
From the 1Department of Rehabilitation, Amsterdam UMC, University of Amsterdam, Amsterdam Movement Sciences, 2Department of Rehabilitation Medicine, Amsterdam UMC, Vrije Universiteit Amsterdam, Amsterdam Movement Sciences, Amsterdam, and 3Department of Biomechanical Engineering, Delft University of Technology, Delft, The Netherlands
*These authors contributed equally to this work.
Objective: To describe the orthotic properties and evaluate the effects of ankle-foot orthoses for calf muscle weakness in persons with non-spastic neuromuscular disorders compared with shoes-only.
Design: Cross-sectional study.
Subjects: Thirty-four persons who used ankle-foot orthoses for non-spastic calf muscle weakness.
Methods: The following orthotic properties were measured: ankle-foot orthosis type, mass, and ankle and footplate stiffness. For walking with shoes-only and with the ankle-foot orthoses, walking speed, energy cost and gait biomechanics were assessed.
Results: Four types of ankle-foot orthosis were identified: shaft-reinforced orthopaedic shoes (n = 6), ventral ankle-foot orthoses (n = 10), dorsal leaf ankle-foot orthoses (n = 12) and dorsiflexion-stop ankle-foot orthoses (n = 6). These types differed significantly with regards to mass, ankle-and footplate stiffness. Compared with shoes-only, all ankle-foot orthoses/orthopaedic shoes groups combined increased walking speed by 0.18 m/s (95% confidence interval (95% CI) 0.13–0.23), reduced energy cost by 0.70 J/kg/m (95% CI 0.48–0.94) and limited ankle dorsiflexion by –3.0° (95% CI 1.3–4.7). Higher ankle-foot orthoses ankle stiffness correlated with greater reductions in walking energy cost and maximal ankle dorsiflexion angle.
Conclusion: Ankle-foot orthoses for persons with non-spastic calf muscle weakness vary greatly in properties and effects on gait. The large variation in effectiveness may be due to differences in ankle stiffness, although this requires further prospective evaluation.
Key words: ankle-foot orthosis; orthoses; gait; neuromuscular disease; rehabilitation; muscle weakness; disease management.
Accepted Dec 27, 2019; Epub ahead of print Jan 14, 2020
J Rehabil Med 2020; 52: jrm00026
Correspondence address: Niels F. J. Waterval, Department of Rehabilitation, Amsterdam UMC, University of Amsterdam, Amsterdam Movement Sciences, Amsterdam, The Netherlands. E-mail: n.f.waterval@amc.uva.nl
Ankle-foot orthoses are used to improve walking in persons with non-spastic calf muscle weakness. For best results the mechanical properties of the device should be matched with the patient’s impairments. However, there are currently no guidelines about the optimal mechanical properties of ankle-foot orthoses, due to a lack of studies evaluating their effects and properties. In order to establish a baseline and guide further research, we conducted an overview of the mechanical properties and effects of the ankle-foot orthoses provided in usual care in the Netherlands. The results show that, in usual orthotic care, ankle-foot orthoses that are not optimally matched with the patient’s impairments are provided to persons with non-spastic calf muscle weakness. Differences in ankle-foot orthoses ankle stiffness were related with their effects. In general, persons wearing ankle-foot orthoses with the greatest ankle and footplate stiffness showed the largest benefits with regard to improved walking ability, although this warrants further prospective research.
Weakness of the lower leg muscles due to non-spastic neuromuscular disorders, such as Charcot-Marie Tooth disease or poliomyelitis, often includes weakness of the calf muscles and foot dorsiflexors. As a consequence of calf muscle weakness, the patient’s gait is usually characterized by excessive ankle dorsiflexion and persistent knee flexion during stance (1, 2). Furthermore, ankle push-off is reduced (2). This results in an increased risk of falls (3), higher walking energy cost (4, 5) and diminished walking speed (4, 6, 7), limiting walking ability and activity in daily life (8).
Ankle-foot orthoses (AFOs) are provided to improve gait in lower leg muscle weakness (9–11). In addition to lifting the foot in swing, the AFO should aim to compensate for calf muscle weakness by restricting ankle dorsiflexion, thereby enabling an external dorsiflexion moment around the ankle (10, 11). Reducing ankle dorsiflexion also reduces the external knee flexion moment, thereby alleviating quadriceps muscular overload (4, 10). By restoring these gait deviations, AFOs can increase walking speed and reduce energy cost. In current orthotic practice in the Netherlands, a variety of AFOs for lower leg non-spastic muscle weakness are applied, ranging from off-the-shelf to custom-made AFOs (12) and high shaft reinforced orthopaedic shoes (OS) (13, 14). However, some studies evaluating AFOs/OS in persons with non-spastic muscle weakness have revealed a lack of improvements in walking speed (6, 12, 15, 16), energy cost (4) and gait biomechanics (4, 12, 17).
Differences in orthotic properties, such as ankle and footplate stiffness, footplate length and mass, may explain the variation in effectiveness (15, 18). Although, these mechanical properties have been evaluated in small clinical studies of patients with lower limb salvage (19), stroke (20, 21) and cerebral palsy (22), the few studies evaluating AFOs in non-spastic neuromuscular disorders did not specify the mechanical properties of the investigated AFOs (12, 23). Consequently, there is a lack of evidence-based guidelines to select the most effective AFO to improve gait in this population, and choices in current practice are based on the preferences of the prescribing physician or orthotist (12).
We hypothesize that, in current practice, this results in the provision of AFOs that are mechanically suboptimally matched to the patient and consequently vary in effects on gait. Providing a detailed overview of the mechanical properties and effects of the different AFOs provided to persons with non-spastic calf muscle weakness will establish a baseline against which the effect of optimization of AFO properties can be measured. This will guide further research aiming to provide evidence for improved provision of orthotics, as recommended in recent reviews (12, 23).
The aim of this study is to describe the orthotic properties and effects of AFOs provided in current practice to persons with non-spastic calf muscle weakness due to neuromuscular disorders, compared with shoes-only. Secondly, this study aimed to evaluate the effects of the various types of AFO and their orthotic properties on walking speed, walking energy cost and gait biomechanics.
Study design and setting
Cross-sectional data used in this study originate from the baseline visits of the PROOF-AFO trial (24). Data used are: orthotic properties, walking speed, walking energy cost, gait biomechanics and lower limb muscle strength. The PROOF-AFO trial (NTR 5170) was approved by the medical ethics committee of the Academic Medical Center in Amsterdam, The Netherlands.
Study population
Participants were recruited in hospitals and rehabilitation centres throughout the Netherlands between July 2015 and July 2017. Eligible persons were invited for a screening visit in which written informed consent was given and a rehabilitation physician checked the inclusion criteria. The inclusion criteria were: (i) diagnosed with a neuromuscular disorder; (ii) presence of non-spastic calf muscle weakness (unilateral or bilateral), defined as a score below grade 5 on the manually assessed Medical Research Council (MRC) scale (25) or unable to perform 3 heel rises (toe-standing) while standing on one leg; (iii) using an AFO/AFOs that enclosed the shank above the malleoli or using reinforced high shaft orthopaedic shoes (OS) provided for walking problems due to lower limb muscle weakness; and (iv) able to walk for at least 6 min with and without AFO/OS, if necessary with an assistive device, such as canes, crutches or walkers. Patients were excluded in case of quadriceps weakness for which a knee-ankle-foot orthosis was indicated or in case of severe foot deformities that could not be fitted into a regular AFO.
For this study, a convenience sample was used. The sample consisted of all participants of the PROOF-AFO trial (24). The sample size of the PROOF-AFO trial was calculated to demonstrate a 10% reduction in walking energy cost with a new stiffness-optimized AFO compared with a general prescribed AFO.
Measurements
Orthotic properties. The following orthotic properties were assessed: AFO type, whether the AFO was custom-made or off-the-shelf, mass, material, ankle stiffness, footplate stiffness, footplate length and dorsiflexion stop (DF-stop) angle of the ankle hinge if applicable.
AFO type and material were classified according to one of the following subgroups indicated by van der Wilk et al. (12): reinforced high shaft OS, ventral shell AFOs with no hinge, dorsal leaf AFOs with no hinge, hinged AFOs with a dorsiflexion stop (DF-stop AFO) and circular AFOs, which have no hinge and entirely enclose the ankle.
Ankle and footplate stiffness were measured with the Bi-articular Reciprocal Universal Compliance Estimator (BRUCE, Amsterdam, The Netherlands), which was designed specifically to measure AFO ankle and footplate stiffness (26). For stiffness measurements, the AFO was attached to a dummy leg. The metatarsal bending line of the AFO footplate was aligned with the metatarsal joints of the dummy foot and with the fulcrum of the BRUCE footplate. The BRUCE continuously measures the ankle and footplate angle and the moments exerted on the device. By manually pushing the BRUCE footplate towards dorsiflexion, a force was applied to flex the AFO footplate at the metatarsal bending line to approximately 30° of flexion (26). This was repeated 3 times and the footplate stiffness was defined as the linear slope between toe angle and recorded moment. The ankle stiffness was determined by manually pushing the AFO towards dorsiflexion and calculated by fitting a linear curve of the angle-moment relationship (26, 27). Ankle stiffness was measured only for non-articulated AFOs.
The angle of the DF-stop was calculated based on three-dimensional (3D) gait analysis data. The dorsiflexion angle at initial contact was subtracted from the maximal dorsiflexion angle in terminal stance. It was assumed that the hinge was in its neutral position at initial contact and at maximal dorsiflexion during terminal stance.
Walking speed and energy cost. For both shoes-only and the AFO/OS condition, walking speed and walking energy cost were assessed during a 6-min walk test with simultaneous breath-by-breath assessment of VO2 and VCO2 (Cosmed K4B2, Rome, Italy) on a 35-m oval track, which has been shown a reliable method in neuromuscular disorders (5, 28). If necessary, the use of customary assistive devices (e.g. canes, walker) was allowed. For convenience, the AFO/OS condition was tested first, with at least 10 min rest, or more if needed to recover, before the shoes-only condition started.
Gait biomechanics. Gait biomechanics were assessed using 3D gait analysis for walking over-ground with shoes-only and walking with the AFO/OS. Data were acquired using an 8-camera Vicon MX 1.3 system (100 Hz, Vicon, Oxford, UK) and 2 force plates (1,000 Hz, OR6-7, AMTI, Watertown, MA, USA). As the force plates were in series in the sagittal plane, the ground reaction forces of both legs could be recorded during one trial. Markers were placed according to the Plug In Gait (PIG) model (29). Three trials at self-selected comfortable walking speed in which each foot landed completely on one force plate, meaning that a full step for both legs was recorded, were analysed. To record 3 successful trials, approximately 10 trials were necessary.
Lower limb muscle strength. Muscle strength of both legs was manually assessed by a trained physician according to the MRC scale for hip abduction, hip adduction, hip flexion, hip extension, knee flexion, knee extension, plantar flexion and dorsiflexion (25). The scores of these 8 muscles were summed to calculate a composite muscle strength score for each leg, the MRC sum score (range 0–40) (30).
In addition, maximal isometric strength for the plantar flexors was assessed with a fixed dynamometer (Biodex Corp., Shirley, NY, USA). Subjects were positioned with their ankle in 15° plantarflexion, their shank horizontally, and the back of the chair at a 70° angle. Three maximal 5-s voluntary contractions (MVCs) were recorded, with 30-s rest in between. The highest recorded peak value (in Nm) was used for analysis.
Data analysis
Walking speed and walking energy cost. Walking speed (in m/s) and walking energy cost (in J/kg/m) were calculated over a steady-state period of at least 60 s within the last 3 min of the walk test. Steady state for VO2, VCO2 and walking speed was determined visibly. Mean steady state VO2, VCO2 and walking speed values were then used to calculate the gross walking energy cost according to: ((4.940* (VCO2/VO2) +16.040)*VO2)/walking speed). Energy cost was scaled to body mass including clothes and shoes.
Gait biomechanics. For each of the shoes-only and AFO/OS condition, 3 trials were analysed. Using the ground reaction force data, the moment of heel-contact and toe-off were determined. Trials were time-normalized and averaged using a custom-written Matlab script (version 2015, MathWorks, Natick, MA, USA). Subsequently, the following biomechanical parameters were determined: maximal ankle dorsiflexion during stance, maximal external ankle dorsiflexion moment, peak ankle power, minimal knee angle and maximal external knee extension moment during stance, which are considered relevant for the evaluation of AFOs in calf muscle weakness (3, 9, 31).
Statistical analysis
To describe participants (sociodemographic and clinical characteristics) frequencies are used to describe categorical outcomes and means and standard deviation (SD) for continuous, normal distributed outcomes. Orthotic properties, e.g. stiffness, are reported similarly. In the case of bilaterally affected persons, the orthotic properties of both AFOs were included in the analysis. Legs on which the AFO was worn were considered affected legs; in case AFOs were worn bilaterally both legs were considered affected. Differences in sociodemographic and clinical characteristics between users of different AFO types were tested with a 1-way ANOVA. To test for differences in orthotic properties between AFO types, a Kruskal–Wallis test was used due to the small number of subjects. The relationship between calf muscle strength in the affected leg (in Nm) and leg muscle strength (MRC sum score) for the affected legs with AFO ankle stiffness, considered a biomechanically important orthotic property (32), was tested using Spearman’s correlations because the data were not normally distributed.
Differences in walking speed and energy cost between walking with the AFO/OS and shoes-only were analysed with paired t-tests for all AFO types together and for the AFO types separately (SPSS for Windows (version 24)). The effect sizes of the AFO/OS on walking speed and energy cost were calculated for each individual. If the effect size was larger than the reported smallest detectable change (SDC), the AFO/OS was considered effective or detrimental, respectively. To be considered effective in increasing walking speed, the AFO should increase speed by at least 0.12 m/s, while for energy cost a reduction of at least 0.45 J/kg/m should be achieved (5).
Differences in gait biomechanics between AFO/OS and shoes-only were analysed with a multilevel mixed model using MLwiN 2.34 (Institute of Education, University of London, London, UK). This method was used to take into account: (i) the dependency between the 2 legs, if the person used AFOs bilaterally, and (ii) the influence of walking speed. Data were nested at 3 levels, namely; person (third level), leg (second level) and condition (first level). To model differences in baseline value (i.e. the value for walking with shoes-only) between participants, a random intercept was included. In addition, a random slope was included to model differences in effect of the AFO between participants. Both significantly improved the ˗2loglikelihood and therefore the model. To take into account the difference in walking speed between walking with and without AFO, walking speed was added as a fixed factor. Effects on the gait biomechanics of the different AFO types were tested separately using the same model. For all analyses, the significance was set at p = 0.05.
The effect of AFO ankle stiffness on gait outcomes was tested for ventral and dorsal leaf AFOs only, as the working mechanism of these AFO to restrain the ankle angle depends primarily on ankle stiffness (12). To test the effect of ankle stiffness on walking energy cost and speed, Spearman’s correlations were used, as AFO ankle stiffness was not normally distributed. In case of bilateral weakness, the mean AFO stiffness of the 2 legs was taken. To test the effect of ankle stiffness on gait biomechanics, a mixed modelling with a random intercept was used, in which the effect of AFO stiffness was modelled as a fixed effect. To take into account the effect of walking speed, this variable was also included as a fixed effect.
Subject characteristics
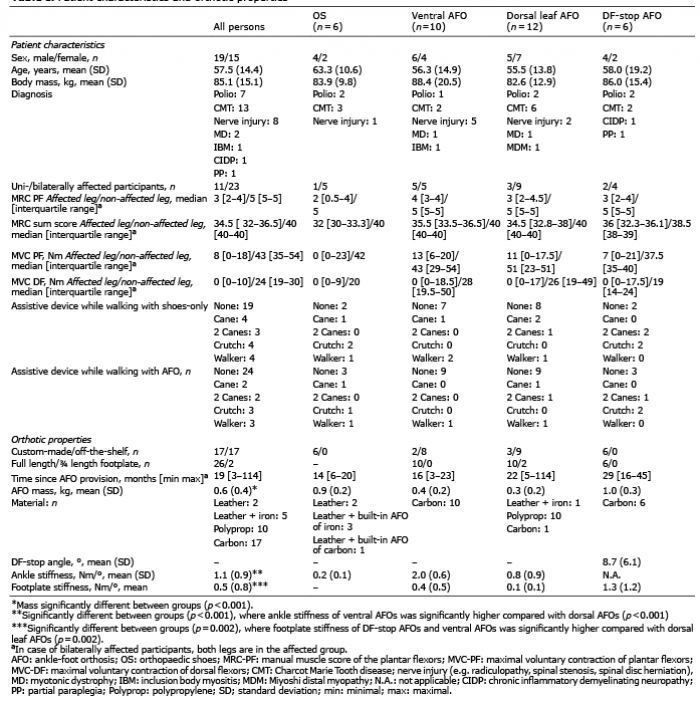
A total of 41 eligible persons were invited to participate in the PROOF-AFO trial. Of these, 34 persons from 12 hospitals and rehabilitation centres throughout the Netherlands met the inclusion criteria. Reasons for exclusion were: inability to walk without an AFO (n = 4), not wearing/using an AFO or shaft-reinforced OS (n = 2), or presence of severe knee extensor weakness (n = 1). Participants’ characteristics are presented in Table I (19 males; mean (SD) age: 57.5 (14.4) years)).
In total, 6 persons wore OS (5 bilateral), 10 wore a ventral AFO (5 bilateral), 12 a dorsal leaf AFO (9 bilateral) and 6 a DF-stop AFO (4 bilateral). None of the persons wore circular AFOs. All bilaterally affected persons wore the same AFO on both legs. There were no significant differences between AFO type subgroups on sociodemographic and clinical characteristics (p > 0.098). Fifteen persons used an assistive device when walking with shoes-only (cane: 4 patients, 2 canes: 3, crutches: 4, walker: 4) and 10 persons when walking with the AFO (cane: 2 patients, 2 canes: 2, crutches: 3, walker: 3).
Orthotic properties
Half of the AFOs/OS were custom-made, half were off the shelf and most were made out of carbon (n = 17) or polypropylene (n = 10). Mass differed significantly between the AFO types (range 0.3–1.0 kg, p < 0.001) (see Table I). Properites and effect of indiviual AFOs are presented in Appendix SI1
Table I. Patient characteristics and orthotic properties
Ankle stiffness was measured for 21 AFOs/OS. Stiffness was not measured for 4 OS as they did not fit in the BRUCE, for 2 ventral AFOs due to logistic issues as the BRUCE was located in another department, and for 1 ventral AFO and the DF-stop AFOs (when at the DF-stop) as these AFOs were completely rigid. Ventral AFOs (n = 7) were significantly stiffer than dorsal AFOs (n = 12) (p < 0.001). Footplate stiffness differed significantly between AFO types (p < 0.001); both DF-stop AFOs (p = 0.004) and ventral AFOs (p = 0.002) had stiffer footplates than dorsal AFOs (see Table I). Indiviudal AFO properties can be found in the Appendix SI1
No correlation was found between calf muscle strength (n = 21, r = 0.120, p = 0.603) or leg muscle strength (r = 0.221, p = 0.349) and AFO ankle stiffness (Fig. 1).
Fig. 1. Ankle-foot orthosis (AFO) ankle stiffness vs affected leg muscle strength. No correlation was found between leg muscle strength and AFO ankle stiffness, indicating that this characteristic is not taken into account when providing an AFO in clinical practice. If persons were bilaterally affected, the mean muscle strength and AFO ankle stiffness was plotted. OS: orthopaedic shoes ; MVC: maximal voluntary contraction; MRC: manual muscle score.
Walking speed and walking energy cost
Between the walking test with the AFO/OS and the test with shoes-only, 2 participants needed more than 10 min rest, but neither exceeded 15 min. When using an AFO/OS walking speed increased by a mean of 0.18 m/s (95% CI 0.13–0.23) (20%) from 0.86 m/s (SD 0.21) to 1.04 m/s (SD 0.21), while walking energy cost decreased by 0.70 J/kg/m (95% CI –0.94 to 0.48) (–13%) from 5.26 J/kg/m (SD 1.13) to 4.55 J/kg/m (SD 0.85) with AFO/OS (healthy reference value 3.30 J/kg/m).
When evaluating the effect size of wearers of different AFO types, walking speed increased most in ventral AFO users (n = 10, by 0.23 m/s (95% CI 0.10–0.36) from 0.86 (SD 0.21) to 1.09 m/s (SD 0.18), followed by OS users (n = 6, by +0.19 m/s (95% CI 0.08–0.31) from 0.75 (SD 0.29) to 0.94 m/s (SD 0.32) and DF-stop AFOs users (n = 6, by 0.18 m/s (95% CI –0.01 to 0.37) from 0.76 (SD 0.11) to 0.94 m/s (SD 0.21), while least improvement was found in users with dorsal leaf AFOs (n = 12, by 0.14 m/s (95% CI 0.07–0.21) from 0.96 (SD 0.18) to 1.10 m/s (SD 0.14). Walking energy cost reduced most in persons wearing DF-stop AFOs (n = , by –1.10 J/kg/m (95% CI –1.84 to –0.36) from 5.97 (SD 1.46) to 4.87 J/kg/m (SD 1.33)), OS (n = 6, by –0.93 J/kg/m (95% CI –1.72 to –0.13) from 5.77 (SD 1.39) to 4.83 J/kg/m (SD 0.85)) and ventral AFOs (n = 10, by –0.68 J/kg/m (95% CI –1.06 to –0.28) from 5.03 (SD 0.82) to 4.35 J/kg/m (SD 0.80), while a smaller and non-significant effect was found for users with dorsal leaf AFOs (n = 12, –0.41 J/kg/m (95% CI –0.82 to 0.01) from 4.83 (SD 0.88) to 4.42 J/kg/m (SD 0.62) (see Fig. 2).
Compared with the shoes-only condition, the AFO/OS improved both energy cost and walking speed above the SDC for 16 (47%) persons. Only energy cost improved for 5 (15%) persons (using 1 ventral, 2 dorsal and 2 DF-stop AFOs) and only walking speed for 5 others (15%) (using 1 OS, 1 ventral and 3 dorsal AFOs). Finally, 8 (24%) persons saw no improvements in energy cost or walking speed (using 1 OS, 3 ventral, 3 dorsal and 1 DF-stop AFO). The effect of the AFO for each individual can be found in the Appendix SI1
Correlation analysis showed that, with an increase in AFO ankle stiffness, the walking energy cost reduced (r = –0.510, p = 0.031), while no effect on walking speed was found (r = 0.264, p = 0.290).
Gait biomechanics
Among the 34 included patients, walking with AFOs/OS reduced the maximal ankle dorsiflexion angle by a mean of 3.0° (95% CI 1.3–4.7) and increased the maximal external ankle dorsiflexion moment by a mean of 0.18 Nm/kg (95% CI 0.09–0.27) compared with shoes-only (p < 0.001). On peak ankle power, there was no significant effect of using an AFO/OS (—0.11 W/kg (95% CI –0.34 to 0.12)). The minimal knee angle during stance was reduced significantly, by 2.2° (95% CI –4.5 to 0.0), and the maximal external knee extension moment increased significantly, by 0.09 Nm (95% CI 0.02–0.16), when using the AFO/OS (Table II).
Table II. Effect of the ankle-foot orthoses (AFOs) on gait biomechanics: results of the mixed model analyses
The effects of the different AFO types are shown in Figs 3 and 4 and Table III. Maximal ankle dorsiflexion angle reduced substantially in ventral AFO users and DF-stop AFO users, while in OS users and dorsal AFO users a smaller effect was found. On ankle moment, DF-stop AFOs showed the largest improvement. Ventral AFOs and OS also showed increases, while dorsal AFOs did not. Although none of the AFO users showed a significant change in peak ankle power, it is noteworthy that a slight increase in peak ankle power was found in ventral AFO users only (+0.08 W/kg; SD 0.20).
Fig. 2. Mean effect of the ankle-foot orthosis/orthopaedic shoes (AFO/OS) (black bars) compared with shoes-only (grey bars) on walking speed and energy cost (left-hand panels) and on individual level (right-hand panels). Effects are presented for the whole group and per AFO type. In the right-hand panels, the black solid line represents no effect. The dashed line represents an improvement or deterioration with the smallest detectable change of 0.12 m/s for walking speed and 0.45 J/kg/m for walking energy cost. In the walking energy cost graph, a symbol below the solid line means that walking energy cost is reduced (improved) when wearing the AFO. In the walking speed graph, a symbol above the solid line means that walking speed increased (improved) when wearing the AFO. DF-stop: dorsiflexion stop.
Fig. 3. Mean gait biomechanics for walking with shoes-only and with the ankle-foot orthosis/orthopaedic shoes (AFO/OS) for the different types of ankle-foot orthoses (AFO). The figure indicates that the effect of the dorsal AFOs and OS on gait biomechanics is smaller than the ventral AFOs and DF-stop AFOs. DF: dorsiflexion.
Table III. Effect sizes of the different ankle-foot orthosis (AFO) types on walking energy cost, speed and gait biomechanics
With regard to the knee, the minimal knee angle reduced most in persons wearing DF-stop AFOs, and tended to reduce in OS users, while smaller effects were found for persons wearing the other AFO types. The maximal external knee extension moment in late stance was most enlarged in persons wearing DF-stop AFOs, ventral AFOs and OS, while no effect of dorsal AFOs was found.
AFO ankle stiffness decreased the maximal ankle dorsiflexion angle by 2.5° with an increase of 1 Nm/° (95% CI –4.1 to –0.7). No effects were found on maximal ankle moment (+0.04 Nm, 95% CI 0.16 to –0.08), peak ankle power (–0.07 W/kg, 95% CI –0.35 to 0.21), minimal knee angle (–1.2°, 95% CI –3.6 to 1.2) or external knee extension moment (–0.02 Nm, 95% CI –0.11 to 0.07).
Fig. 4. Individual effects of the ankle-foot orthosis (AFO) on maximal ankle dorsiflexion angle, maximal external dorsiflexion moment, knee angle and maximal external knee moment during stance. OS: orthopaedic shoe; DF: dorsiflexion; Nm/kg: Newton*metre per kg.
The sample of 34 persons with neuromuscular disorders exhibiting non-spastic calf muscle weakness in this study were provided with a variety of orthotic devices that differed largely in mass, material, and ankle and footplate stiffness. The differences in or-thotic properties were not explained by differences in patient characteristics. On average, the provided AFOs/OS were effective in improving walking speed, energy cost, and ankle and knee biomechanics, but large inter-individual and inter-AFO type differences were found. Persons using ventral AFOs and DF-stop AFOs showed larger beneficial effects in gait biomechanics compared with OS and dorsal AFOs, which is, at least partly, explained by the lower AFO ankle stiffness of OS and dorsal AFOs.
Only 20% of subjects in this study used a dorsal leaf AFO or DF-stop AFO made of carbon, which are the AFOs recommended for non-spastic calf muscle weakness by a recent Dutch guideline (10). The other persons used different AFO types with a variety of mechanical properties, which could be due to specific patient wishes or to differences in preferences of clinicians and orthotists. The mean effects of the provided AFOs/OS on walking speed (+19.5%) and energy cost (–13.5%) were larger compared with previous studies in unilaterally affected polio patients with non-spastic calf muscle weakness reporting a 8% increase in speed and 7% reduction in energy cost (4). It is likely that the inclusion of bilaterally affected persons and persons with very little remaining calf muscle strength increased the effect of the AFOs in our study, as demonstrated in patients with Charcot-Marie-Tooth disease (33). Nevertheless, in more than 50% of subjects, the AFOs were ineffective in improving walking speed and/or energy cost, while there was potential for functional gain. This is a comparable percentage of non-responders to the AFO as found in children with cerebral palsy (34). Although it is uncertain whether another type of AFO (i.e. with different mechanical properties) would improve the functional outcomes in our subjects, we hypothesize that at least a proportion of the non-responders is due to an inadequate match between the AFO ankle stiffness and the patient’s impairments. An increase in ankle stiffness was shown to restrain the ankle angle more and is correlated with a larger reduction in energy cost. A higher stiffness would therefore be most beneficial for more severely affected persons, as these patients experience the most excessive ankle dorsiflexion and a more elevated energy cost. However, we did not find a correlation between AFO ankle stiffness and calf muscle strength, suggesting that in usual care the AFO mechanical properties may be suboptimally matched to the patients’ impairments.
Similarly, inadequate AFO ankle stiffness could explain the smaller effects on maximal ankle angle mainly found in OS and dorsal AFOs users. To effectively alter the ankle angle, substantial ankle stiffness is needed to restrain the uncontrolled forward rotation of the tibia in the sagittal plane during stance, as typically seen in persons with non-spastic calf muscle weakness (19, 21, 35). Furthermore, higher footplate stiffness helps to move the origin of the ground reaction force forward underneath the foot during stance (36, 37), which would increase the external ankle and knee moment. We argue that the stiffness of the ankle and footplate of OS and dorsal AFOs were generally too low in our sample, as a high percentage of users showed little effect on the gait biomechanics compared with ventral and DF-stop AFOs users (see Fig. 4). Differences in these properties can also explain the lack of effect on walking energy cost in users of dorsal AFOs, as ankle stiffness was found to be correlated with the AFOs’ effect on energy cost.
The largest effect sizes on walking speed and energy cost were seen in ventral AFO and DF-stop AFO users, showing substantial effects on ankle and knee moments. Dorsal AFO users showed considerably less effect on walking speed and energy cost, which coincides with small effects on joint moments. We acknowledge that dorsal AFO users had a better walking performance without the AFO, but when walking with an AFO the gait biomechanics were considerably more normalized in ventral AFO and DF-stop AFO users (Figs 3 and 4). This suggests that the mechanical properties of dorsal AFOs were insufficiently matched to the specific muscle function deficits to meaningfully affect the gait biomechanics.
However, a rule such as “the stiffer the better” does not hold, since in persons using OS substantial effects on energy cost and speed were found despite a low ankle stiffness. It is probable that this is caused by a better foot clearance in swing, as can be seen in Fig. 3, or by the rocker-profile of the shoe, which was the case in most OS. However, the OS did not seem to support the calf muscles as well during stance as ventral and DF-stop AFOs, since OS users still avoid a large external ankle dorsiflexion moment. This lack of support for the calf muscles seems to induce a stiff-knee gait pattern, as the maximal knee flexion angle in loading response was reduced when using the OS, which was not seen in the other AFO types (Fig. 4). Apparently, this stiff-knee gait pattern is efficient in improving the ankle and knee moment, but in the longer term it may induce knee injuries (38).
The AFOs/OS provided did not increase peak ankle power on average, which is due to the restriction of ankle movement, i.e. limiting plantarflexion motion (3, 39). Potentially, supporting the ankle power could further improve walking speed and energy cost (40). In this regard, it is noteworthy that ventral AFO users, despite the relatively high stiffness, slightly increased peak ankle power. The design and material (carbon) provide these AFOs with spring-like capabilities, which can support the push-off by releasing energy that was stored in midstance. However, the ability of spring-like AFOs to effectively support the push-off depends on their ankle stiffness (18). In patients the interaction between AFO ankle stiffness and muscle function is difficult to predict, which calls for a prospective study to systematically evaluate the effect of the stiffness of different AFO in patients with calf muscle weakness.
Strengths and limitations
This study is the first to provide a detailed overview of the orthotic properties and effects of multiple AFO types provided in usual care to people with non-spastic neuromuscular disorders. Previous AFO studies lacked information about specific orthotic properties (12, 23). Although our sample size is one of the largest so far evaluating AFOs in neuromuscular disorders, the heterogeneity in AFO types resulted in small subgroups.
A major limitation of this study is that it did not compare different AFO types within subjects. As such, the effect sizes across AFOs cannot be attributed directly to differences in mechanical AFO properties, because they will also be affected by differences in baseline gait patterns between patients (1). In addition, the measured AFO properties might have been affected by the long usage time of some AFOs and consequent wear of the material. Thus, this observational study does not allow us to draw firm conclusions about which AFO is most beneficial for persons with non-spastic calf muscle weakness. Future research should explore prospectively how orthotic properties, especially AFO ankle stiffness, affect gait biomechanics, walking speed and energy cost, in order to provide evidence for optimal orthotic treatment in patients with calf muscle weakness.
Conclusion
In conclusion, in usual orthotic care in the Netherlands AFOs, as well as shaft-reinforced OS, which vary greatly in orthotic properties, are provided to persons with non-spastic calf muscle weakness. The effects of the AFOs/OS provided coincide with differences in mechanical properties and are highly variable with regard to increasing walking speed, reducing walking energy cost and improving ankle dorsiflexion angle and external knee moment. In dorsal and ventral AFO users, larger reductions in walking energy cost and maximal ankle angle are related to greater ankle stiffness, indicating the importance of optimizing this AFO property. Prospective research, which systematically evaluates the effect of AFO properties, is needed to establish evidence-based AFO prescription for persons with calf muscle weakness.
This work was supported by the Prinses Beatrix Spierfonds (grant number W.OR 14-21).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize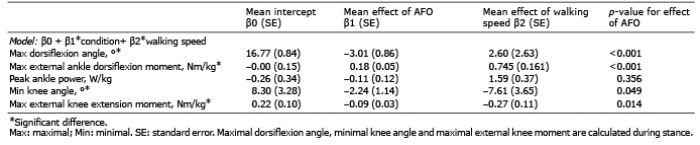 Click to show fullsize
Click to show fullsize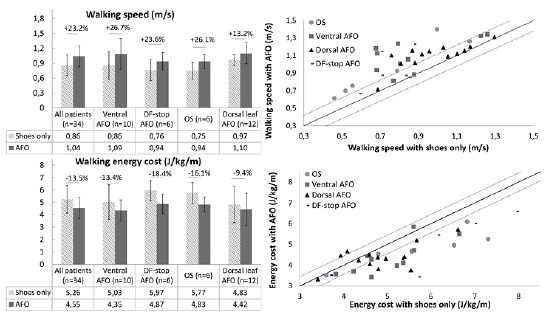 Click to show fullsize
Click to show fullsize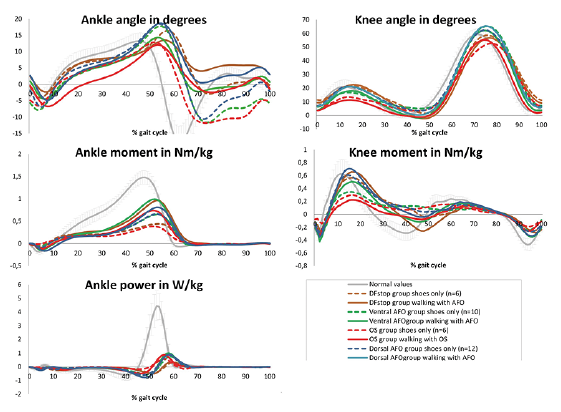 Click to show fullsize
Click to show fullsize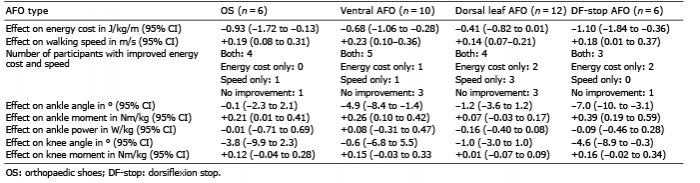 Click to show fullsize
Click to show fullsize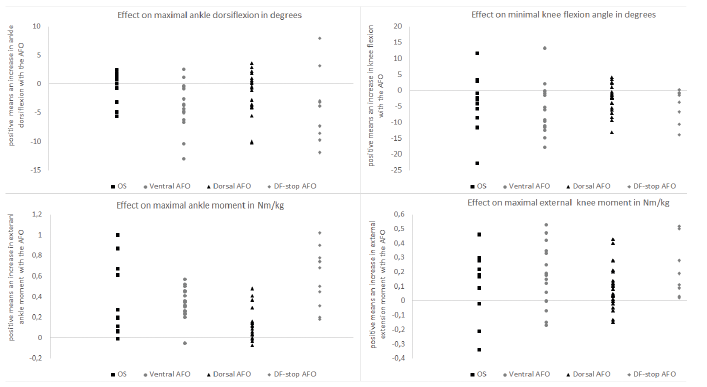 Click to show fullsize
Click to show fullsize