
From the 1Department of Rehabilitation Medicine and 2Department of Oral and Maxillofacial Surgery, University Medical Center Groningen, University of Groningen, Groningen, and 3Roessingh Center for Rehabilitation, Enschede, The Netherlands
Objective: To report the rates of persons returning home within one year following dysvascular major amputation of the lower limb in the Netherlands, and to identify factors associated with returning home directly after hospital admission and after discharge to care facilities.
Design: Retrospective cohort study.
Patients: Dysvascular major amputation of the lower limb, n = 382, mean age 71.9 years (standard deviation (SD) 12.5 years), 65% male.
Methods: Medical records of all persons undergoing major amputation of the lower limb in 2012–2013 in 12 hospitals in Northern Netherlands were reviewed. Odds ratios (OR) were calculated using multivariate logistic regression.
Results: Among persons admitted from home and surviving the hospital admission, 21% returned home, with higher odds of returning home being associated with living with a partner (OR = 2.8, p = 0.006) and younger age (< 65 years). Among those discharged to care and surviving the first year, 77% returned home within one year after amputation, with higher odds being associated with younger age (<75 years) and admission to inpatient rehabilitation (OR = 10.6, p = 0.004) or geriatric rehabilitation in skilled nursing facilities (OR = 3.5, p = 0.030).
Conclusion: Four out of 5 persons surviving dysvascular major amputation of the lower limb return home within one year, although a majority requires care in either inpatient rehabilitation or a skilled nursing facilities setting.
Key words: amputation; skilled nursing facility; rehabilitation centre; frail elderly.
Accepted Nov 19, 2019; Epub ahead of print Nov 22, 2019
J Rehabil Med 2020; 52: jrm00008
Correspondence address: Behrouz Fard, University Medical Center Groningen, Department of Rehabilitation Medicine, Internal Post Code CB40, PO Box 30.001, NL-9700 RB Groningen, The Netherlands. E-mail: b.fard@umcg.nl
Persons undergoing lower limb amputation due to vascular disease and/or diabetes mellitus are typically elderly and medically frail. Most are admitted from home, and approximately one-fifth return home after hospital admission for amputation surgery, especially those with a partner and younger than 65 years. Among those who are unable to return home in the first instance, eventually nearly 4 out of 5 return to independent living within one year after amputation. It should be borne in mind, however, that one-third of persons does not survive up to one year after amputation and that the aforementioned number of people returning home applies only to those who survive the first year. The healthcare system in the Netherlands provides dedicated rehabilitation programmes for elderly patients, with lower intensity training compared with traditional inpatient rehabilitation programmes. In this study, ”geriatric rehabilitation” seemed effective in terms of improving the chances of persons’ return to home after a dysvascular major amputation of the lower limb.
Over 90% of lower limb amputations (LLA) in Western European countries are secondary to peripheral arterial disease (PAD) and diabetes mellitus (DM) (1), and may be referred to as “dysvascular” amputations. LLA are categorized as minor or major, the latter defined as amputation through the ankle joint and more proximal levels (2–5). Major LLA are associated with more disability (6) and higher mortality rates (3) compared with minor LLA. On average, 47% (5) of patients do not survive the first year after major LLA, although the reported 1-year mortality ranges widely (16–48%) (5). A majority of persons with LLA live independently at home prior to amputation (7–9). Successful rehabilitation may be defined as regaining ambulation and/or prosthesis use (7, 10–13). However, being able to return home is also an important goal for patients, their families and healthcare professionals (9, 14, 15), even more so considering the limited life expectancy of persons undergoing amputation (16). Resumption of independent living directly after hospital admission for LLA is often not feasible, and patients are discharged to inpatient care facilities (17, 18). Traditionally, high-intensity treatment for persons undergoing amputation has been provided in inpatient rehabilitation centres. Considering the typically older age of patients undergoing dysvascular LLA (19) and high comorbidity rates (20), skilled nursing facilities (SNF) have increased in numbers in recent decades in order to accommodate this population (14, 15).
Current research on the effectiveness of SNFs is conflicting to a large extent: several studies have reported that more comprehensive rehabilitation programmes are associated with better survival (11, 21, 22) and functional outcomes (11, 18, 21, 23), while others did not find these differences (12, 24) and observed benefits of rehabilitation programmes offered in SNFs (14). To our knowledge, few studies have focused specifically on analysing return home among persons undergoing dysvascular LLA, taking into account factors such as mortality rates at different stages and the patient’s eventual residential situation (9, 22). Most prior research has focused on populations from a single (rehabilitation) centre (7, 8, 25), hospitals for military veterans (13, 18, 23) or SNFs only (14, 26), and has excluded patients with prior LLA (9, 12, 27) or bilateral/proximal level of LLA (24, 28, 29) or included those with traumatic aetiology (12, 22, 23), which may be regarded as a separate population that typically includes younger patients, with a lower incidence of comorbidity and higher life expectancy (30).
The aim of the present study is to report the rates of persons returning home within the first year following dysvascular major LLA in the Netherlands, and to identify factors associated with returning home directly after hospital admission and after being discharged to care facilities. The results will provide insight into the path-ways of care for these patients, for surgeons, Physical and Rehabilitation Medicine (PRM) specialists and geriatric specialists involved in the multidisciplinary treatment of persons undergoing dysvascular amputation, who constitute a small, but frail, population.
Setting and population
Data for all major LLA performed from 1 January 2012
through 31 December 2013 in the 3 northern provinces of the Netherlands were examined for eligibility. Data collection was performed in 12 hospitals (11 general hospitals and 1 university hospital) from 1 January 2015 to 1 April 2017, for which patients’ medical records were accessed directly. Prior to data collection, the study was approved by the regional Medical Ethics Committee (M15.176087), local Medical Ethics Committees of hospitals, and Board of Directors. Dysvascular LLA was defined as any major amputation (i.e. ankle disarticulation and more proximal) among patients with a recorded diagnosis of PAD and/or DM at the time of, or prior to, the amputation. Amputation due to trauma, cancer, complex regional pain syndrome type-1, iatrogenic complications, lymphoedema, fulminant infection in otherwise healthy adults, and congenital syndromes were excluded. No patients were excluded based on age. Additional information pertaining to the healthcare system in the Netherlands, differences in care facilities and the study population is provided in Appendix SI1 (section S1).
Variables
The outcomes were discharge directly to home following hospital admission and return home within one year, among persons surviving the first year after major LLA, as identified from their medical records. Data regarding age, sex, presence of comorbidities, vascular surgical history, including percutaneous transluminal angioplasty, arterial bypass grafting, endarterectomy and previous minor or major LLA, were also extracted from the medical records, specified for having been performed either ipsilateral, contralateral or bilateral to the side of first major LLA in the study period (i.e. the index amputation). For every amputation performed (both during and prior to the study period), aetiology, date, level and anatomical side were recorded. Because the aim of this study was to assess a functional outcome, anatomical levels of amputation were subsequently re-coded as either: “unilateral high” (knee disarticulation (KD) or transfemoral (TF) amputation), “’unilateral low”’ (transtibial (TT) amputation) or “bilateral” (TF, KD or TT). When multiple amputations had been performed on the ipsilateral or contralateral limb, either prior to or within the study period, the most proximal level was used to determine the level of amputation, since this may determine discharge destination due to level of ambulation. For example, TF performed within the study period and contralateral TT prior to the study resulted in the amputation level being coded as “bilateral”, whereas TT followed by an ipsilateral TF within the study period resulted in the amputation level being coded as “unilateral high”. A primary LLA was defined as no recorded history of any revascularization, minor or major LLA on the side of index amputation. Because social support has been reported to influence outcome after amputation (31), the status of patients living with a partner at the time of index amputation was recorded and analysed. Marital status was recorded (but is not presented), because many “unmarried” and “widowed” individuals have a life partner with whom they share a household, and marital status by itself provides insufficient information in assessing social support. Further details pertaining to data collection and variables are provided in Appendix SI1 (section S2).
Statistical analyses
Age as a potential predictor of the outcomes was analysed both as a continuous variable (presented in Appendix SI1, sections S3 and S4) and re-coded into age categories in order to facilitate clinical interpretation. Univariate associations between patient characteristics and the outcome variables were explored using χ2 tests. Variables with p < 0.2 were included in the multiple logistic regression analyses with backward stepwise elimination. Odds ratios (OR) with 95% confidence intervals (95% CI) were calculated for the identified associations between the predictor and outcome variables. For the main analyses, statistical significance was set at α = 0.05. Microsoft Excel 2016 and IBM SPSS Statistics 24 were used for analyses.
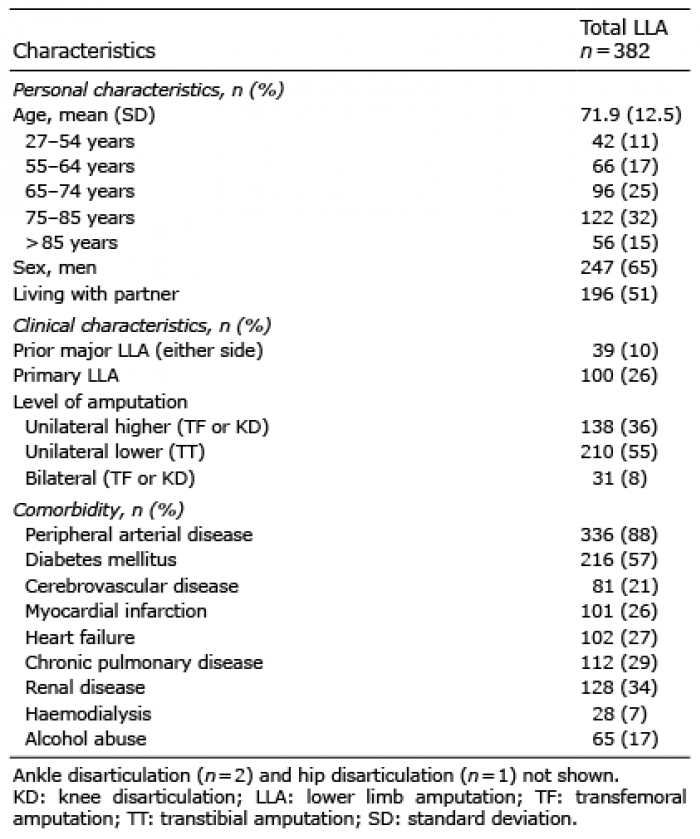
A total of 382 persons undergoing dysvascular major LLA in 2012 and 2013 were identified, of whom 65% were male (Table I). The mean age (standard deviation (SD)) at the time of index amputation was 71.9 years (SD 12.5 years), the youngest person was 27 and oldest 95 years old. The mean ages (SD) of persons discharged to home, inpatient rehabilitation, SNF and nursing home were, respectively, 62.3 (SD 11.9), 64.3 (SD 9.4), 73.7 (SD 11.0) and 77.6 years (SD 12.3). The clinical course after hospital admission showed a high level of complexity with regard to discharge destinations, mortality rates at different stages and eventual outcomes at one year after amputation (Fig. 1). The aim of the study being to report rates of return to independent living, persons already residing in nursing homes or residential care prior to amputation and those who died during hospital admission or after discharge were not classed as returning home (Fig 1), with the exception of one person who was admitted from a nursing home (which was a temporary admission unrelated to amputation) and who was observed to reside in independent living within one year of amputation.
Table I. Patients’ characteristics
Discharge to home following hospital admission
Among persons who were admitted from home and who had survived the hospital admission (n = 266), 56 (21%) returned home and 210 (79%) were discharged to either care in a nursing home, inpatient rehabilitation centre or SNF (Table II). Univariate and subsequent multivariate analyses of discharge to home are shown in Table II. Compared with those aged > 85 years, persons in the age categories 0–54 and 55–64 years had, respectively, 7.6 (p = 0.013) and 7.9 (p = 0.009) times higher odds of being discharged directly to home. The rates of discharge to home for persons aged 65–74, 75–84 and >85 years were similar. Independent of age, living with a partner at the time of hospital admission was associated with higher odds of being discharged to home (OR=2.8, 95% CI 1.3–5.7, p = 0.006).
Table II. Univariate and multivariate analyses of discharge to home following hospital admission for amputation
Return home within one year of amputation
Among persons who could not be discharged to home after hospital admission and who survived the first year after amputation (n = 158), 122 (77%) returned home within one year, whereas 36 (23%) did not (22 resided in a SNF, 11 in a nursing home and 3 were still admitted for inpatient rehabilitation) (Table III, Fig. 1). Univariate and subsequent multivariate analyses of return home within one year of the amputation are shown in Table III. Respectively, 50 out of 53 persons referred to inpatient rehabilitation, 64 out of 86 discharged to SNFs and 8 out of 19 discharged to nursing homes, returned home within one year. Compared with those aged > 85 years, ORs of returning home within one year were 11.5 (p = 0.013) for persons aged 0–54 years, 12.6 (p = 0.008) for those aged 55–64 years, and 6.9 (p = 0.007) for those aged 65–74 years. Compared with discharge to a nursing home after hospital admission, both inpatient rehabilitation and SNF were associated with higher odds of returning home within one year, with ORs of 10.6 (95% CI 2.2–52.3, p = 0.004) and 3.5 (95% CI 1.1–11.1, p = 0.030), respectively.
Table III. Univariate and multivariate analyses of return home within one year of amputation
Fig. 1. Pathways of care at admission, hospital discharge and 1 year after amputation. Eligible for return home directly after hospital admission: n = 382 excluding persons admitted from nursing home (n = 45), residential care (n = 33) and those who died in hospital (n = 38); and eligible for return home within one year: additionally, excluding persons discharged to residential care (n = 2), home (n = 56), those who returned home but died (n = 9) and those who died after discharge without returning home (n = 41). In total 130 (34%) persons died within one year after amputation: 49 during hospital admission and 81 after discharge. For 18 (5%) persons, outcome data were unavailable at one year after amputation. *Returned home, but died before one year after amputation.
The main findings of this study are that 21% of persons surviving hospital admission for dysvascular major LLA in the Netherlands are discharged home; and that, among those who cannot be discharged home directly and survive the first year, 77% return home within 1 year of amputation. In our study, 4 out of 5 persons undergoing major LLA were admitted from independent living at home, similar to previous studies (7–9, 22). Direct comparison of the outcomes with previous research is challenging, however, because of inherent differences in healthcare systems and study populations (e.g. inclusion of minor LLA and exclusion of patients with prior or bilateral LLA). Our finding that 21% of subjects were discharged home directly following hospitalization has been similarly reported in a study conducted in the USA (17), whereas other studies have observed approximately 50% of persons being discharged home following LLA (9, 21). These disparities may be explained, to some extent, by the inclusion of foot amputations (21) and patients with first-ever LLA after revascularization only (9). Previous studies report that between 42% and 84% (14, 22, 23, 26, 32) of persons eventually return home in the first year after amputation. The relatively large variation observed across studies is probably due to the aforementioned differences in healthcare systems, study samples and study designs.
Most previous research has focused solely on persons undergoing their first-ever LLA. These persons may be expected to have less severe vascular disease and to be in a better physical condition, compared with those who have undergone dysvascular amputation(s) in the past (3). We chose to include these persons in order to test the assumption that having undergone a major LLA in the past would predispose one to lower odds of returning home after major LLA. A small minority of persons (10%) in our study had a prior major LLA on either side, but they were no better or worse off than those undergoing their first LLA, in terms of returning home after hospitalization or within one year of amputation. There is an ongoing discussion in the literature as to whether persons undergoing major LLA after “failed” attempts of revascularization have worse clinical outcomes compared with those for whom the decision to amputate (i.e. “primary”) is reached earlier (10, 13, 33). In this study, one-quarter of subjects underwent primary LLA (i.e. no ipsilateral revascularization or minor/major LLA prior to the eventual major LLA), but this was not associated with different odds of returning home (10, 11, 13). Previous studies state that comorbidities, such as cerebrovascular disease (27, 34), (congestive) heart disease (5), chronic pulmonary disease (31, 34) and end-stage renal disease (9, 10, 27), are associated with poorer outcomes of survival, ambulation or prosthesis use. Therefore, we expected persons with these conditions to show lower rates of being able to return home, which was not the case in this study. Several authors note that persons with dysvascular amputation, especially the geriatric subpopulation, are medically frail and that multi-morbidity is common (5, 20). However, the extent of the role of different comorbidities on clinical outcomes, such as walking ability, remains unclear, as concluded by a systematic review (35). It is surprising that proximal or bilateral levels of amputation were not associated with less favourable odds of returning home directly after hospital admission or within 1 year, as distal and unilateral LLA have been found be to associated with better physical functional outcomes and prosthesis use in previous research (10, 13, 18, 26). However, a distal unilateral amputation might not be a requisite for achieving ambulation (with or without a prosthesis) (12, 35) at the level needed for returning to independent living.
