
From the 1Department of Rehabilitation Medicine, Saiseikai Kanagawaken Hospital, Kanagawa, 2Department of Rehabilitation Medicine, Keio University School of Medicine, Tokyo and 3Department of Rehabilitation Medicine I, Fujita Health University School of Medicine, Aichi, Japan
Objective: To examine functional outcomes in patients with subacute stroke who are on haemodialysis.
Design: Observational cohort study.
Subjects: Patients with stroke who were admitted to rehabilitation wards between April 2011 and August 2016 were retrospectively enrolled.
Methods: Data on the Functional Independence Measure (FIM) and discharge destination were collected from medical records as outcomes. Outcomes were compared for patients who received haemodialysis and those who did not. Multiple regression analyses were carried out to explore the impact of haemodialysis on functional outcomes.
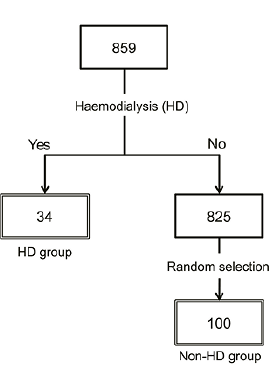
Results: Among 859 patients, 34 (mean age 63.6 years (standard deviation (SD) 11.7)) required haemodialysis while staying in rehabilitation wards. One hundred patients not receiving haemodialysis (mean age 70.7 years (SD 13.8) ) were randomly selected as controls. The total FIM score at discharge, FIM gain, FIM efficiency, FIM effectiveness, and discharge destination were not significantly different between the 2 groups (p > 0.05). Multiple regression analysis, adjusted for other confounding factors, found no significant difference in total FIM score between groups at discharge (p = 0.427).
Conclusion: Dialysis was not an inhibitory factor affecting outcomes during subacute rehabilitation in patients with stroke. Rehabilitation should be considered for patients with subacute stroke requiring haemodialysis, in order to provide every opportunity to achieve adequate functional outcomes.
Key words: activities of daily living; comorbidity; functional outcome; kidney diseases; rehabilitation; renal dialysis; stroke.
Accepted Jan 13, 2020; Epub ahead of print Jan 24, 2020
J Rehabil Med 2020; 52: jrm00033
Correspondence address: Yohei Otaka, Department of Rehabilitation Medicine I, School of Medicine, Fujita Health University, 1-98 Dengakugakubo, Kutsukake, Toyoake, Aichi, 470-1192, Japan. E-mail: otaka119@mac.com
The aim of this study was to clarify whether patients with subacute stroke who are receiving haemodialysis can attain similar functional outcomes after rehabilitation as those not receiving haemodialysis. Stroke patients who were admitted to rehabilitation wards were retrospectively enrolled. Functional outcomes were compared between 34 patients receiving haemodialysis and 100 randomly selected patients not receiving haemodialysis. The results indicate that the functional outcomes were not significantly different between the groups. Furthermore, dialysis was proven to not be an inhibitory factor that affects outcomes after controlling for possible cofounding factors. This study suggests that clinicians should consider rehabilitation for all patients with subacute stroke who require haemodialysis, in order to provide the opportunity for these patients to achieve adequate functional outcomes.
Chronic kidney disease (CKD), including end-stage renal failure, is associated with platelet dysfunction, coagulation disorder, endothelial dysfunction, inflammation, alterations in cardiac output and regional cerebral perfusion, accelerated systemic atherosclerosis, altered blood brain barrier, and the risk of atrial fibrillation; thus, CKD is a risk factor for cerebrovascular diseases (1–5). The incidence rate of ischaemic stroke and haemorrhagic stroke in patients with CKD is much higher than in the general population (6, 7). In addition, the number of patients with end-stage renal disease requiring haemodialysis (HD) is increasing in developed countries, including Japan (8–10). Therefore, clinicians are more frequently encountering stroke patients on HD who are candidates for rehabilitation.
It is well-established that rehabilitation outcomes in general deteriorate with an increasing number of comorbidities and severity of comorbidities (11–13). Patients with end-stage renal failure are more likely to be restricted in daily activities because of various unfavourable conditions, including anaemia, decreased cardiac function, protein energy malnutrition, lower muscle strength, and metabolic disorders (14, 15). However, the effect of CKD on functional outcomes in stroke patients is not well understood. One study (16) with a limited sample of patients with cerebrovascular disease (n = 11) reported that HD patients with cerebrovascular disease had lower motor score gains on the Functional Independence Measure (FIM) than did non-HD patients. The lack of knowledge about functional outcomes in stroke patients with CKD inhibits appropriate decision-making, particularly regarding whether an intensive inpatient rehabilitation programme is relevant to a stroke patient on HD.
The aims of this retrospective study were: (i) to investigate the characteristics of patients with subacute stroke on HD receiving rehabilitation; and (ii) to explore whether the rehabilitation outcomes were different between subacute stroke patients receiving HD and those who were not receiving HD.
Patients
A total of 859 consecutive patients with cerebral infarction or cerebral haemorrhage (excluding subarachnoid haemorrhage) who were transferred to the Kaifukuki Rehabilitation Ward (KRW) in Saiseikai Kanagawaken Hospital from acute hospitals for rehabilitation between April 2011 and August 2016, were reviewed retrospectively. Saiseikai Kanagawaken Hospital is the only rehabilitation facility in Kanagawa-ku at which HD can be performed. Kanagawa-ku is 1 of the 18 wards of the city of Yokohama in Kanagawa Prefecture, Japan. It has an estimated population of 238,578, covering an area of 31.01 km2. Before the review, we estimated the sample size for the analyses. We determined that a sample size of 29 patients for the HD group and 3 times that for the non-HD group (n = 87) was sufficient to detect a difference of 9 points in the FIM score, assuming a standard deviation (SD) of 16 using a 2-tailed t-test of difference between means, with 80% power and a 5% level of significance. For the collection of patients in the HD group, we started with patients seen in August 2016 and worked backwards in time until the sample size was reached. Thirty-four patients with HD were then enrolled, including patients seen between April 2011 and August 2016. For selection of non-HD patients, 100 patients were randomly selected by computer-generated random numbers from a group of patients admitted during the same period who did not receive HD. This study was approved by the ethics committee of Saiseikai Kanagawaken Hospital (No. 16-09).
Subacute rehabilitation in Japan
The KRW system for intensive rehabilitation, a governmental insurance system for rehabilitation of patients in rehabilitation wards during their convalescent period, was introduced in Japan in 2000. Patients were eligible for admission to the KRW within 2 months of onset of stroke. Physical, occupational, and speech therapies lasting for a maximum of 3 h/day were provided as part of the intensive intervention. The KRW team provided patients and their families with a comprehensive monthly rehabilitation plan, including information about achieved goals, planned goals, and rehabilitative approaches to the achieved goals, discharge planning, and social resources necessary for home discharge. Timing for discharge was set when patients reached a plateau in activities of daily living, and the maximum length of stay was 150 days for patients with stroke and 180 days for patients with stroke and accompanying severe disabilities and cognitive disorders.
Data collection
Patient information, including age, sex, days from onset to admission, past history of stroke, types of stroke, side of hemiparesis, motor function on the Stroke Impairment Assessment Set (17), Charlson Comorbidity Index (18), transient discontinuation of rehabilitation, length of stay in the rehabilitation hospital, discharge destination, modified Rankin scale (mRS) (19) before the onset and at discharge, and admission and discharge FIM (20, 21), was collected. Transient discontinuation of rehabilitation was defined as an event of discontinued rehabilitation for medical reasons lasting one day or more. In addition, for the patients on HD, data about the type of renal disease and the duration of dialysis were collected. Information on the total time of rehabilitation undertaken per day was collected and defined as the dose of rehabilitation.
Analyses
Prior to analyses between the HD and non-HD groups, we examined whether the selected non-HD group was a representative sample of whole patients who were not receiving HD. Age, sex, and stroke types were compared between the selected non-HD patients and the rest of the patients who were not receiving HD using an independent t-test or χ2 test.
For baseline comparisons, demographic and clinical variables at admission were compared in the HD and non-HD groups using the independent t-test, Mann–Whitney test, or χ2 test, depending on the type of variables.
Discharge FIM, FIM gain, FIM efficiency, and FIM effectiveness were employed as the functional outcomes (22). Indices were calculated using the following equations:
Gain = discharge FIM-admission FIM
Efficiency = (discharge FIM-admission FIM)⁄Length of stay
Effectiveness = (discharge FIM-admission FIM)⁄(maximum FIM-admission FIM)
Length of stay in the rehabilitation hospital, mean rehabilitation time per day, the number of patients who experienced transient discontinuation of rehabilitation, mRS at discharge, and discharge destination were used as the other outcomes. Outcomes were compared between groups with the Mann–Whitney test or χ2 test, depending on the types of variables.
To investigate whether there was a significant difference in the discharge FIM between the HD group and the non-HD group after adjusting for covariates and possibly confounding variables, we developed a multiple regression model for the discharge FIM with group (HD/non-HD), age, sex, length of hospital stay, admission FIM, mean rehabilitation time per day, and the Charlson Comorbidity Index as covariates. JMP software version 13 (SAS Institute Inc., Cary, NC, USA) was used for statistical analyses. Any p-value < 0.05 was considered statistically significant with no adjustment for multiple comparisons.
