
From the 1Department of Neuromedicine and Movement Science, NTNU – Norwegian University of Science and Technology, 2Stroke Unit, Department of Medicine, St Olavs Hospital, Trondheim, Norway and 3Stroke Division, Florey Institute of Neuroscience and Mental Health, University of Melbourne, Melbourne, Australia
Objectives: To explore mechanisms affecting mental health in patients with stroke. The aims were to investigate the association between pre-stroke physical activity and symptoms of anxiety and depression 3 months after stroke, and to investigate how self-reported physical activity changed from before to 3 months after the stroke.
Design: Secondary analyses of a prospective observational multicentre study.
Patients: Stroke patients from 11 Norwegian stroke units.
Methods: Symptoms of anxiety and depression were measured using the Hospital Anxiety and Depression Scale, and physical activity was assessed by self-report. Negative binomial regression was used to analyse associations.
Results: The analysed sample consisted of 205 patients; mean age was 74 years (standard deviation (SD) 11.5); 46% were women. Higher activity levels before stroke were associated with fewer symptoms of depression in multivariable analyses with regression coefficient of 0.84 (95% confidence interval 0.73–0.97), p = 0.015. Eighty-five (41.5%) patients reported similar activity levels before and after
stroke.
Conclusion: In this group of patients with mild symptoms of emotional distress, it seems that pre-stroke physical activity might be protective against post-stroke depression, but not anxiety. Many patients with mild-to-moderate stroke report being equally active before and after the stroke.
Key words: cerebrovascular disease; mental health; exercise; depression; physical activity.
Accepted Sep 18; 2019; Epub ahead of print Sep 30, 2019
J Rehabil Med 2019; 51: 755–760
Correspondence address: Martina Reiten Bovim, Norwegian University of Science and Technology (NTNU), Department of Medicine and Health Science, 7491 Trondheim, Norway. E-mail: martina.r.bovim@ntnu.no
Depression and anxiety are more common after stroke than in the general population. In non-stroke patients, physical activity and exercise is associated with less psychological distress. This study found that pre-stroke physical activity was associated with fewer depressive symptoms 3 months after stroke. However, being physically active was not related to symptoms of anxiety. In addition, most patients reported performing approximately the same level of physical activity before and after stroke. Despite the lack of causality, these findings indicate that pre-stroke physical activity might be protective against post-stroke depression, but not against anxiety.
The Global Burden of Disease studies state that depression and anxiety are among the leading causes of disability worldwide (1). Results from systematic reviews show that stroke patients are even more vulnerable to emotional distress than the general population (2–5). The higher prevalence of post-stroke anxiety and depression might be a consequence of the life-changing event of having a stroke (2, 6). However, evidence implies that underlying biological changes could have some importance, at least in the development of post-stroke depression (2). Both depression and anxiety are associated with poor outcome after stroke, affecting independence in activities of daily living, reducing quality of life and, in the case of depression, increasing mortality (7–10).
There is some evidence of the beneficial effects of physical activity (PA) and exercise in stroke patients, as it reduces disability and the risk of subsequent cardiovascular events (11–14). Exercise seems to have a therapeutic effect in people with depression and anxiety without stroke (15–17). Furthermore, epidemiological studies have found that higher levels of PA are associated with fewer symptoms of depression in the general population, while there is conflicting evidence of its association with anxiety symptoms (18–20). In the case of stroke, we know less about the potential relationship between PA and depression or anxiety. The aetiology of anxiety and mood disorders in stroke patients might differ from that in non-stroke patients (2). While PA appears to be associated with less depressive symptoms after stroke, at least during maintenance of activity (21), it is unknown how post-stroke exercise influences anxiety. Importantly, most PA and exercise studies have failed to consider whether activity levels before the stroke may influence the prevalence of anxiety and depression among stroke survivors.
The primary aim of this study was to investigate the association between PA in the time before stroke, and symptoms of anxiety and depression 3 months later. We hypothesized that patients who reported more PA before stroke would have fewer symptoms of anxiety and depression at 3 months post-stroke. The secondary aim was to examine how activity levels changed from before to 3 months after stroke. The secondary hypothesis was that patients would report a lower level of activity after stroke than before stroke.
Study design
This was a secondary analysis of data from a Norwegian prospective observational multicentre study, the LEAST study (22). The primary aim of the LEAST study was to examine the amount and quality of early mobilization provided to stroke patients in Norwegian stroke units. Patients were recruited from 11 different stroke units from December 2011 to June 2013. Hospitals were screened for eligible patients once every fortnight, and inclusion was performed if 2 or more eligible patients were hospitalized.
Patient sample
Patients were eligible if they were diagnosed with acute stroke according to the World Health Organization’s definition (23) within 14 days before inclusion, were over 18 years of age, and were able to speak and understand the Norwegian language. Patients could consent for themselves or, in keeping with Norwegian consent procedures, could be included if unable to consent for themselves when their next of kin did not oppose participation. To be included in the analyses, the Hospital Anxiety and Depression Scale (HADS) and questions concerning pre-stroke and post-stroke activity needed to be complete. Patients were excluded if they received palliative care, or were discharged from hospital before the required information was assessed at baseline. After discharge from hospital, all patients were followed according to the National Norwegian Guidelines. Inclusion and follow-up were performed by 4 trained research assessors: 1 physician, 1 physiotherapist, 1 nurse and 1 medical student. None of these had a therapeutic relationship with the patients. The study was approved by the Regional Committee for Medical and Health Research Ethics in Norway (REC no 2011/1428).
Procedure and outcome variables
Patients were included within 14 days after stroke, and reassessed 3 months later. The 3-month follow-up was conducted in an outpatient clinic, by home visit or by telephone.
At baseline, patient characteristics, such as sex, age and type of stroke, were recorded. Stroke severity was obtained using the National Institutes of Health Stroke Scale (NIHSS) (24). Functional levels before and 3 months after stroke were assessed using the modified Rankin Scale (mRS) (25).
The primary outcome was symptoms of anxiety and depression 3 months after stroke, which was measured using the HADS (26). This questionnaire consists of 14 questions; 7 covering anxiety symptoms and 7 covering depressive symptoms. HADS is not a diagnostic tool, but can be used to score symptoms of anxiety and depression. Each question scores from 0 to 3, with a maximum total score of 42; 21 for each subscale. A higher score indicates more severe symptoms. It is recommended that the subscales are used separately (27). A cut-off score of 8 is suggested for case finding, giving an optimal balance between sensitivity and specificity (28), and is used when describing the data in this study. The scale format of the HADS has been used in the regression analyses. Patients with a very high score were seen by a physician in relation to the project unless they were already receiving adequate care.
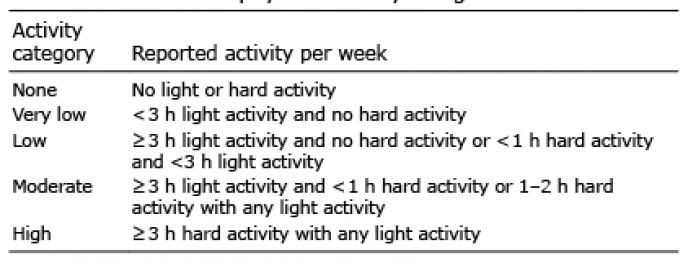
Self-reported physical activity (PA) was measured at inclusion and at the 3-month follow-up by using questions from the HUNT2-questionnaire. This is a short questionnaire that is easy to administer, asking the participants to rate how many hours they had spent in light and in hard PA during a certain time-period (29). At inclusion, patients were asked how many hours (mean per week) they had spent in light and hard PA for the past year (pre-stroke). Light activity was defined as activity without sweating or becoming out of breath, while hard activity was characterized as sweating or becoming out of breath. Response opportunities were: none, ≤ 1 h, 1–2 h or ≥ 3 h for both categories. Three months after stroke, patients were asked the same questions, considering activity level since the stroke. In order to merge the 2 PA categories (light and hard activity) into 1 variable, they were summarized according to an algorithm used in a previous study, and further divided into 5 categories; none, very low, low, moderate and high PA (30). Definitions are described in Table I. Only patients who had completed the HADS and the questions on PA were included in the analyses.
Table I. Definition of physical activity categories
Statistical analysis
Proportions were analysed and p-values generated using the Pearson’s χ2 test. Mann–Whitney U test was used to compare groups for variables with a skewed distribution and independent sample t-test was used for variables that complied with normal distribution.
Associations between PA and symptoms of anxiety and depression were analysed using negative binomial regression, as responses to the HADS score were not normally distributed. Using this statistical method made it possible to keep the scale format of the dependent variables, as opposed to dichotomizing them, omitting valuable information. Univariate and multivariate analyses were performed with covariates that, based on the literature and clinical judgement, were thought to influence symptoms of anxiety and depression (2, 31).
Wilcoxon signed-rank test was used to compare levels of activity before and after stroke. Collinearity was tested using the variance inflation factor (VIF). In the regression analysis, the activity categories “none” and “very low” activity were merged, due to the low number of patients in the no-activity group. p-value < 0.05 was considered significant in the analyses. Statistical analyses were performed in SPSS 25 and Stata 15.
A total of 547 patients were screened for inclusion, and 390 patients were included in the LEAST study. The flow of patients is illustrated in Fig. 1.
Fig. 1. Flow chart of participants in the study. PA: physical activity; HADS: Hospital Anxiety and Depression Scale.
Baseline information of patients with complete vs not complete dataset is listed in Table II. Patients responding to the questionnaires, and hence included in the analyses, were significantly younger, with less severe strokes and higher functional level both pre- and post-stroke, compared with those not responding.
Among the 205 respondents, the median score on the HADS-anxiety was 1 (interquartile range (IQR) = 4) and median score on HADS-depression was 3 (IQR = 4) 3 months after stroke. Thirty-four patients (16.6%) scored above the cut-off for depression, and 23 patients (11.2%) scored above the cut-off for anxiety.
Table II. Baseline data of patients responding and not responding to questionnaires
Variance inflation factor (VIF) was below 1.6 for pairwise correlation between all variables in the regression model, indicating no severe collinearity between any of the covariates. As shown in Table III, pre-stroke PA was not associated with symptoms of anxiety 3 months after stroke, but it was associated with symptoms of depression. In multivariable regression, pre-stroke PA was associated with fewer symptoms of depression when adjusted for age, sex, premorbid mRS and NIHSS at inclusion. This association indicates that for each unit increase in premorbid PA, the score on HADS-depression is reduced by a factor of 0.84, 95% CI 0.73–0.97, p = 0.015.
Table III. Regression analysis for the association between physical activity before stroke and symptom of anxiety and depression after stroke
Fig. 2 illustrates the number of patients reporting different activity levels before and after stroke. Eighty-five patients (41.5%) reported the same activity level premorbid and 3 months after stroke. Sixty-eight patients (33.2%) reported a lower activity level 3 months after stroke than before the stroke, while 52 patients (25.4%) reported a higher activity level 3 months after stroke. There were no significant differences in the activity levels reported pre- and post-stroke, p = 0.325. Among the 34 patients scoring above cut-off for depression post-stroke, 3% reported no PA before the stroke. Very light PA was reported in 47%, light PA in 35%, moderate PA in 12% and hard PA in 3%. After stroke, the numbers were 3%, 53%, 29%, 9% and 6%, respectively.
Fig. 2. Physical activity (PA) before and after stroke. Number of patients (n) is listed for each group.
In this group of stroke survivors with mild symptoms of emotional distress, a higher level of self-reported activity before the stroke was associated with fewer symptoms of depression, but not anxiety, 3 months after stroke. Almost half of the patients reported the same activity level after as before the stroke. One in 4 reported a higher activity level, while one in 3 reported a lower activity level after compared with before the stroke.
Previous studies have revealed the potential beneficial effects exercise after stroke has on mood (21), and this study confirms that higher activity is associated with less depression symptoms after stroke. Several mechanisms might explain this interaction, such as diversion from negative thoughts through activity, increased social contact and self-efficacy (15). Physiological changes in endorphin levels may also positively influence mood (15).
Post-stroke depression has been hypothesized to have a multifactorial cause, with both biological and psychological components (2). The effect of PA might differ depending on the underlying causes of depression, and it is possible that the beneficial effects of PA are present only in certain constellations of stroke patients. It is also possible that use of antidepressant medications interferes with this relationship, although there are no studies confirming this.
One recent study found an association between higher pre-stroke PA and less severe stroke (32). However, this is, to our knowledge, the first study investigating how premorbid PA is associated with psychological well-being after stroke. The finding supports the growing evidence of the benefits of PA in promoting mental health (15, 16). Still, causality cannot be proven, and it might be that the inactivity among patients with higher symptoms of depression is a consequence of the depressive state, which might also have been present before the stroke.
No association was found between PA before the stroke and symptoms of anxiety 3 months later. Findings from epidemiological studies differ (18, 19, 33), and even though there are only a small number of RCTs investigating this relationship, with small sample sizes and lacking adequate controls, the evidence suggests that anxious patients benefit from exercise in the general population (16, 17). The intensity of the activity reported in this current study might not have been high enough to reduce symptoms of anxiety, as the RCTs have investigated exercise interventions. It is also possible that the low number of anxious patients in this study reduced our capacity to identify an association that was actually present. Anxiety can have many different clinical manifestations, such as social anxiety, generalized anxiety, and phobic disorders; hence they might be a more heterogeneous group than patients with depression (34).
The prevalence of depression and anxiety in this cohort was generally lower than reported in the literature (2, 3). Depression seems to be more common in patients with more severe stroke (2). Because depression was determined based on a questionnaire, the more severely affected patients who not were able to respond, were excluded. However, such selection bias where the poorest patients are excluded is not unique to this study. The form of administration of the HADS might influence the response, as one study found that more symptoms of depression appear to be present with use of self-administration schemes than through interview (35). Anonymity has been suggested as a possible explanation. The HADS was originally developed as a self-administered tool, but was mainly assessed through telephone interviews in the LEAST study, which might have contributed to the low prevalence of depression and anxiety. We have no good data concerning the use of antidepressant drugs or psychotherapy in these patients, which might have affected the observed prevalence.
The variables included in the regression model were tested for collinearity, because closely related variables should not be included in the same model. However, none of the variables had a strong correlation, which was rather surprising for some variables, such as PA level and mRS score. There might be several explanations for this, and it might indicate that PA depends on more than functional level alone.
More than 40% of patients reported the same activity level before and after the stroke. We have not investigated which variables were related to changes in PA levels, but severe strokes affecting functional abilities are likely to reduce PA in patients with a high pre-stroke activity level. Many patients were categorized as having a very light to light activity level, which might not be too hard to return to after the stroke. In addition, patients able to respond to the questionnaires were a selected group of patients with relatively good function, being able to walk and move about. Other features, such as becoming depressed after a stroke, might also lead to less post-stroke PA, although the literature confirming this is sparse (21). One in 4 reported a higher activity level, while 1 in 3 reported a lower activity level after stroke. We do not have information about which of these patients received physiotherapy or other support-enhancing activity. However, as most patients increased or decreased their activity only one level, the observed variation may be within expected measurement error of the self-report PA instrument. Test-retest reliability of the HUNT questions was considered to be moderately good regarding hard PA (wκ = 0.41), but poor regarding light activity (wκ = 0.2) (29). Compared with other measures of PA, such as VO2max, the questions concerning light PA correlated poorly (r = 0.03), while the questions about hard PA showed a moderate correlation (r = 0.46) (29). It is not certain that one level change in PA represent a true change in activity level, and it might be more realistic to consider the extreme changes as true changes. In fact, most patients appeared to be quite consistent in their pre- and post-stroke activity level, which was not in accordance with our hypothesis of lower activity levels after stroke. The reason for this might be the selection of patients favouring those with less severe strokes to this study. Some may also live with the impression of being as active after as before the stroke, even though this might not be the case.
Study limitations
Because of the observational design, the ability to identify causal relationships was limited, and despite adjusting the analyses for possible confounding factors, it was difficult to eliminate the risk of other variables influencing the results. Physical disability, stroke severity, history of depression and cognitive impairment are variables known to be associated with depression after stroke (2). The regression analyses were adjusted for stroke severity and pre-stroke functional disability, but history of depression and cognitive impairment were not examined in this study. Functional disability was significantly associated with both depression and anxiety, but PA and depression showed an association independent of functional disability. Information about pre-stroke mental health would have made it possible to distinguish between depression and anxiety that occurred before and after the stroke, as these entities might have different causes and progression. The use of medications for depression or anxiety might confound the effect of PA on depression and anxiety, and our analyses are limited by the lack of this information.
Another variable that might interfere with both PA, mood and anxiety is fatigue (36, 37). However, the relationships appear to be complex, especially between fatigue and depression, as fatigue might be a part of a depressive state as well as an isolated phenomenon.
The advantage of self-report schemes is that they are easy and cheap to apply, particularly in large patient groups. However, people tend to overestimate their volume of PA compared with when PA is measured with an activity measuring device (38). Hence, the actual activity level was probably lower than reported in this study. However, when it comes to pre-stroke activity level, there exist no recommendations for other plausible methods (39).
Another limitation with the self-report schemes is that they are subjective, requiring a certain level of cognitive function among participants, both when evaluating their own level of PA, and when completing the scheme, or it requires that they have a next of kin who can assist them. Asking about activity levels for the last year before the stroke introduces a risk of recall bias, and it is probably difficult to give good estimates for such a long time. Other more objective methods of assessing PA, such as activity-monitoring chips (40), are expensive in such a high number of patients, and were therefore not used in this study. However, such methods are recommended for use in further research.
Conclusion
This study shows that a higher level of PA before stroke is associated with fewer symptoms of depression after stroke, but not with symptoms of anxiety. Pre- and post-stroke self-reported activity levels appeared to be quite consistent. Although limited to associations, this study supports the benefits of PA in the general population in order to improve outcome and lessen the impact of stroke. Hence, future studies should be designed to confirm the benefit of PA in primary and secondary prevention of emotional distress after stroke.
The authors would like to thank Mari Gunnes and Christine Sandø Lundemo for their participation in collecting data.
This work was supported by the Liaison Committee between the Central Norway Regional Health Authority, the Norwegian University of Science and Technology and the Research Council of Norway [grant number 205309].
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize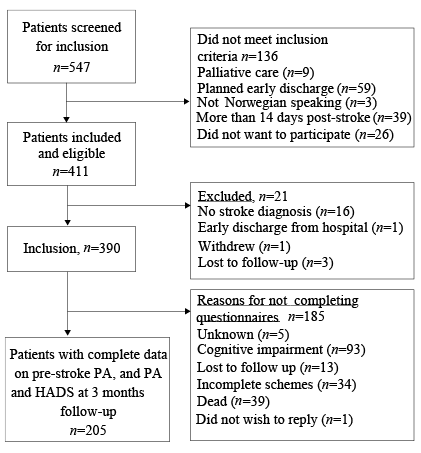 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize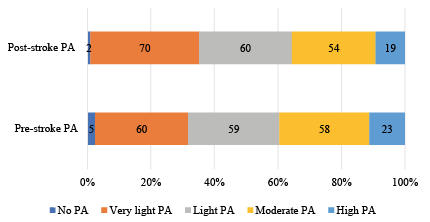 Click to show fullsize
Click to show fullsize