
From the 1Department of Rehabilitation Medicine, Erasmus University Medical Center, Rotterdam, The Netherlands, 2Center for Rehabilitation in Global Health Systems, WHO Collaborating Center, Department of Health Sciences and Medicine, University of Lucerne, Switzerland and 3Swiss Paraplegic Research (SPF), Nottwil, Switzerland
Although we are currently overwhelmed by the astonishing speed of infection of the Covid-19 pandemic, and the daily onslaught of new, and ever-worsening predictions, it is vital that we begin to prepare for the aftershocks of the pandemic. Prominent among this will be the cohort of post-intensive case survivors who have been mechanically ventilated and will likely experience short- and medium-term consequences. The notion that patients surviving intensive care and mechanical ventilation for several weeks can be discharged home without further medical attention is a dangerous illusion. Post Intensive Care Syndrome and other severe conditions will require not only adequate screening but early rehabilitation and other interventions. Action must be taken now to prepare for this inevitable
aftershock to the healthcare system.
Key words: Covid-19; Post Intensive Care Syndrome; Rehabilitation.
Accepted Apr 14, 2020; Epub ahead of print Apr 14, 2020
J Rehabil Med 2020; 52: jrm00044
Correspondence address: Gerold Stucki, Center for Rehabilitation in Global Health Systems, WHO Collaborating Center, Department of Health Sciences and Medicine, University of Lucerne, Switzerland
In 2020, the world community is experiencing a pandemic from a novel coronavirus Covid-19 that touches every corner of the world. During a pandemic, it is easy to get overwhelmed by the astonishing speed of infection and the daily onslaught of new, and ever-worsening predictions. Pandemics are extraordinary public health challenges that demand targeted and coordinated responses by health care systems and governments. But this pandemic, almost from the outset, has also raised the specter of utter health systems failures to cope with the ‘surge’ of demand, putting not only Covid-19 victims at risk but all other individuals who require health care services.
Researchers at the Institute of Health Metrics and Evaluation (IHME) at the University of Washington in Seattle, Washington, USA, modeled expected impacts of the pandemic on healthcare resources (1). They estimated that by mid-May the excess demand from Covid-19 is predicted to be nearly 65,000 hospital beds, and 17,000 intensive care unit (ICU) beds, while ventilator use is predicted to be as high as 20,000. These data constitute a burden that “is well beyond the current capacity of hospitals to manage, especially for ICU care” (2). It is expected that the results for the rest of the world, once they are available, will be worse, especially for low and middle resource countries (3).
It is not premature to begin to think past the pandemic when incidence and death rates are reduced to a point where more general population immunity – enhanced by the eventual vaccination options – becomes likely. From our current perspective, it is difficult to imagine this, but we must not only keep this in mind but urgently prepare for what amounts to the more long-lasting aftershocks of the pandemic.
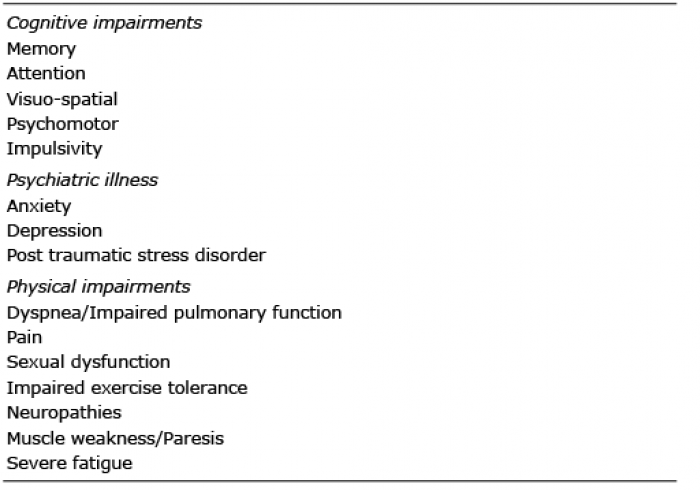
As disease-causing respiratory distress, Covid-19 in a minority of cases (the Italian experience suggests around 15%) (4) often involving elderly individuals or those with chronic comorbidities, requires intensive care and reliance on ventilators. A distinctive feature of this disease is that when necessary, acute and intensive care and ventilator reliance are required for a considerably longer period – perhaps as high as 20 days (5, 6) – than more typical uses of ICU. Until countries begin to experience a decrease in incidence, these hospitalization and ICU usage rates will be a major concern. But as patients improve and are discharged home, the pandemic will cause an aftershock: recovery from the consequences of severe respiratory illness and the secondary disabilities that result from intensive care treatments, including Critical Illness Polyneuropathy (CIP) and Critical Illness Myopathy (CIM), as part of the Post Intensive Care Syndrome (PICS) (Video; Table I) (7).
Table I. Post Intensive Care Syndrome (PICS)
The notion that patients surviving intensive care and mechanical ventilation for several weeks can be discharged home without further medical attention is a dangerous illusion. The longer a patient remains in the ICU, the higher the risk for long-term physical, cognitive and emotional complications. Among the major risk factors are cognitive impairments, acute brain dysfunction, hypoxia, hypotension, and glucose dysregulation (8). Cognitive impairments, including delirium, have been reported in between 30% and 80% of post-ICU patients, varying in severity and duration depending on pre-existing cognitive deficits and age (9). The risk factors for PICS are shown in Table II. One-year outcomes of PICS have been reported to include new symptoms such as dyspnea, pain, sexual dysfunction, impaired pulmonary function and impaired exercise tolerance. But the most common complications are neuromuscular, resulting in poor mobility, frequent falls, even quadriparesis (6). CIP and CIM syndromes seen in approximately 25–45% of critically ill patients during and after intensive care stays with mechanical ventilation – exhibit even more severe neurodegenerative complications, including flaccid and symmetric paralysis, limb and respiratory muscle weakness, systemic inflammatory response syndrome, or multiple organ failure (10).
Table II. Risk Factors for Post Intensive Care Syndrome (PICS)
The long-term impacts of extended periods in ICU are not only highly disruptive to the health of individuals; but also to the society (11–13). Nearly a third of patients who experience PICS do not go back to work, and another third do not go back to their pre-ICU job, or a job with a pre-ICU salary. At least 25% of these patients experience a dramatic loss of independence and require assistance in activities in daily living one year after ICU admission, putting an enormous burden on informal and formal caregivers (14). Patients experiencing CIP suffer from decreased exercise capacity, disability and compromised quality of life for months, even years after intensive care.
There is a range of established clinical responses to these syndromes that control risk factors to avoid or limit the use of neuromuscular blocking agents and corticosteroids (15,16). There is a clear consensus that “early rehabilitation combining mobilization with physiotherapy is emerging as an important strategy to treat critical illness polyneuropathy and myopathy, and to facilitate and improve long-term recovery and functional independence of patients, and shorten the duration of ventilation and hospitalization” (8).
Now is the time to acknowledge and take seriously the need for a coordinated response to the anticipated cohort of post-ICU patients that the Covid-19 pandemic will create over the next several months, across countries of the world. Patients and their caregivers need to be informed about what may be health consequences after the stay in the ICU as well as the long duration of limitations in functioning and the option to seek counseling and treatment.
The size of this cohort will be unprecedented as the disease surge will yield a large number of patients vulnerable to PICS and other less serious consequences of intensive care and mechanical ventilation. Many countries of the world are currently experiencing the catastrophic results of not preparing for a pandemic such as that we are experiencing now; it is urgent that countries do not fail to prepare for this major aftershock of the pandemic. Awareness of the inevitability of this aftershock is the first, and most important, step in the call for action. Professional societies across health care professions involved in rehabilitation and acute care can cooperate in the scaling up of the response within countries and regions. They may rely on tools and guidance provided by the World Health Organization (WHO) developed in response to “Rehabilitation 2030: A Call for Action”.
It is vital to establish adequate screening opportunities (15). This may be done by a general practitioner
alone or by a multiprofessional team consisting of a rehabilitation physician, a physical therapist, a psychologist, a critical care physician and others (16). The choice of a screening technique (including telemedicine and other e-health applications) depends on available resources, local healthcare infrastructure and availability of further rehabilitative interventions. There is strong evidence from systematic reviews that the availability and application of rehabilitation interventions are of primary importance to deal with the consequences of intensive care and mechanical ventilation (17–20). This has been supported by several randomized controlled trials as well (21–24).
It is therefore important to turn to the resources of rehabilitation hospitals and specialists in rehabilitation medicine and their multiprofessional teams who are equipped and experienced in providing the necessary interventions for mental, cognitive and physical impairments of the consequences of intensive care and mechanical ventilation. The capacity of both in- and outpatient rehabilitation of patients with PICS consequences will likely be sufficient, as public health social distancing measures might have eased their standard workload from traffic and work-related spinal cord injuries, head trauma and multi-trauma patients. Nevertheless, it remains important for policymakers to prepare to allocate additional resources to facilitate in– and outpatients’ interventions for ICU survivors. Many rehabilitation institutions are already involved in acute care for patients with Covid-19. Some of them are equipped with ICU beds, and most of the rehabilitation institutions admit patients who have been discharged from ICU and are not yet ready to return home. Rehabilitation institutions may alleviate the enormous burden on acute hospitals and take care of a considerable number of patients.
The authors would like to thank Cristiana Baffone (SPF) and the following contributors from the European Academy of Rehabilitation Medicine: Jari Arokoski (Finland), Merce Avellanet (Andorra), Kristian Borg (Sweden), Helena Burger (Slovenia), Maria Gabriella Ceravolo (Italy), Joaquim Chaler (Spain), Anne Chamberlain (UK), Richard Crevenna (Austria), Thierry Deltombe (Belgium), Jean-Pierre Didier (France), Gabor Fazekas (Hungary), Christoph Gutenbrunner (Germany), Elena Ilieva (Bulgaria), Alvydas Juocevicius (Lithuania), Jaro Karppinen (Finland), Carlotte Kiekens (Italy/Belgium), Jolanta Kujawa (Poland), Jorge Lains (Portugal), Antti Malmivaara (Finland), Angela McNamara (Ireland), Xanthi Michail (Greece), Stefano Negrini (Italy), Rory O’Connor (UK), Johan H. Rietman (Netherlands), Cecile Røe (Norway), Jean Paysant (France), Brigitte Perrouin-Verbe (France), Konstantina Petropoulou (Greece), Joao P. Pinheiro (Portugal), Diane Playford (UK), Bengt Sjölund (Denmark/Sweden), Britt-Marie Stålnacke (Sweden), Katharina Stibrant Sunnerhagen (Sweden), Guy Vanderstraeten (Belgium), Anthony B.Ward (UK) and Mauro Zampolini (Italy).


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize