
From the 1Department of General Biochemistry, Faculty of Biology and Environmental Protection, University of Lodz, 2Department of Neurological Rehabilitation, Medical University of Lodz and 3Laboratory of Medical Genetics, Faculty of Biology and Environmental Protection, University of Lodz, Lodz, Poland
Background: Activation of immunologically competent cells results in the overproduction of pro-inflammatory factors, and causes progression of nerve tissue damage. However, the potential neuroprotective effects of these factors in brain damage have not been well investigated.
Objective: To evaluate the effect of extremely low frequency electromagnetic field (ELF-EMF) treatment on the molecular mechanism of inflammatory cytokine activity in post-stroke patients.
Methods: All patients underwent the same rehabilitation program, but the ELF-EMF group were also given ELF-EMF treatment. Both groups have been used in our previous studies. In order to determine the plasma level of cytokines, the levels of interleukin 1β (IL-1β), interleukin 2 (IL-2), interferon-γ (INF-γ) and transforming growth factor β (TGF-β) were evaluated, and the level of IL-1β mRNA expression was determined.
Results: After ELF-EMF treatment, both IL-1β plasma level and IL-1β mRNA expression level, as well as IL-2 plasma level increased, while IFN-γ and TGF-β levels did not change.
Conclusion: The increased expression of IL-1β found in this study may be a response to ELF-EMF stimulation. It is hypothesized that a neuroprotective role of this cytokine may occur due to IL-1β-dependent regulation of neurotrophic factors. Further research is needed to explore this hypothesis.
Key words: extremely low frequency electromagnetic field treatment; interleukin 1; stroke; rehabilitation.
Accepted Oct 29, 2019; Epub ahead of print Nov 5, 2019
J Rehabil Med 2019: 51: 854–860
Correspondence address: Michal Bijak, Department of General Biochemistry, University of Lodz, Pomorska 141/143 90-236 Lodz, Poland. E-mail: michal.bijak@biol.uni.lodz.pl
During stroke, overproduction of pro-inflammatory factors occurs, which leads to the progression of brain damage. However, current knowledge indicates that these factors may also impact on protective processes in brain tissue, but this has not been well investigated. This study evaluated the effect of extremely low frequency electromagnetic field treatment on the molecular mechanism of inflammatory cytokine activity in patients after stroke. A total of 48 patients were included in the study and were divided into 2 groups. Both groups have been used in our previous studies. All patients underwent the same rehabilitation program, but the study group also given magnetotherapy. Levels of interleukin 1β plasma, interleukin 1β mRNA expression, and interleukin 2 plasma increased after magnetotherapy. The increased expression of interleukin 1β may be a response to electromagnetic field stimulation, and it is possible that this cytokine has a neuroprotective role; however, further research is needed to explore this hypothesis
Rehabilitation is probably one of the most important phases of recovery for many stroke patients. The effect of stroke usually enforces the necessity of the relearning process. Rehabilitation can improve basal functions after stroke because of the neuroplastic ability of the brain. The term “brain plasticity” encompasses all the modifications in the organization of neural components occurring in the central nervous system. Neuronal plastic phenomena is likely to be at the basis of learning and adaptive modifications in response to anatomical or functional deficit or brain damage (1). The destruction of neural networks stimulates reorganization of the connections and this modification process is regulated by neurotrophic factors (2).
The mechanisms underlying network reorganization and regaining of basal functions in stroke patients are incompletely understood. The process of neurogenesis is regulated by many factors, including neurotrophins, growth factors, neurotransmitters and microenvironmen-tal factors (3). Recent investigations have reported that these mechanisms could involve immune responses. The inflammatory reaction that is initiated in the peripheral blood immediately after stroke, due to the response to phenomena occurring in the area of acute ischaemia, affects the normal development of plastic changes (4).
It is known that the activation of immunologically competent cells results in the overproduction of pro-inflammatory factors, which are responsible for progression of neurodegenerative diseases (5), but their potential effects on neuroprotection have not been well investigated in neurodegenerative diseases. Little is known about endogenous regulatory immune mechanisms involved in neuro-restoration. However, some recent evidence suggests that inflammatory reactions can be also neuroprotective. Ischaemic inflammatory events (the activation of glial cells, production of number of destructive mediators including pro-inflammatory cytokines, and infiltration of monocytes into the brain) have been shown to contribute to brain injury, but, on the other hand, activated inflammatory cells can participate in tissue remodelling following brain damage (6).
Early post-stroke physical therapy, including the use of extremely low frequency electromagnetic field (ELF-EMF) treatment, is beneficial in restoring the patient after stroke, mainly due to anti-inflammatory, regenerative, and analgesic actions. Moreover, the beneficial effect of ELF-EMF is to promote cell proliferation, protein synthesis, ion transport and changes in cellular signal transmission (7).
The impact of ELF-EMF on biological systems is, however, unclear. Our previous study indicated that ELF-EMF treatment results in the activation of antioxidant enzymes and increases the level of neurotrophic factors in vivo in post-stroke patients, probably as a result of the impact of ELF-EMF on gene expression (8, 9).
One potential target for ELF-EMF treatment is the immune system. Several studies indicate that ELF-EMF regulates the activity of immune cells (10, 11). Experimental data indicate that, in both animals and humans, several inflammatory cytokines (i.e. IL-1, IL-6, and TNF-α) are associated with stroke severity, and thus have a direct impact on the plasticity processes occurring after stroke (12).
The aim of this study was to investigate the effect of ELF-EMF treatment on the molecular mechanism of inflammatory cytokine activity in post-stroke patients.
Subject selection and rehabilitation protocol
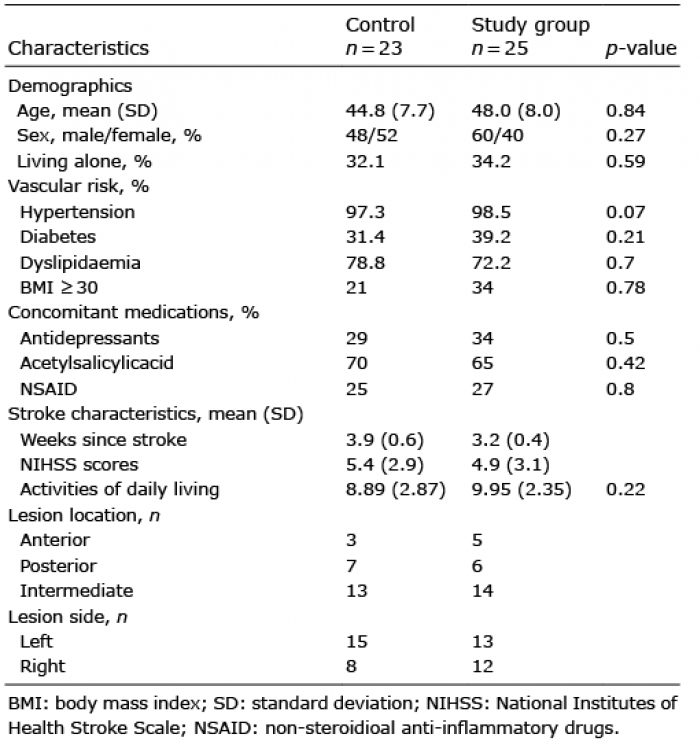
A total of 48 post-stroke patients were enrolled in the study. Patients were hospitalized in the Neurorehabilitation Ward, III General Hospital in Lodz, Poland. The clinical and demographic characteristics of the patients are shown in Table I. The cerebral ischaemic event in each patient was documented by computer tomography (CT) scan of the brain. Neurological and CT findings were interpreted by 2 or more independent experienced neurologists. All patients were diagnosed with ischaemic stroke. Patients with other types of stroke were excluded. Other exclusion criteria were: patients with neurological illness other than stroke; chronic or significant acute inflammatory factors; and/or dementia.
Table I. Characteristics of the study groups
All patients received a rehabilitation programme of aerobic exercise, as described below. Participants were randomly divided into 2 groups: an ELF-EMF group (n = 25), who were additionally rehabilitated with ELF-EMF treatment, and a non-ELF-EMF group (n = 23).
Both groups have been used in our previous studies, in which we tested gene expression of neurotrophic factor, antioxidant and nitric oxide synthesis enzymes (8, 9, 13), because of same techniques were not been available at that time.
In both the groups, the patients received a rehabilitation programme provided by a physiotherapist, every day for a period of 4 weeks with weekend breaks. The rehabilitation programme in post-stroke rehabilitation consisted of 15 min of psychotherapy, 60 min neurophysiological session in the morning (30 min of shaping techniques and 30 min of repetitive task practice or balance) and 30 min aerobic training (2–3 times a day for 10 min at 60 min intervals). Neurophysiological rehabilitation consisted mainly of functional rehabilitation shaping techniques and repetitive task practice designed to intensively use the affected upper and lower limbs. The shaping techniques included activities based on activities of daily living. However, training time was individually modified depending on the improvement in motor function of the affected limbs, if necessary. The rehabilitation programme in the control group consisted of a 60 min session in the morning (30 min of shaping techniques and 30 min of balance training), 30 min aerobic training (2–3 times a day for 10 min at 60 min intervals) and 30 min muscle strengthening exercises. The range of physical effort during the rehabilitation programmes in both groups of patients was between 13 and 14 according to Borg scale (moderate effort).
ELF-EMF treatment (15 min) was performed using a Magnetronic MF10 generator (EiE Elektronika i Elektromedycyna, Otwock, Poland) (Fig. 1), with specific parameters (magnetic induction of frequency of 40 Hz, magnetic induction of 5 mT. The pulses were applied using an AS-550 applicator (EiE Elektronika i Elektromedycyna, Otwock, Poland), which has the following properties: 550 mm diameter, 270 mm length, and 5 layers of 187 turns of 1.45-mm twin-parallel wires. Both groups were treated for the same time (15 min), although the non-ELF-EMF group were only given sham exposures. Patients with metal and/or electronic implants (pacemakers, etc.), were excluded from the study group.
Fig. 1. Schematic diagram of extremely low frequency electromagnetic field (ELF-EMF) treatment device.
Blood samples were taken before and after a standard 10 sessions of treatment (with an interval of 14 days). Samples were collected into anticoagulant solution, containing citric acid, sodium citrate, monobasic sodium phosphate, dextrose, and adenine (CPDA1) (Sarstedt, Nümbrecht, Germany), between 7 am and 9 am, under fasting conditions. Immediately upon collection, a portion of the sample was frozen at –80°C, for evaluation of mRNA expression. For isolation of plasma, the remaining samples were centrifuged (1,500 g, 15 min, 25°C). All blood samples were stored using the same protocol.
The study protocol was approved by the ethics committee of the Faculty of Biology and Environmental Protection of University of Lodz, Poland (number 28/2015). All participants provided written informed consent.
Cytokine level analysis in plasma
Measurements of interleukin 1β (IL-1β), interleukin 2 (IL-2), interferon-γ (INF-γ) and transforming growth factor β (TGF-β) in plasma samples were performed with Human IL-1β development kit, Human IL-2 development kit, Human INFγ development kit, and Human TGF-β development kit, respectively (MABTECH, Cincinnati, OH, USA), according to the manufacturer’s protocol. All measurements were made using MaxiSorp plates (Nunc, Roskilde, Denmark). The absorbance was measured at 450 nm.
Isolation of mRNA and reverse transcription
Isolation of RNA from frozen whole-blood samples was executed using TRI Reagent® (Sigma-Aldrich, Saint Louis, MO, USA). InviTrap Spin Universal RNA Mini Kit (Stratec Biomedical Systems, Birkenfeld, Germany) was used for purification of the RNA-containing aqueous phase. Estimation of purity and quantity of isolated RNA was performed using a Synergy HTX Multi-Mode Microplate Reader, equipped with a Take3 Micro-Volume Plate (BioTek Instruments Inc., Winooski, VT, USA). Then, RNA samples (diluted to 10 ng/µl) were transcribed onto cDNA using a High-Capacity cDNA Reverse Transcription Kit (Applied Biosystems™, Waltham, MA, USA). All steps were performed in accordance with the manufacturers’ protocol.
Real-time PCR analysis of gene for IL-1β expression
Expression levels of the analysed gene were determined using the following TaqMan probes: Hs01555410_m1 for human IL-1β gene, and Hs99999905_m1 for human GAPDH gene as an endogenous control (Life Technologies, Carlsbad, CA, USA). Real-time PCRs were performed in a CFX96 Real-Time PCR system (BioRad Laboratories, Hercules, CA, USA), with used a TaqMan™ Gene Expression Master Mix (Life Technologies, Carlsbad, CA, USA). All procedures were conducted according to the manufacturers’ instructions. The calculation of relative expressions of the analysed gene was performed using the equation 2–ΔCt, where ΔCt=Ct(target gene) – Ct(GAPDH).
Statistical analysis
For comparison of differences in obtained parameter changes between the ELF-EMF group and non-ELF-EMF group changes in these parameters we calculated after appropriate treatments. For all subjects the values of parameters before treatments were used as the output value (100%). The raw data are shown in Table II. Data from experiments performed on these same subjects after appropriate treatments were expressed as percentages of output value. All results were expressed as means (standard deviations (SD)). All statistical analyses were performed using StatsDirect statistical software V. 2.7.2. The results were analysed for normal distribution with the Shapiro–Wilk test. The significance of differences between the values obtained for patients before and after treatments were analysed using a test for normal distribution (paired Student’s t-test), whereas the significance of differences between the ELF-EMF group and non-ELF-EMF group was determined using unpaired Student’s t-test or Mann–Whitney U test. For all analysis a level of p < 0.05 was considered statistically significant.
Table II. Raw data for results obtained in this study (before transformation to % values)
This comparative analysis demonstrated the effect of ELF-EMF treatment on the expression of various pro-inflammatory cytokines. The plasma level of IL-1β in the ELF-EMF group after 10 sessions of rehabilitation was significantly higher than in the non-ELF-EMF group (p < 0.05). The increase in IL-1β level in the ELF-EMF group was approximately 100% (p < 0.05), while in the non-ELF-EMF group it remained at a comparable level (p > 0.05) (Fig. 2). The effect of ELF-EMF on gene expression in the whole-blood samples of IL-1β was also investigated. After ELF-EMF treatment, the expression of IL-1β mRNA increased approximately 70% (p < 0.001), while in the non-ELF-EMF group it did not change (Fig. 2).
Fig. 2. Comparison of the interleukin 1β (IL-1β), level obtained from the extremely low frequency electromagnetic field (ELF-EMF) group vs the non-ELF-EMF group. (A) IL-1β plasma concentration. Statistical significance between ELF-EMF and non-ELF-EMF groups: b vs d: p < 0.05. (B) IL-1β mRNA expression. Statistical significance between ELF-EMF and non-ELF-EMF groups: b vs d: p <0.0001.
Moreover, after a standard series of 10 physical treatments, the IL-2 plasma concentration in the ELF-EMF group increased approximately 15% (p < 0.05), but in the non-ELF-EMF group it remained unchanged (p > 0.05) (Fig. 3). An increase in plasma concentration, almost identical in value, was measured during comparative analysis of plasma IFN-γ concentration, but the increase in IFN-γ concentration observed in the ELF-EMF group was not statistically significant (Fig. 4). The reverse effect after treatment was demonstrated in the case of plasma TGF-β concentration. The TGF-β level in the ELF-EMF group was unchanged, whereas in the non-ELF-EMF group was increased, but not statistically significant. (Fig. 5).
Fig. 3. Comparison of the plasma interleukin 2 (IL-2) levels obtained from the extremely low frequency electromagnetic field (ELF-EMF) group vs the non-ELF-EMF group. Statistical significance between ELF-EMF and non-ELF-EMF groups: b vs d: p < 0.05. a) value obtained in non-ELF-EMF group before treatment, b) value obtained in non-ELF-EMF group after treatment, c) value obtained in ELF-EMF group before treatment, d) value obtained in ELF-EMF group after treatment.
Fig. 4. Comparison of the plasma interferon γ (INFγ) levels obtained from the extremely low frequency electromagnetic field (ELF-EMF) group vs the non-ELF-EMF group. a) value obtained in non-ELF-EMF group before treatment, b) value obtained in non-ELF-EMF group after treatment, c) value obtained in ELF-EMF group before treatment, d) value obtained in ELF-EMF group after treatment.
Fig. 5. Comparison of the plasma level of transforming growth factor β (TGF-β) in the extremely low frequency electromagnetic field (ELF-EMF) group vs the non-ELF-EMF group. a) value obtained in non-ELF-EMF group before treatment, b) value obtained in non-ELF-EMF group after treatment, c) value obtained in ELF-EMF group before treatment, d) value obtained in ELF-EMF group after treatment.
Damage to the brain tissue due to stroke is associated with inflammation. The immune and inflammatory responses are involved in both acute brain injury and prolonged inflammatory response, as well as subsequent brain rehabilitation after stroke; they induce tissue reconstruction and repair via the removal of dead cells, developing an anti-inflammatory milieu and generating pro-survival factors (14).
Microglial cells (monocytes) play a central role in brain inflammation, and are essential for the maintenance of integrity of the central nervous system (CNS). Microglia cells are the first non-neuronal cells that respond to injury, and they are the main source of pro-inflammatory mediators. Furthermore, immediately after acute events, such as stroke, blood-borne T and B lymphocytes invade the CNS and stimulate resident or infiltrating inflammatory cells, resulting in the development of inflammation. Through these interactions, the brain’s precursor cells become activated and may contribute to the healing process via the generation of new cells to substitute for the neurones and glia that have died due to stroke (15).
The latest reports suggest that inflammatory responses following injury to the CNS may not be entirely negative, since they may also represent neuroinflammatory events occurring as reparative mechanisms (16). Following brain trauma, a local remedial response and deep remodelling (remodelling) to restore the most important functions of the nervous tissue occur. As a result of damage to the CNS, the progenitor cells of oligodendrocytes proliferate and differentiate into mature oligodendrocyte cells that carry out re-myelination processes, restoring the communication between neurones (17).
Over recent decades, accumulating evidence suggests that ELF-EMF has significant biological effects. There is considerable evidence to show that exposure to ELF-EMF can affect numerous biological functions, both in vivo and in vitro, including DNA synthesis, RNA transcription and gene expression (18), protein synthesis, tissue repair, regulation of cell differentiation (19) and cell proliferation (20). Exposure to ELF-EMF can also modify the biophysical properties of cell membranes, including their permeability to Ca2+ ions (21). Exposure to ELF-EMF reportedly modifies intracellular Ca2+ levels in rat thymic lymphocytes, human T-lymphocytes, and Jurkat cells (22–24). Depending on the dose (field induction and frequency) and duration of treatment, and the type of inflamed tissue, exposure to EMF can be harmful or may induce a cytoprotective cellular response (25).
Many studies have shown that voltage-dependent calcium channels may account for the biological effects of exposure to EMF. It has also been shown that calcium channel blockers can greatly reduce the effects of exposure to ELF-EMF, and cause interference in cell differentiation and neurogenesis, with Ca2+ influx into cells (26). It is well documented that Ca2+ ions affect activity-dependent gene expression (27) and this effect is mediated by signalling pathways activating Ca2+-responsive DNA regulatory elements, including the transcription factor CREB, associated with cell survival, neuronal differentiation, synaptic plasticity, neurogenesis, and numerous other cell functions (28).
The potential use of electromagnetic field in stroke rehabilitation was presented in study by Pena-Philippides et al. (29). They tested the effect of pulsed electromagnetic field (PEMF) on infarct size and inflammation in a mouse model after cerebral ischaemia. This study demonstrated that PEMF significantly influenced the expression profile of pro- and anti-inflammatory factors in the hemisphere ipsilateral to ischaemic damage (29). A subsequent study in a human model was performed by Capone et al., who showed that 1 mT ELF-EMF reduced ischaemic lesion size in patients with acute ischaemic stroke, which strongly suggested that ELF-EMF could represent a potential therapeutic approach after ischaemic stroke (30). Our previous study estimated the clinical status of patients with the National Institutes of Health Stroke Scale (NIHSS), Barthel Index of Activities of Daily Living (ADL), modified Rankin Scale (mRS), Mini-Mental State Examination (MMSE) and Geriatric Depression Scale (GDS). Stroke-related neurological deficit, estimated using NIHSS, decreased approximately 65% more in the ELF-EMF group than in the non-ELF-EMF group. mRS decreased in both groups, but in the ELF-EMF group the reduction was approximately 50% greater than in the non-ELF-EMF group. Approximately 35% greater improvement in cognitive impairment, as estimated by MMSE, was observed after ELF-EMF treatment. Depressive syndrome, measured in GDS, decreased significantly, while ΔGDS gained approximately 45% better results in the ELF-EMF group than in the non-ELF-EMF group (9).
The regeneration of tissues depends on the course of inflammation being controlled, so that the acute inflammatory response does not become chronic. The acute inflammatory condition allows the tissue to regenerate through cell proliferation, while chronic inflammation continuously destroys the tissue after it has been repaired. Although drugs are commonly used to suppress the inflammatory response, there is evidence to show that suppressing inflammation can hinder wound healing (31).
Although the delayed inflammatory response to stroke induces secondary neurological injury, several studies have shown that many cytokines can modulate the expression of neurotrophins and their receptors, which may indicate the involvement of inflammatory mediators in neuroplasticity processes (32). In light of this, we investigated whether exposure of post-stroke patients to ELF-EMF affects expression of pro-inflammatory cytokines (IL-1β, IL-2, INF-γ and TGF-β). Among the pro-inflammatory cytokines measured in the plasma of post-stroke patients after ELF-EMF treatment, we found evidence that ELF-EMF has a substantial impact on interleukins, which was not noted in the non-ELF-EMF group (Figs 2, 3). The level of INF-γ was slightly higher, but this increase was not statistically significant (Fig. 4), and the level of TGF-β did not change (Fig. 5) after magnetotherapy treatment.
IFN-γ is considered a key regulator of immune and inflammatory responses and is absent from normal brain parenchyma. The data indicate that IFN-γ/IP-10 is a major inflammatory signal pathway in the immune response to stroke (33). Zhang et al. reported that IFN-γ can protect the stem cell population during inflammatory response and can stimulate stem cell neurogenesis. Co-injection of neural stem cells and IFN-γ have been shown to improve therapeutic outcomes in a model of ischaemic stroke in rats. IFN-γ treatment significantly increased neurogenesis in vivo, and induced levels of subsequent neuronal differentiation of cytokines BDNF, VEGF, IGF-1 and TGF-β (34).
TGF-β is a multifunctional cytokine that plays an important role in the control of the immune system, regulating cell growth, proliferation, differentiation and apoptosis. TGF-β is also involved in the pathogenesis of cerebrovascular diseases. Evidence suggests that IFN-γ can modulate TGF-β activity in vitro and negatively regulate the TGF-β signalling pathway at wound sites in vivo (29). However, further studies are needed to assess whether there is crosstalk between the IFN-γ and TGF-β signalling pathways in various pathological conditions. In the current study, we observed that the TGF-β plasma level increased in the non-ELF-EMF group, but was unchanged in the group exposed to ELF-EMF (Fig. 4). The reported effects were opposite to those for IFN-γ; however, none of the changes were statistically significant.
Statistically significant increases in IL-1β (approximately 100%) and IL-2 (approximately 15%) plasma levels were observed after application of ELF-EMF treatment (Figs 2 and 3).
IL-2 is generally viewed as a pro-inflammatory cytokine, but its role in acute ischaemic stroke is not clear; little information is available on IL-2 in post-stroke patients. It is likely that, as with other pro-inflammatory cytokines, IL-2 works remarkably in the first phase after stroke, but its further increase may be destructive. Nayak et al. found a significant increase in plasma level of IL-2 in post-stroke patients in the hyperacute stage (0–24 h), compared with a healthy control group (35). This level gradually decreased with treatment at successive intervals: 48, 72, and 144 h in improved patients, compared to patients who have died. In addition, IL-2 has been shown to regulate the proliferation and survival of regulatory T cells (Tregs), which exert important neuroprotective effects in stroke (36).
The current study showed, for the first time, that ELF-EMF treatment not only increased IL-1β concentration, but also increased IL-1β mRNA expression in vivo in humans (Fig. 1). This result should be interpreted taking into account the complex effects of this cytokine, and especially its role in acute inflammation and tissue repair. IL-1β is responsible for a broad spectrum of immune and inflammatory responses, induces T-cell and B-cell activation, and consequently the synthesis of other pro-inflammatory cytokines (such as IFN-γ, IL-6 and TNF) and antibody production. IL-1β is widely considered as a constitutive factor in the brain; its expression declines to low levels in the normal adult and increases markedly after injury (37).
It is well documented that ELF-EMF treatment reduces the inflammatory response in many pathological conditions, and thereby improves the condition and function of a variety of tissues. EMF has also been shown to modulate an inflammatory cytokine after traumatic brain injury in rats. Electromagnetic pulse (EMP) treatment attenuated IL-1β levels up to 10-fold in cerebrospinal fluid (CSF) within 6 h after initial injury and also significantly suppressed IL-1β within 17–24 h after penetrating injury (38). Indeed, some studies have reported a positive correlation between IL-1β and BDNF levels, demonstrating that this interleukin is able to modulate pro-survival BDNF signalling (39). Furthermore, some cytokines, such as IL-1 and IL-6, are known to improve neuronal survival in stressed cellular paradigms (40). The increase in IL-1β expression reported in this study may be a response to ELF-EMF stimulation and, in light of the previous research discussed above, it can be hypothesized that a neuroprotective role of this cytokine might be attributable to IL-1β-dependent regulation of neurotrophic factors. However, further research is needed to verify this hypothesis.
This study was supported by the Department of General Biochemistry, Faculty of Biology and Environmental Protection, University of Lodz, Lodz, Poland (number 506/1136).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize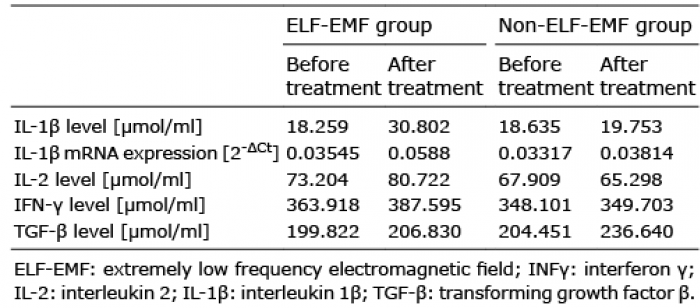 Click to show fullsize
Click to show fullsize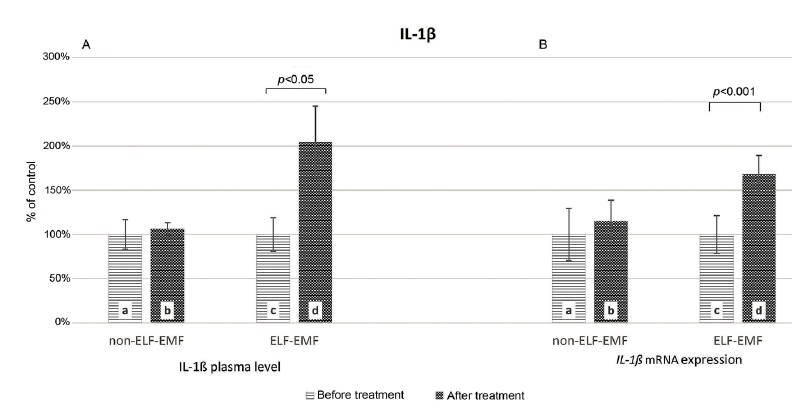 Click to show fullsize
Click to show fullsize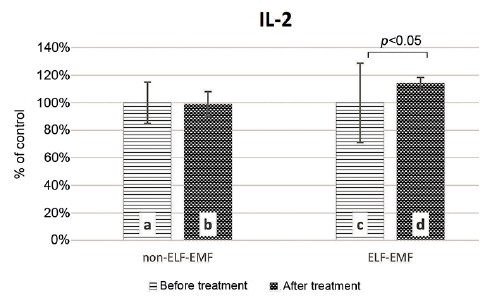 Click to show fullsize
Click to show fullsize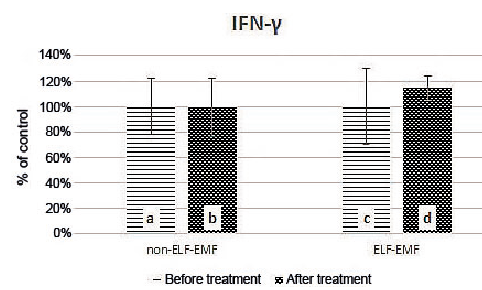 Click to show fullsize
Click to show fullsize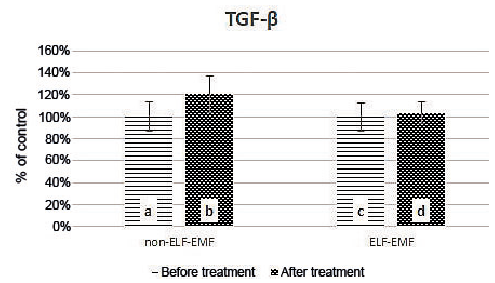 Click to show fullsize
Click to show fullsize