
From the 1Department of Rehabilitation Medicine, Konkuk University School of Medicine and Konkuk University Medical Center, 2Center for Neuroscience Research, Institute of Biomedical Science & Technology, Konkuk University, 3Research Institute of Medical Science, Konkuk University School of Medicine, Seoul, Korea and 4Program in Occupational Therapy, Washington University School of Medicine, St Louis, MO, USA
*These authors contributed equally to this work as first authors.
Background: Acquired brain injury can cause disorders of consciousness. An additive effect of cerebrolysin and amantadine has been postulated, but not systematically studied. The present study aimed to investigate this additive effect in patients with disorders of consciousness secondary to acquired brain injury.
Methods: The medical records of patients diagnosed with disorders of consciousness after acquired brain injury were reviewed. The patients were categorized into 2 groups: single regimen (amantadine only) and dual regimen (amantadine plus cerebrolysin). The patients’ conscious states were assessed using the Coma Recovery Scale-Revised (CRS-R) before, and after 4 weeks of drug administration.
Results: Data for a total of 84 patients were analysed. The degree of change in CRS-R and the proportion of patients in the disorders of consciousness category showing a change was higher in the dual regimen group than in the single regimen group. Analysis of patients who had initially been in a prolonged vegetative state or minimally conscious state minus before administration showed that the patients in the dual regimen group had greater increases in CRS-R scores than those in the single regimen group.
Conclusion: This study identified that an amantadine-plus-cerebrolysin regimen additively affects patients with prolonged disorders of consciousness. A future controlled trial is needed to investigate the efficacy of each regimen in patients with prolonged disorders of consciousness secondary to acquired brain injury, particularly for patients who have remained in a prolonged vegetative state after acquired brain injury.
Key words: cerebrolysin; amantadine; disorders of consciousness; acquired brain injury; responsiveness.
Accepted Jan 28, 2020; Epub ahead of print Feb 14, 2020
J Rehabil Med 2020; 52: jrm00025
Correspondence address: Jongmin Lee, Department of Rehabilitation Medicine, Konkuk University School of Medicine and Konkuk University Medical Center, Seoul, Korea. E-mail: leej@kuh.ac.kr
Acquired brain injury can impair the conscious state. This study aimed to investigate how cerebrolysin and amantadine positively affect patients with impaired conscious state caused by acquired brain injury. The medical records of patients diagnosed with impaired conscious state caused by acquired brain injury were reviewed. The study included only patients who had initially been in a vegetative state, or had low levels of behavioural interaction, before drug administration. Data for a total of 84 patients were analysed and the patients were divided into 2 groups: a group received amantadine only (“single regimen”), and a group received amantadine plus cerebrolysin (“dual regimen”). The patients’ conscious states were assessed using the Coma Recovery Scale-Revised (CRS-R) before, and after 4 weeks of drug administration. The dual regimen group showed more favourable results, in that their CRS-R scores increased more than those in the single regimen group. This study shows that an amantadine-plus-cerebrolysin regimen additively affects patients with a prolonged state of impaired consciousness. A future controlled trial is needed to investigate the efficacy of each regimen for patients with prolonged states of impaired consciousness.
Acquired brain injury (ABI), including stroke, traumatic brain injury (TBI), and hypoxic brain injury, can result in disorders of consciousness (DOCs), which are impaired states of consciousness, including the vegetative state (VS) and the minimally conscious state (MCS). The VS is characterized by wakefulness without awareness, whereas the MCS is characterized by limited but discernible evidence of awareness toward the self and the environment (1). In the USA, 200 people per million population experience severe brain injury each year, which may result in impaired consciousness (2), while the annual incidence of VS is estimated to be 4,200 cases (3). In long-term care facilities in Austria, the prevalence of VS and MCS are 3.36 and 1.5, respectively, per 100,000 patients with stroke, TBI, anoxic brain injury, intoxication, or inflammatory disease (4). If a DOC lasts longer than 28 days (4 weeks) after the ABI, it is classified as a “prolonged DOC (PDOC)”. More than 10% of patients with severe TBI remain in a VS after acute-stage care (5). In the USA, 56–170 patients per million population with prolonged loss of consciousness due to severe TBI are reported each year (6). The cost of lifetime care for a patient with a PDOC is estimated to exceed US $ 1,000,000 (3). DOCs thus pose a heavy burden on patients’ families, as well as on society, and they raise many legal and ethical issues (7, 8). For this reason, various studies have been conducted to improve the consciousness of patients with ABI, and several have demonstrated the effects of medication on DOCs (9, 10).
Amantadine is known to enhance neurotransmission, through the activation of dopamine-dependent brain circuits (11), and increases dopamine activity in presynapses and postsynapses, acting as an antagonist of the N-methyl-D-aspartate receptor (12). Amantadine treatment has been shown to be correlated with increased metabolism in the frontoparietal network of a patient in an MCS (13). Analysis of positron emission tomography (PET) data showed a significant increment in left pre-frontal cortex glucose metabolism after administration of amantadine (14), and several clinical trials conducted in patients with DOCs have confirmed that amantadine hastens functional recovery (15) or elevates the arousal level of patients with TBI (16). Other studies have led to amantadine becoming a widely accepted medicine for recovering consciousness after TBI (9, 17). Furthermore, the drug has been reported to improve consciousness in patients with DOCs caused by non-traumatic brain injury. For example, in 1990, Horiguchi et al. (18) reported a case of clinically significant recovery after amantadine administration in a patient who had been in a VS for 3 years due to olivopontocerebellar atrophy. In another study, patients who had remained in an MCS for 21 days due to inadvertent rupture of the left middle cerebral artery showed significant recovery of consciousness after administration of amantadine, and their level of consciousness was dose-dependent (19). In addition, amantadine has been reported to improve consciousness in comatose patients after cardiac arrest (20). However, in a randomized, double-blind, placebo-controlled crossover trial no significant effect was found on impaired consciousness secondary to ABI (11).
Cerebrolysin, which consists of peptides and amino acids and is extracted from porcine brain tissue, is a nootropic drug with neuroprotective and neurotrophic properties (21). Specifically, it consists of 15% low molecular weight peptides and 85% amino acids (22). Cerebrolysin is known to inhibit the cell damage caused by excitotoxicity, free radicals, and neuroinflammation (23–26), and to improve cell survival and neurogenesis by stimulating neurotrophic factors in damaged brain tissues (21, 27). Studies using the mild TBI rat model showed that cerebrolysin significantly improves long-term cognitive function, which was found to be correlated with increased neuroblast formation and neurogenesis (28). A double-blinded, placebo-controlled, randomized phase II pilot study in patients with mild TBI demonstrated that cerebrolysin is effective in the improvement of patients’ cognitive functions (29). In patients with severe TBI, a significant improvement in Glasgow Coma Scale (GCS) scores was observed between 10 and 30 days in the cerebrolysin treatment group (30). In a study of patients with severe Alzheimer’s disease, a significant improvement in cognitive function and activities of daily living was observed after 24 weeks of cerebrolysin treatment (31). In a study involving 119 patients who had experienced acute ischaemic stroke, the National Institutes of Health Stroke Scale score was significantly increased after 30 days in the cerebrolysin treatment group with severe neurological deficits (32). However, a recent Cochrane review suggests no clinical benefit of cerebrolysin on mortality of patients with acute ischaemic stroke (33).
Given what is known about the mechanisms of amantadine and cerebrolysin, the positive effects of these drugs on consciousness recovery in patients in a post-ABI state are probably mediated through the drugs’ respective pathways, thereby activating neuronal networks in the injured brain. In addition, additive effects are expected if the drugs are used in combination, although this has never been systematically studied. Therefore, the present study aimed to investigate the additive effect of cerebrolysin and amantadine on restoring consciousness in patients with DOCs secondary to ABI.
This study reviewed the medical records of all patients with a DOC after ABI who had been administered either amantadine only, or amantadine plus cerebrolysin, at the Department of Rehabilitation Medicine of one university hospital between 1 January 2013 and 31 December 2017. The study was approved by the Institutional Review Board of the university hospital. The requirement for patient consent was waived by the review board due to the retrospective design of the study.
The attending physician prescribed amantadine to patients who had a DOC due to ABI, unless they were medically unstable and epileptiform discharge was detected in the electroencephalogram. Patients who did not show significant recovery of consciousness after 1 month of ABI, those who showed good compliance with multi-drugs and whose primary caregivers agreed to the cerebrolysin administration, also received cere-brolysin. Exclusion criteria were: patients who were prescribed other cognitive enhancers or antiepileptic drugs. Nootropics were administered throughout the patients’ hospital stay, lasting approximately 1 month. For the current study, the schedule of amantadine administration used in the previous randomized controlled trial (RCT) was modified (8). Amantadine was administered orally twice a day at a dose of 100 mg in the first week, 150 mg in the second week, 200 mg in the third week, and 100 mg in the fourth week as the maintenance dose. Cerebrolysin was administered intravenously twice a day (dose 2.125 g/10 ml per injection). During the drug administration period, patients were allowed to continue their rehabilitation therapy, e.g. mat exercises, depending on their functional status. Cognitive enhancers were terminated when serious complications (e.g. seizures) or medical conditions (e.g. pneumonia) occurred during the administration period.
The Coma Recovery Scale-Revised (CRS-R) was used to evaluate patients’ levels of consciousness. The CRS-R score ranges from 0 to 23, with higher scores indicating a higher level of neurobehavioural function. This scale is a neurobehavioural assessment measure consisting of 23 items and 6 subscales that assess auditory function, visual function, motor function, verbal function, level of communication, and level of arousal in patients with DOCs (25). The CRS-R is one of the most standardized neurobehavioural assessment tools (26) by which physicians can identify the specific type of DOC present in a patient (VS or MCS). This study conducted CRS-R assessments on 2 occasions to evaluate the conscious states of the patients: first, within the 2 days prior to drug administration, and secondly, 2 days prior to drug discontinuation. Based on information obtained from their caregiver regarding diurnal variation in the patient’s consciousness, the attending physician assessed the CRS-R score at the time when the level of consciousness was expected to be optimal. A further 2 physicians reviewed the measured CRS-R scores and confirmed the final score. Based on CRS-R scores, patients were classified as either VS, MCS–, or MCS+. MCS+ was defined by the presence of command-following, intelligible verbalization, or gestural or verbal yes/no responses (34). MCS– describes low-level behavioural interaction characterized by the presence of non-reflex movements (i.e. visual pursuit or localization of noxious stimulation).
Disease chronicity was defined as follows: acute stage, within 1 month after onset; subacute stage, from 1 to 6 months after onset; chronic stage, later than 6 months after onset.
Statistical analysis
Comparisons of clinical characteristics between the 2 groups were performed using R software (version 3.3.2; http://www.r-project.org). For continuous variables, the Student’s t-test or the Mann-Whitney U test was used to compare between groups, using the parametric or non-parametric test according to whether the respective datasets were normally distributed and homoscedastic. For categorical variables, the χ2 test or Fisher’s exact test was used depending on the expected frequencies. A p-value < 0.05 was considered significant.
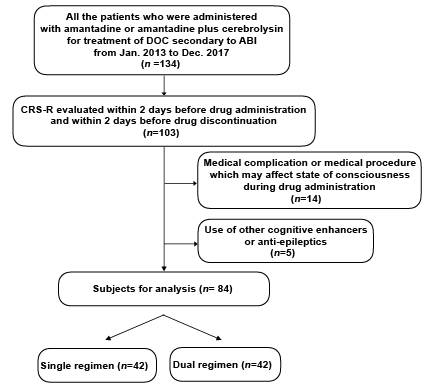
A total of 84 patients with DOCs were included in the analysis (Fig. 1). The mean age of the patients was 60.2 (standard deviation (SD) 17.1) years, and 37 patients (44.1%) were women (Table I). In particular, 36 of the patients had experienced haemorrhagic stroke, 23 had experienced ischaemic stroke, 17 had TBI, 5 had hypoxic brain injury, and 3 had unspecified injuries (2 metabolic encephalopathy and 1 leukoencephalopathy). The mean initial CRS-R total score was 10.7 (SD 4.4), and the interval between disease onset and treatment was 24.9 (SD 25.6) weeks. According to the CRS-R assessment, 21 patients were diagnosed with VS and 63 with MCS (39 with MCS– and 24 with MCS+).
Fig. 1. Flowchart of the patient enrollment procedure. ABI: acquired brain injury; DOC: disorder of consciousness; CRS-R: Coma Recovery Scale-Revised.
Forty-two patients (50.0%) were administered amantadine plus cerebrolysin, defined as the dual regimen group; 42 patients (50.0%) were administered amantadine only, defined as the single regimen group. Mean significant differences were observed between the groups in terms of age (single regimen group: 65.6 (SD 15.5) years, dual regimen group: 54.8 (SD 17.2) years; p = 0.004), category of disease (p = 0.039), chronicity of disease at the time of drug administration (single regimen group: 8 acute, 19 subacute, and 15 chronic; dual regimen group: 1 acute, 26 subacute, and 15 chronic; p = 0.038), initial CRS-R total score (single regimen group: 13.1 (SD 4.2), dual regimen group: 8.2 (SD 3.1); p < 0.001), follow-up CRS-R total score (single regimen group: 15.9 (SD 4.1), dual regimen group: 12.4 (SD 4.4); p < 0.001), change in CRS-R total score (single regimen group: 2.8 (SD) 3.1, dual regimen group: 4.2 (SD 3.3); p = 0.027), initial category of DOC (single regimen group: 6 VS, 15 MCS–, and 21 MCS+; dual regimen group: 15 VS, 24 MCS–, and 3 MCS+; p < 0.001), and follow-up category of DOC (single regimen group: 3 VS, 8 MCS–, 25 MCS+, and 6 EMCS; dual regimen group: 3 VS, 22 MCS–, 14 MCS+, and 3 EMCS; p = 0.032). We included and assessed the patients who received amantadine (± cerebrolysin) and were assessed by CRS-R before and after drug administration. Therefore, drop-out/death numbers was 0.
There were no significant differences in the duration of treatment between the groups. During the treatment period, no significant adverse effects or medical complications, including seizures or cardiovascular problems, were observed in either of the groups.
A difference was also found in the type of DOC category change between the groups, albeit without statistical significance (single regimen group: 27 no change, 2 VS to MCS–, 1 VS to MCS+, 6 MCS– to MCS+, 3 MCS– to EMCS, and 3 MCS+ to EMCS; dual regimen group: 17 no change, 9 VS to MCS–, 3 VS to MCS+, 10 MCS– to MCS+, 1 MCS– to EMCS, and 2 MCS+ to EMCS; p = 0.077) (Table I).
Table I. Characteristics of patients according to the regimen administered: single regimen (amantadine only) and dual regimen (amantadine plus cerebrolysin)
The clinical variables of patients who were initially in prolonged VS before drug administration were compared between the groups. There were no significant differences in age, sex, category of disease, chronicity of disease at the time of drug administration, or initial CRS-R total score (Table II). However, a significant difference was found in the mean change in CRS-R total score between the groups (single regimen group: 1.6 (SD 2.1), dual regimen group: 4.7 (SD 3.7); p = 0.038). A difference was also observed in the category of DOC at follow-up assessment between groups, albeit without statistical significance (single regimen group: 3 VS and 2 MCS–, dual regimen group: 3 VS, 9 MCS–, and 3 MCS+; p = 0.195). The change in CRS-R total score according to the disease entity is shown in Fig. 2. All the patients with TBI (3 subacute and 3 chronic) who were initially in a VS and received the dual regimen showed a significant change in DOC category.
Table II. Efficacy of the respective regimen for the patients in a prolonged vegetative state
Fig. 2. Changes in Coma Recovery Scale-Revised (CRS-S) scores in patients who were in a prolonged vegetative state. ⎢Patients showing change in consciousness from a vegetative state to minimally conscious state minus (MCS–); υ: patients showing change in consciousness from a vegetative state to MCS+; HS: haemorrhagic stroke; HBI: hypoxic brain injury; IS: ischaemic stroke; TBI: traumatic brain injury.
The change in CRS-R subdomain score was also compared between the groups. A significant difference was observed in the mean change in CRS-R visual function scale score (single regimen group: 0.4 (SD 0.9), dual regimen group: 1.7 (SD 1.3); p = 0.044). Differences were also found in the change in CRS-R auditory function scale score (single regimen group: 0.4 (SD 0.9), dual regimen group: 1.1 (SD 1.0); p = 0.200) and motor function scale score (single regimen group: 0.2 (SD 0.5), dual regimen group: 1.1 (SD 1.1); p = 0.070), albeit without statistical significance. The groups were divided according to the responsiveness to the respective regimen. No differences were found in age, category of disease, or chronicity of disease at the time of drug administration between the groups.
The clinical variables of patients who remained prolonged MCS– before drug administration were compared between the groups. There were significant differences in mean age (single regimen: 63.0 (SD 12.5), dual regimen: 50.7 (SD 18.6); p = 0.036) and initial CRS-R total score (single regimen: 12.6 (SD 3.0), dual regimen: 9.5 (SD 2.3); p = 0.012) between the groups. A difference was also found in change in CRS-R total score (single regimen: 1.7 (SD 1.9), dual regimen: 3.4 (SD 2.7); p = 0.067), albeit without statistical significance. No difference was found in the category of DOC at follow-up assessment between groups (single regimen group: 5 MCS– and 5 MCS+, dual regimen group: 13 MCS–, 9 MCS+, and 1 EMCS; p = 0.711). The change in CRS-R total score according to the disease entity is also shown in Fig. 3. Only one patient with haemorrhagic stroke, who had emerged from MCS, received the dual regimen. No patients with TBI who remained prolonged MCS– showed a significant change in conscious state.
A significant difference was observed in the mean change in CRS-R oromotor/verbal function scale score (single regimen: –0.1 (SD 0.3), dual regimen: 0.5 (SD 0.6); p = 0.008). A difference was also found in the mean change in CRS-R auditory function scale score (single regimen group: 0.3 (SD 0.7), dual regimen group: 0.8 (SD 0.9); p = 0.114) and motor function scale score (single regimen group: 0.2 (SD 1.3), dual regimen group: 0.8 (SD 1.1); p = 0.127), albeit without statistical significance. No differences were found in age, category of disease, or chronicity of disease at the time of drug administration between the groups, according to responsiveness to the respective regimen.
Fig. 3. Changes in Coma Recovery Scale-Revised (CRS-R) score in patients who were in prolonged minimally conscious state minus. ⎢Patients showing change in consciousness from minimally conscious state minus (MCS–) to MCS+; υ: patients showing change in consciousness from MCS– to “emergence from MCS”; HS: haemorrhagic stroke; HBI: hypoxic brain injury; IS: ischaemic stroke; TBI: traumatic brain injury.
In this study the CRS-R scores increased and consciousness improved in both groups of patients with DOCs after ABIs, those on single regimen (amantadine only) and those on dual regimen (amantadine plus cerebrolysin). These results are consistent with those of the previous studies mentioned, which demonstrated the efficacy of amantadine on consciousness recovery in patients after ABI (15, 16, 18–20). The current study also found that even chronic-stage patients showed significant change in DOC after drug administration in both groups. However, it cannot be concluded that the improvement in conscious state among the enrolled patients was attributed solely to the effect of nootropics, because, due to ethical issues, no patients with DOC were assigned to a placebo control group. Furthermore, the current study found that the degree of change in CRS-R and the proportion of patients with significant changes in DOC category were both higher in the dual than in the single regimen group. However, it should be noted that the initial CRS-R total score and the initial DOC categories were significantly lower in the dual regimen group than in the single regimen group.
Patients who were in prolonged VS or MCS– before drug administration showed higher CRS-R score changes in the dual regimen group than in the single regimen group. There is a limitation in generalizing these results to the total population of patients with DOC because the disease entity in patients with prolonged MCS– was somewhat different between groups. In particular, there were more patients with TBI in the dual regimen group; however, this is not thought to have resulted in a false-positive effect of the dual regimen because, for most of the patients who responded in each group, stroke was the cause of DOC. In addition, the fact that the ages in the dual regimen group were lower than in the single regimen group also may have biased the results of the group analysis for prolonged MCS–. However, this is not thought to have resulted in a false-positive effect of the dual regimen because the patients who responded in the dual regimen group were older than those who did not respond to the dual regimen. Future RCTs with good comparability of disease entity and age are needed to confirm the precise efficacy of the dual regimen.
This study also found that administration of dual regimens resulted in a higher number of significant DOC category changes than single regimens among the patients who remained in a prolonged VS. All 3 patients who changed from prolonged VS to MCS+ had received the dual regimen. Only 1 patient who changed from prolonged MCS– to EMCS had also received the dual regimen. None of the patients who received the single regimen had changed from prolonged VS to MCS+ or from prolonged MCS– to EMCS. These results reveal the possibility that cerebrolysin combined with amantadine has an additive effect on improvement of prolonged DOC secondary to ABI. This study also demonstrated that the dual regimen has a positive effect on visual function in the patients who were initially in a VS; the positive effect was also seen for the oromotor/verbal function of the patients who were initially in MCS–, compared with the single regimen.
This study also found that patients who remained in a prolonged VS due to severe TBI tended to respond well to the dual regimen, although, due to the small sample size, it is difficult to generalize this result. The acute phase of recovery from severe TBI involves a brief period of neuronal excitability, followed by a longer period of hypoexcitability characterized by the depletion of multiple neurotransmitters, including dopamine (15). Amantadine increases the activity of dopamine in both presynapses and postsynapses (12). Cerebrolysin also restores damaged brain tissue by activating nerve growth factor (NGF), which in turn stimulates the long-term growth of neurites in the brain (26, 35). In a mouse study, cerebrolysin had positive effects on structural synaptic plasticity (36). Therefore, amantadine combined with cerebrolysin has been postulated to affect consciousness recovery after TBI, by elevating the activity of neural circuits in the brain in an additive manner, which facilitates dopaminergic activity and neural plasticity in the neurotransmitter-depleted and structurally damaged brain.
In a previous study investigating the effect of amantadine on recovery after severe TBI, 100 mg amantadine was administered twice daily for the first 2 weeks. The dose was then gradually increased to 150 and 200 mg for the third and fourth week, respectively (15). In another study, amantadine (100 mg, twice a day) was administered for 1–4 weeks to determine its effect on the recovery of comatose patients after cardiac arrest (20). In a clinical study of children aged 8–14 years who had undergone anoxic brain injury or stroke, a maximal daily dose of 300 mg/day in the first week and 400 mg/day in the second week were used (37). The dose used in the present study was similar to the doses used in these studies.
In an earlier study in patients with severe TBI, 10 ml cerebrolysin was administered for 30 days, starting 1 month after injury (38). In another study of mild TBI, 30 ml cerebrolysin was administered for 5 days, beginning 24 h after injury (29). In a more recent study, 10–50 ml cerebrolysin was administered to patients with severe TBI for 10 days, beginning 6 h after the injury (39). A study using a rat model found that 30 ml cerebrolysin for a person weighing 70–75 kg would be optimal for functional recovery after mild TBI (40). In studies involving patients who had experienced stroke, 30–50 ml cerebrolysin per day was administered for 10–21 days (23, 27). In the present study, 20 ml cerebrolysin was administered daily, irrespective of the patients’ body weights, which was slightly lower than the dose administered in the previously described studies.
In the present study, 7 subacute or chronic patients emerged from MCS after the administration of cognitive enhancers, which are consistent with previous studies. In a clinical trial demonstrating the effect of amantadine on recovery after severe TBI, some patients did emerge from MCS (15). Although the study design was somewhat weak, cerebrolysin was also shown to increase the consciousness level of patients with a DOC to beyond MCS levels (38).
Limitations
The present study has several limitations. First, since the physician decided which patients were administered the dual regimen based on the clinical information of patients, an allocation bias might have occurred. The enrolled patients in each group had different demographic characteristics, including age, disease entity, disease chronicity, and level of consciousness, before drug administration. As a result, the groups may not be directly comparable. However, the clinical characteristics, except for the age of the patients who were initially in MCS–, were not significantly different between the groups of patients with the same level of initial consciousness (Table II and Table III). It is obvious that the patients who had been in MCS– prior to drug administration were younger in the dual regimen group than in the single regimen group. However, the administration of dual regimens to younger patients may not have resulted in false-positive results of the dual regimen effect on the basis that patients who responded to dual regimens were older than those who did not respond to dual regimens. Secondly, the dose of cerebrolysin used in the present study was lower than that used in previous studies, and clinical trials in the future should test doses ≥ 30 ml cerebrolysin. Thirdly, due to design limitations, this study could not confirm whether the effect of cerebrolysin persisted after discontinuation. Finally, this study could not demonstrate the initial changes in CRS-R score because the conscious state of patients was assessed once before, and once after, drug administration.
Table III. Efficacy of the respective regimen for patients with prolonged minimally conscious status minus
Conclusion
An amantadine-plus-cerebrolysin regimen was shown to additively affect the conscious state of patients with prolonged DOC secondary to ABI, especially in patients who remained in a prolonged VS. These preliminary results provide a strong basis for a future well-designed controlled trial to investigate the efficacy of each regimen in patients with DOCs secondary to ABI, and particularly for patients remaining in a prolonged VS state after ABI.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize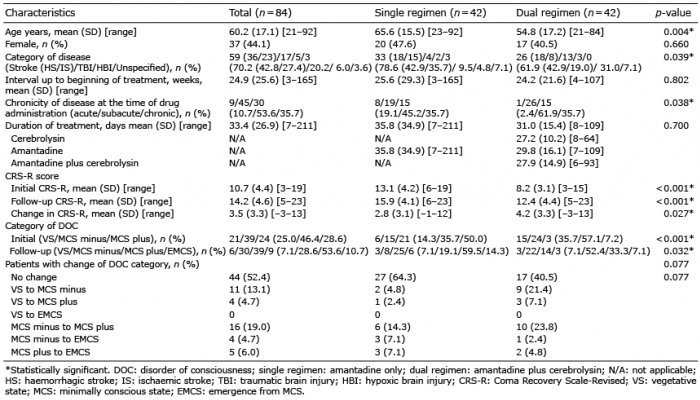 Click to show fullsize
Click to show fullsize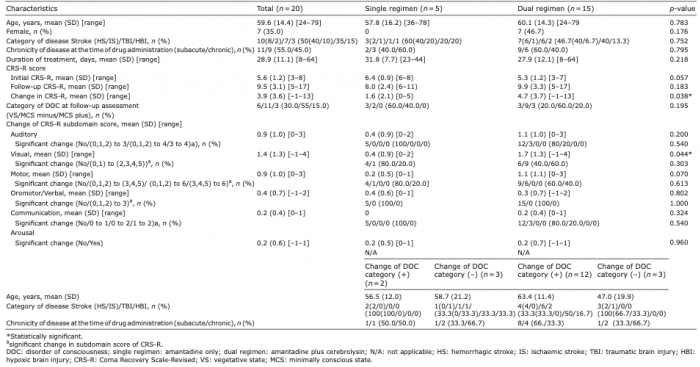 Click to show fullsize
Click to show fullsize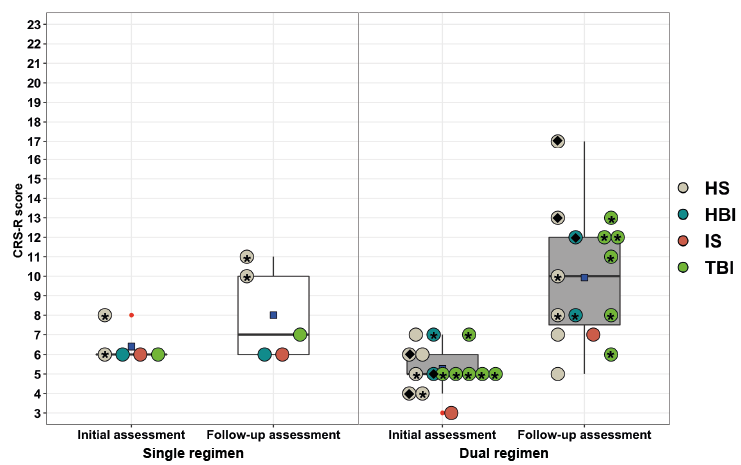 Click to show fullsize
Click to show fullsize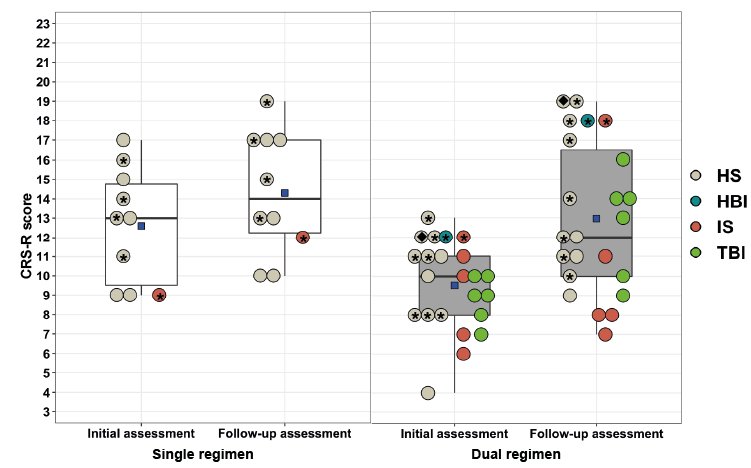 Click to show fullsize
Click to show fullsize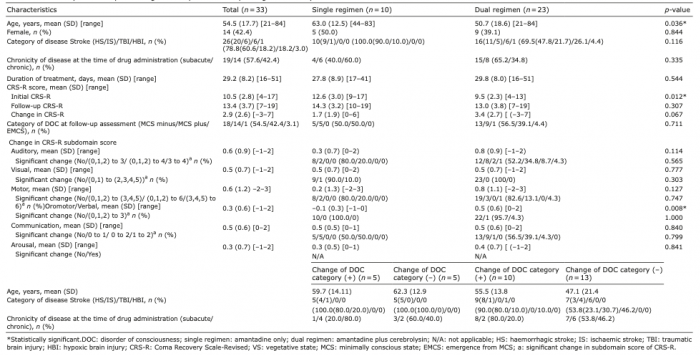 Click to show fullsize
Click to show fullsize