Strengths and limitations
The main strength of this study is that by including persons from 12 hospitals it was possible to avoid selection bias to a large extent, as the population was not restricted only to persons from inpatient rehabilitation, geriatric or single hospital settings. Also, by analysing the clinical course from the time of amputation up to one year, this study was able to illustrate the intricacies of care pathways at different stages. A limitation is that difficulties were encountered in determining the cumulative length of hospital stay related to the amputation, because many persons had multiple admissions prior to and after the index amputation, some related to the amputation and others (potentially) not. Unfortunately, for most persons it was not possible to assess the pre-amputation cognitive, nutritional and ambulatory status based on hospital records. Because these factors have been reported as being predictive of functional outcomes after LLA by some studies (35), their omission in this study should be taken into account. The relatively small sample size may have contributed to limited power in the multivariate analyses. The medical ethical permissions only allowed storage of data relevant to the study population (i.e. dysvascular LLA), because of which it was not possible to provide specific details pertaining to excluded persons (i.e. LLA due to other causes). As extensively described previously, differences in incidence rates, mortality rates, patients characteristics and outcomes are reported between nations, as well as between regions in certain countries (5, 16, 36), we therefore caution generalizing the results of the current study to other countries. The design of the present study does not allow us to ascertain whether inpatient rehabilitation or treatment in SNFs is better in terms of functional outcomes. Although the age of persons receiving SNF care is considerably older than those in inpatient rehabilitation, a majority of persons discharged to SNFs were nonetheless able to return home within one year of amputation. Although analysis of survival rates was not within the scope of this study, it should be noted that the 1-year mortality rate was 34%, which is within the lower range of previously reported research (5), and that conclusions regarding return home should be prefaced by “among those who survived the amputation”.
Clinical implications
Our finding that relatively younger age and having a partner in the home situation are beneficial for the odds of persons returning directly to independent living (10, 17) are in line with clinical experience. Clinicians and researchers might assume that the extent of comorbidity determines whether patients require additional high- or low-intensity inpatient care before being able to resume independent living. However, no single comorbidity was identified as being predictive of odds of returning home. In the Netherlands, PRM specialists determine the indication for inpatient rehabilitation, for which they analyse the overall level of function and make an individual assessment of a person’s biological and psychosocial capacities. The association of admission to inpatient rehabilitation with considerably higher odds of return home compared with admission to a nursing home might therefore be regarded as a proxy of assessing a person’s overall functional status at the time of major LLA, in which factors such as comorbidity are nested. Some studies have suggested that treatment in SNF is associated with worse survival and functional outcomes compared with inpatient rehabilitation (11, 18, 21). However, systematic reviews of 1- and 5-year mortality rates did not identify the type of treatment facility as being associated with survival rates (5, 16). A person’s physical condition is expected to greatly influence whether they are able to adhere to high-intensity treatment in an inpatient rehabilitation setting. With this mind, it is likely that, in the aforementioned studies (11, 18, 21), persons with more deconditioning and more severe comorbidity were discharged to SNFs instead of inpatient rehabilitation, and that the poorer outcomes were not necessarily attributable to the SNF treatment alone. Interestingly, a systematic review concludes that there are likely benefits of geriatric rehabilitation programmes in general, in terms of mortality rates, discharge destinations and functional status (37). Similarly, a recent study of geriatric rehabilitation in the Netherlands stated that, between 2007 and 2015, the intensity of treatment in SNFs increased, while mortality rates decreased and rates of patients returning home improved significantly (38). The rationale behind this being that dedicated rehabilitation therapy and goal-oriented efforts in optimizing functional recovery are more likely to improve the physical condition and motor skills of the affected persons compared with traditional “rest and nursing” regimes in the geriatric population. Given this rationale, the results of the current study suggest that, within the Dutch healthcare system, dedicated geriatric rehabilitation may be effective in facilitating return to independent living among more elderly persons after major LLA, in conjunction with clinical rehabilitation provided for younger physically fitter persons. As we have observed in reviewing the contemporary literature, rehabilitation programmes tailored for elderly patients do not exist in many countries. The findings of the current study may provide incentive for future prospective research in the Netherlands and internationally, with more in-depth analysis of functional outcomes for elderly and non-elderly persons undergoing major LLA in different rehabilitation settings.