The flow diagram of patients is shown in Fig. 1. There was no significant difference in age (mean 70.7 (SD 13.8) vs 71.1 (SD 12.5) years, p = 0.796), sex (male/female, 65/35 vs 425/300, p = 0.280), or types of diseases (haemorrhage/infarction, 44/56 vs 248/477, p = 0.116) in randomly selected non-HD patients (n = 100) and the rest of the non-HD patients (n = 725).
Fig. 1. Flow diagram of patients admitted to Saiseikai Kanagawaken Hospital with cerebral infarction or cerebral haemorrhage between April 2011 and August 2016. HD: haemodialysis.
The characteristics of the patients on admission to the rehabilitation ward in each group are shown in Table I. The causes of HD were diabetes (n = 18), nephrosclerosis (n = 6), glomerulonephritis (n = 4), polycystic kidney (n = 1), and unknown cause (n = 5). The mean duration after the introduction of HD was 8.1 years (SD 6.6). Compared with the non-HD group, patients in the HD group were significantly younger, had a higher Charlson Comorbidity Index, milder upper limb paresis, and better motor, cognitive, and total FIM scores at admission (Table I).
Table I. Characteristics of participants on admission to rehabilitation wards
A patient in the HD group died in the KRW due to severe aspiration pneumonia. The data of this case has been included in the analyses. There were no significant differences in total and motor FIM scores at discharge, FIM gain, FIM efficiency, FIM effectiveness, the number of patients with transient discontinuation of rehabilitation, mRS at discharge, and discharge destination between groups (Tables II and III). The HD group showed significantly shorter lengths of hospital stay. In addition, the HD group showed significantly higher cognitive FIM scores at discharge, although this might be mainly attributed to the significant group difference in the scores at admission. The mean time of rehabilitation per day was 25% shorter in patients on HD than in non-HD patients (Table III). Reasons for the transient discontinuation of rehabilitation were shunt stenosis (n = 2), renal anaemia (n = 2), heart failure (n = 2), and “other” (n = 4) in the HD group. In the non-HD group, the reasons were aspiration pneumonia (n = 6), epilepsy (n = 3), cerebral infarction (n = 1), chronic subdural haematoma (n = 1), and “other” (n = 9).
Table II. Comparison of outcomes of Functional Independence Measure between groups
Table III. Comparison of other outcomes between groups
Multiple regression analysis revealed that the group (HD over non-HD) was not significant. The factors related to the discharge FIM score were the length of hospital stay, total admission FIM score, and the dose of rehabilitation per day (Table IV). Even after excluding the Charlson Comorbidity Index from the model, which also added points for moderate to severe CKD, the result still showed that the group was not significant.
Table IV. Multiple regression analysis for Functional Independence Measure (FIM) score at discharge
This study investigated the characteristics of stroke patients on HD who were receiving subacute rehabilitation, and explored whether the rehabilitation outcomes were different in patients on HD and non-HD patients with subacute stroke in a subacute rehabilitation ward. The patients on HD were significantly younger and had significantly milder upper limb paresis and significantly higher FIM score than non-HD patients at baseline. On the comparison of outcomes between groups, discharge total FIM score, FIM gain, FIM efficiency, FIM effectiveness, and discharge destination were not significantly different between groups (p > 0.05), even though the mean dose of rehabilitation per day was 25% shorter in patients on HD.
Some studies examined the outcomes of stroke patients on HD. Mattana et al. (23) reported that stroke patients on HD could have as good an outcome as those with normal renal function, but were hospitalized longer in an acute hospital setting. Sozio et al. (24) revealed in a large cohort that only 56% of patients successfully escaped death, nursing home, or skilled nursing facility. To the best of our knowledge, however, the characteristics and outcomes of patients on HD receiving rehabilitation have been investigated in only 2 studies with limited numbers of stroke samples, one with only 2 patients (25) and one with only 11 stroke patients (16). Therefore, our findings have valuable implications, even though the sample was not large.
With regard to baseline characteristics, we revealed that patients on HD were in significantly better condition than non-HD patients at baseline. Selection bias regarding candidacy for rehabilitation is the most likely reason for this baseline difference between groups. Although there was no definite evidence that patients on HD will have poorer outcomes compared with non-HD patients, clinicians may tend to choose non-HD patients rather than patients on HD when other conditions are similar, because there are a limited number of rehabilitation hospitals where HD can be performed.
Regarding the rehabilitation outcomes, Forrest et al. (25) reported that the rate of patient discharge to the community was almost the same in patients on HD (34 patients, including 2 stroke) and non-HD patients (497 patients, including 44 stroke). The mean rehabilitation time per day was 27% shorter in patients on HD than non-HD patients. These findings were similar to ours. However, they did not report the findings limited to stroke patients and only 2 HD stroke patients were included. Therefore, these findings cannot be compared with our results. Cowen et al. (16) reported that gains in motor FIM during hospitalization were significantly lower in 11 HD stroke patients with end-stage renal disease compared with those without it. Although the finding also cannot be simply compared with ours because of the limited number of samples and a much shorter mean length of stay in hospital (< 20 days), the finding was different from ours, where FIM gain, efficiency, and effectiveness were not different in HD and non-HD patients. There are 2 possible interpretations for our finding. First, different baseline characteristics might have contributed to the findings. The significantly better condition of HD patients at baseline may have cancelled out the negative effects resulting from intrinsic negative factors in patients on HD, as well as the negative influence of a lesser dose of rehabilitation. The other possible interpretation is that the effects of rehabilitation are truly similar between patients on HD and non-HD patients when rehabilitation is provided over a relatively long-term period in the subacute phase. This explanation was supported by the finding that the discharge total FIM scores were not significantly different between the HD group and non-HD group even after accounting for age, admission FIM, and other possible confounding variables in the multiple regression analysis. We could not conclude which of these interpretations is true; however, we can at least draw the clinical conclusion that HD patients may have a comparable rehabilitation effect to that of non-HD patients during the subacute period.
This study had several potential limitations. The KRW, where the study was conducted, is a unique system for subacute rehabilitation in Japan; and the study was conducted in a single facility. The design of the study was retrospective. Therefore, the generalizability of the findings is limited. Furthermore, although we tried to eliminate the effects of the difference in characteristics between the groups by using a multiple regression model, there is the possibility that the influence of this baseline difference could not be completely removed.
In conclusion, patients on HD with subacute stroke in the rehabilitation ward could have had favourable rehabilitation outcomes, which were comparable to those in non-HD patients. The findings of this study suggest that HD is not a major inhibitory factor for rehabilitation and patients on HD with stroke should have the same opportunities as non-HD stroke patients, because they may benefit from rehabilitation.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize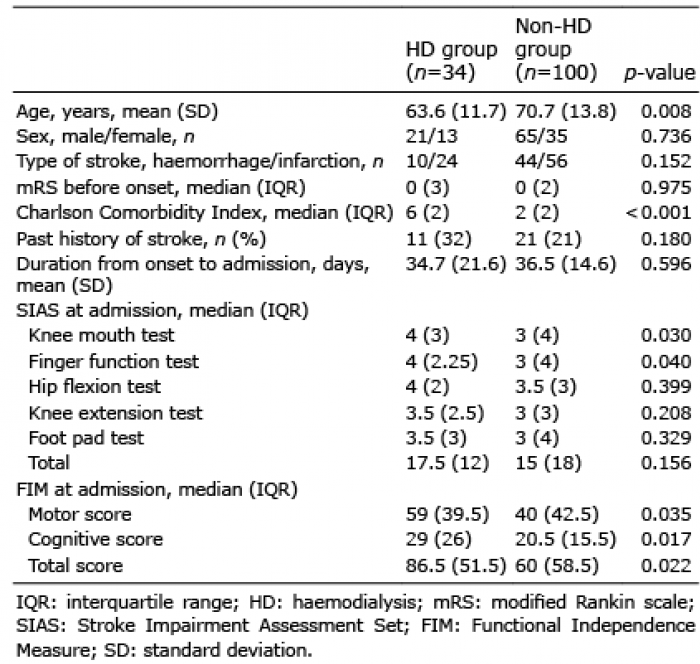 Click to show fullsize
Click to show fullsize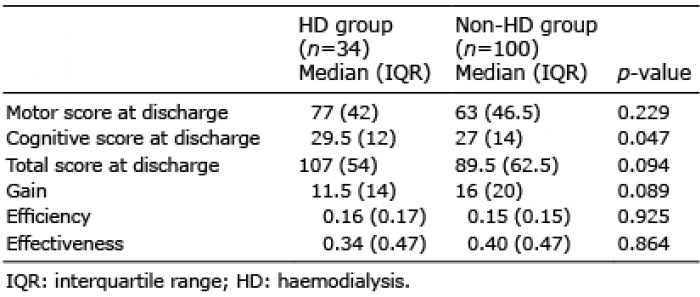 Click to show fullsize
Click to show fullsize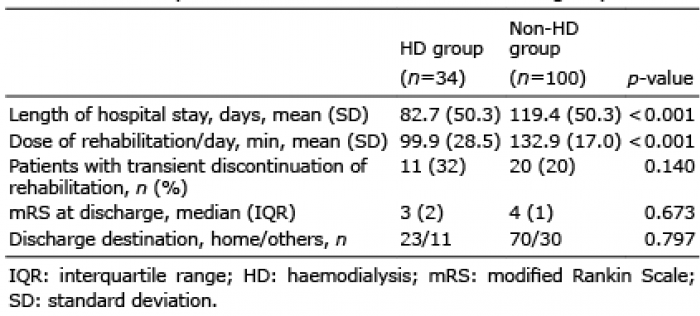 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize