduction layer (Sof-Roll™, BSN Medical; location: Laval, Quebec, Canada) was applied on top, with integrated silicone padding for high-pressure areas. Foam-based (Cellona, Lohmann & Rauscher; location: Milwaukee, Wisconsin, USA) padding was utilized to decrease risk of pressure sores. At the cast application appointments, participants were provided with a standardized information handout to take home on casting day for monitoring potential adverse events. No interventions were provided to the lower limbs.
Outcome measures
Outcome measures of gait assessment included the 2-min walk test (2MWT), Edinburgh Gait Score (EGS) and step-length symmetry. All instructions were standardized, and the same script was followed at both time-points for all participants. The 2MWT was conducted on a 3-m walkway. Parallel bars were available on each side of the walkway as a safety precaution and were not used as gait aids. The EGS is a video assessment of gait quality in people with upper motor neuron diseases, and consists of 17 parameters scored from 0 to 2 points for each lower limb, evaluating gait in frontal, sagittal and transverse planes. The maximal gait alteration is 34 points, and 0 points indicates an absence of pathology (17). Minimum clinically important difference (MCID) of EGS was set as a reduction of 2.4 points (18). Gait was recorded on video before casting and at cast removal. Gait was analysed using the Prosthetic and Orthotics (PnO) Data Solutions to determine EGS and step-length symmetry. Outcome measures were assessed by the same orthotist pre-injection (t0) and following cast removal (approximately 3 weeks post-injection; t1).
In addition to records for adverse events, outcome measures collected at t0 and t1 included the MAS, elbow resting angle when participant is standing (Tardieu V0), elbow angle of arrest at slow speed (Tardieu V1), elbow angle of catch at fast speed (Tardieu V3). The MCID for MAS score is 1-point (19).
Goal Attainment Scaling (GAS) was used to identify person-alized goals with regards to gait post-intervention (20). Goals were set by the participant with the help of the physiatrist at t0 and were assessed by the same physiatrist approximately 3 months post-injection and casting (t2).
Statistical analyses
Changes in outcome measures between t0 and t1 were determined using a paired t-test for normally distributed data. Wilcoxon matched-pairs signed-rank test was used to assess significance for non-normally distributed data. Normality was determined using the Shapiro-Wilk test. A simple regression model was used to assess the effect of the individual participant characteristics on outcome measures. Unless otherwise specified, results are expressed as means and SDs.
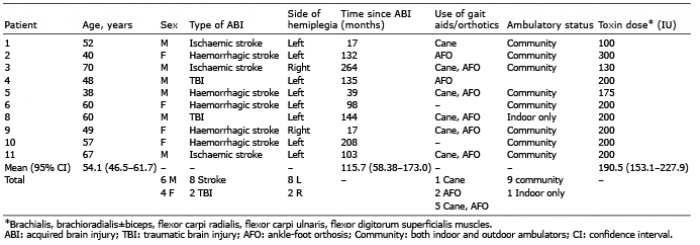
Participant characteristics are summarized in Table I. Participants who used a cane or ankle-foot orthosis (AFO) were assessed while using their gait aids at both t0 and t1.
Table I. Participant characteristics
Elbow flexor spasticity
A statistically significant reduction in MAS score (–0.5±0.41, p = 0.016) was observed at cast removal (t1), with 70% of participants showing improvements (Table II and Fig. 1A). However, only 30% of participants reached the MCID of 1-point reduction in MAS. At t1, all participants showed an increase in angle of catch at V3 on Tardieu and the mean change was +16.7±11.6° (p = 0.001) (Table II and Fig. 1B). There were no significant improvements in the mean Tardieu V0 and V1 angles (Table II).
Table II. Outcome measures at pre-injection and casting (t0), and at cast removal (t1).
Functional gait parameters
Statistically and clinically significant improvement was seen in EGS (–2.7±3.68, p = 0.046) at t1 (Table II). Common improvement categories in EGS were foot rotation, initial contact, and maximum ankle dorsiflexion during ambulation. Seventy percent of participants had a reduction in their EGS, with 40% showing clinically significant improvement (Table II and Fig. 1C). The results of the 2MWT were significantly improved at t1 (+3.1m±4.2, p = 0.045) with 70% of the participants showing improvements (Table II and Fig. 1D). No significant change was observed in step-length symmetry (Table II).
Fig. 1. Improvement in (A) Modified Ashworth Scale (MAS), (B) Tardieu V3, (C) Edinburgh Gait Score scale (EGS) and (D) 2-min walk test (2MWT) in individual participants between pre-injection and casting (t0) and at cast removal (t1). Dashed line indicates threshold for minimum clinically important difference.