Conclusion
In the Netherlands, most persons undergoing major dysvascular LLA are admitted from independent living. Among those surviving the hospital admission, 21% are discharged directly to home, with higher rates being associated with younger age (<65 years) and having a partner at home. Among those who are unable to return home after hospital admission and who survive the first year, 77% return home within one year of amputation. For these persons, younger age (< 75 years) and care in either inpatient rehabilitation or SNF is associated with higher odds of eventually returning home. These results suggest that high-intensity inpatient rehabilitation for younger persons and low-intensity geriatric rehabilitation for elderly persons may be effective in optimizing the odds of return to independent living after major LLA.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize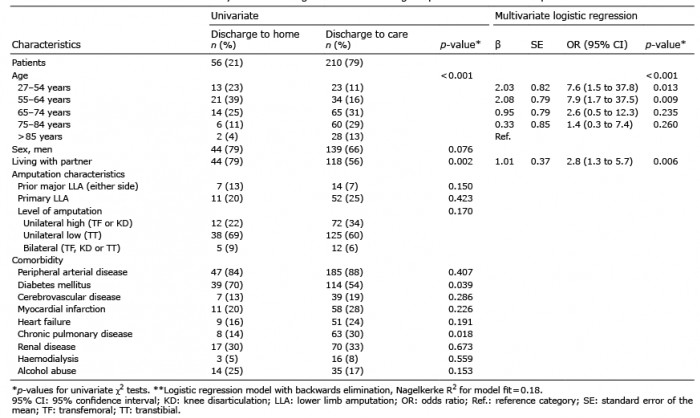 Click to show fullsize
Click to show fullsize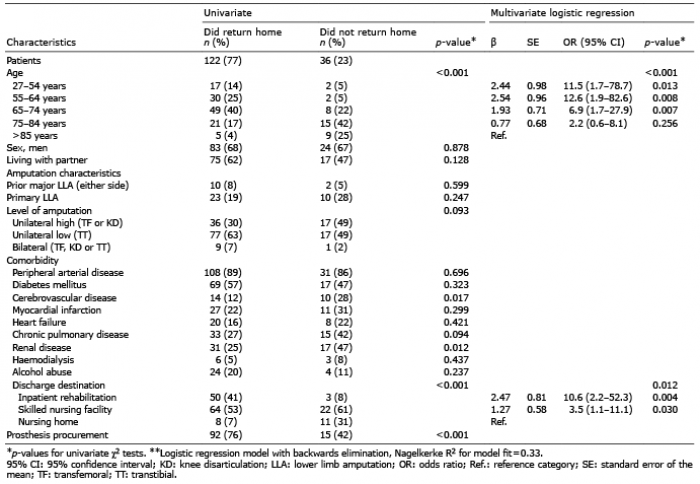 Click to show fullsize
Click to show fullsize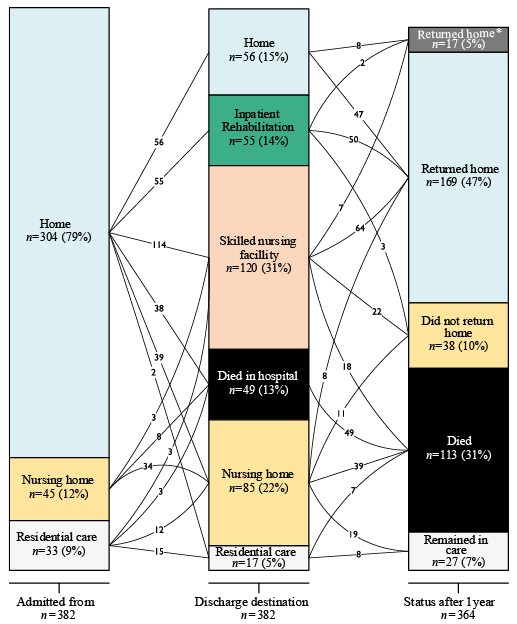 Click to show fullsize
Click to show fullsize