Goal Attainment Scale (GAS)
Gait improvement was a goal identified by all participants, and at approximately 3 months post-intervention 30% rated gait improvements as expected (GAS = 0) and 70% beyond expectation (GAS = +1 or +2). Of all the goals related to the affected upper limb, 30% of participants reported reaching the anticipated level of achievement on all of their goals (GAS = 0) and 50% reported improvements beyond expectation (GAS = +1 or +2). Twenty percent of participants had a GAS lower than the expected achievement (GAS = –1) in decreasing arm flexion. None reported a deterioration from their baseline status (GAS = –2).
Adverse events
One participant reported minor swelling of the arm during casting, but the discomfort was tolerable. The problem was resolved after the cast was removed. No other adverse events were reported.
Analysis of confounding variables
Analysis using a simple regression model found no significant effect of individual participant charac-teristics (age, sex, type of ABI, side of injury and mean dose of toxin injected) on outcome measures. No correlations were found between duration of ABI and outcome measures.
To our knowledge, this is the first published study exploring the effect of combining BoNT injection with casting on gait parameters in patients with ABI who have elbow flexor spasticity. This research builds on previous work suggesting that improvement in elbow flexor spasticity may improve gait without treatment for the lower limbs (6, 11). A systematic review of BoNT injection of spastic upper limb on gait parameters found 3 studies in which gait speed was significantly improved (11). However, amongst these studies, there was no consensus as to which parameters correlated with the improved gait (11).
Although improved gait speed has been demonst-rated in several studies with treatment of elbow flexor spasticity, the mechanism is not precisely known (6, 11, 21). One proposed mechanism suggests that BoNT indirectly alters functional organization of the central nervous system (CNS) through reducing muscle overactivity in afferent fibres, which feed to spinal interneurones and cortical areas, thereby reducing the aberrant efferent signals to muscles seen in spasticity (6). This may lead to improved walking symmetry and speed, through better coupling patterns of arm and leg movements and possible ankle and foot rotation, which may account for the gait quality and speed improvements observed in our study.
In the current study population, all participants were initially referred to the clinic for management of elbow flexor spasticity, and were all ambulators, with 90% being community ambulators and 10% being indoor-only ambulators. In this subset of patients, focusing on treatment of the upper limb with combination therapy of BoNT and casting served as a means to not only improve their upper extremity-related goals, but to also improve gait without treatment applied to the lower limb.
In a recent RCT by McAllister et al. published in the Journal of Rehabilitation Medicine, split dosing of BoNT between the upper and lower limbs vs lower limb alone to treat spastic hemiparesis was shown to result in similar improvements in walking speed (21). In this RCT, patients in the combined upper and lower limb treatment group underwent 4 treatment cycles, with the first 2 cycles being only lower limb injections and the last 2 cycles being split dosing between upper and lower limbs. The combined upper and lower limb treatment group improved to a similar level to the lower-limb-only group on walking speed once upper limb injection became available. This suggests that upper limb treatment may be necessary for gait improvements in a subset of patients with upper limb spasticity (21). In line with these findings, the current study provides preliminary support that treatment for elbow flexor spasticity targeting primarily brachioradialis and brachialis with BoNT and adjunctive casting can be useful to improve gait in people with spastic hemiparesis after ABI.
In addition to objective measurements on gait, GAS was used in the current study as a subjective patient-centred outcome measure. All participants reported subjective improvements in their gait, regardless of the findings of objective measures. This can be due to presumption of therapy effects or placebo effects. This mirrors the findings of a prospective pilot study, in which participants treated with BoNT for elbow flexor spasticity reported improvements in walking without changes in objective parameters of balance or mobility (22). A proposed mechanism for this observation is a reduction in the energy required for walking with decreased muscle spasticity (22). However, a placebo effect cannot be ruled out. Interestingly in the current study, 20% (2 participants) reported achieving less than the expected outcome (GAS = –1) in decreasing arm flexion; however, both of these participants showed clinical improvements in Tardieu V3 and V1 of the elbow and gait parameters. In these participants, the improvements in objective measures may not have translated to noticeable improvements in daily life. This highlights the need for combined use of objective and self-reported outcome measures (22).
While there was a statistically significant difference in MAS, the MCID was not reached by most participants (70%). MCID is intended to measure both magnitude of improvement and subjective value placed on the change by patients (23). It is not uncommon for the observed effect to be smaller than the predefined MCID despite achieving statistical significance (23). The clinical significance of the MAS not reaching MCID is uncertain, given that patients reported subjective improvements on the GAS. A larger high-powered study would be better able to determine the true effect size.
The mean time since ABI for the study cohort was greater than 9 years (Table I). Previous work on com-bined casting and BoNT treatment approach for the lower limb report a mean time since ABI of 4.4 years (13, 24–26). The overall improvements found in the present study suggest that this combined treatment approach can be useful for ambulant people with chronic ABI.
This study focused on the effect of the combined treatment on spasticity rather than passive joint range. As a result, only one cast was applied because we hypothesized that it would be sufficient in providing additional benefit as an adjunct to BoNT. This notion was supported by the current study and a previous study (24). The finding of improvements of Tardieu angle of V3, but not V1, was therefore expected. The purpose of single casts is reported to improve spasticity, while serial casting has been shown to lengthen contractures, which is congruent with the current findings (27). Future studies should assess and better delineate between spasticity and contracture management to improve gait.
In line with previous studies on BoNT and casting, the current study supports that BoNT may reduce the risk associated with casting (14). Theoretically, the relaxation of spastic muscles with BoNT would lead to lower force generated on potential pressure points within the cast, leading to a decreased risk of skin breakdown.
Study limitations and future directions
Study participants were drawn from a convenience sample attending a community spasticity clinic. A prospective case series was performed and as such, there was no control group; it is therefore not possible to determine whether the improvements observed were a result of the study intervention (i.e. a single cast). Furthermore, the study population was both small and heterogeneous, and thus further high-quality randomized controlled studies are still needed to better understand the effectiveness of combining BoNT injection with casting on gait parameters in patients with ABI who have elbow flexor spasticity.
The established 2MWT requires a circular track. However, in the current study, the 2MWT was conducted on a 3-m walkway due to space limitations. We, therefore, can only comment on improvements between t0 and t1, and not on how the patients compared with established value for MCID as this could have been influenced by turning abilities. Measures were put in place to improve reliability of data by using standardized procedures and instructions. Enhanced performance because of repeat exposure was unlikely, due to time lag between assessments
The torque applied was not standardized when assessing range of movement during Tardieu assessment, which may have allowed for unintentional bias; how-ever, as the assessment was conducted by the same physician for all participants, we expect consistency with regards to the velocity component of V3 between assessments. Future studies should apply standardized torque to improve validity of the Tardieu assessment.
Gait was assessed only at time t1 (3 weeks post-injection)
and not at time t2 (3 months post injection). It would also be useful to follow up this cohort longitudinally beyond 3 months post-injection to determine long-term effects in MAS, Tardieu, gait and patient goals.
When designing future RCTs it may be interesting to investigate whether combination therapy of a single upper limb cast post-BoNT injection to the elbow flexors improves gait parameters more than using BoNT alone, and whether this adjunctive therapy may reduce or delay the need for repeated injections. Future studies may also examine the combined treatment for upper and lower limbs vs upper limb treatment alone using casting and the same amount of BoNT on hemiparetic gait parameters.
Clinical messages
A reduction in elbow flexor spasticity following BoNT injection and adjunctive casting may improve hemiparetic gait in ambulatory patients with ABI.
Patients with ABI can benefit from treatment of elbow flexor spasticity to improve gait long after they sustained the injury.
BoNT injection may reduce the risk associated with casting.


 Click to show fullsize
Click to show fullsize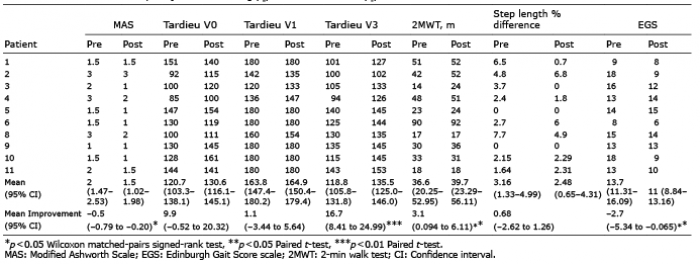 Click to show fullsize
Click to show fullsize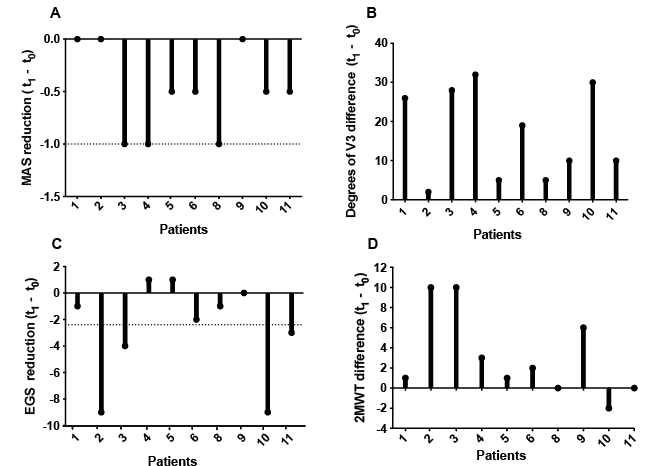 Click to show fullsize
Click to show fullsize