
From the 1Research Group Lifestyle and Health, University of Applied Sciences Utrecht, Utrecht, 2Amsterdam Institute of Social Science Research, University of Amsterdam, Amsterdam, 3Heliomare, Rehabilitation Centre, Wijk aan Zee, 4Julius Centre for Health Sciences and Primary Care, University Medical Centre Utrecht, University Utrecht, and 5National Knowledge and Advisory Centre on Migrants, Refugees and Health (Pharos), Utrecht, The Netherlands
Objective: To explore predictors of dropout of patients with chronic musculoskeletal pain from an interdisciplinary chronic pain management programme, and to develop and validate a multivariable prediction model, based on the Extended Common-Sense Model of Self-Regulation (E-CSM).
Methods: In this prospective cohort study consecutive patients with chronic pain were recruited and followed up (July 2013 to May 2015). Possible associations between predictors and dropout were explored by univariate logistic regression analyses. Subsequently, multiple logistic regression analyses were executed to determine the model that best predicted dropout.
Results: Of 188 patients who initiated treatment, 35 (19%) were classified as dropouts. The mean age of the dropout group was 47.9 years (standard devition 9.9). Based on the univariate logistic regression analyses 7 predictors of the 18 potential predictors for dropout were eligible for entry into the multiple logistic regression analyses. Finally, only pain catastrophizing was identified as a significant predictor.
Conclusion: Patients with chronic pain who catastrophize were more prone to dropout from this -chronic pain management programme. However, due to the exploratory nature of this study no firm conclusions can be drawn about the predictive value of the E-CSM of Self-Regulation for dropout.
Key words: dropout; chronic musculoskeletal pain; interdisciplinary pain management programmes; prospective cohort study; Extended Common-Sense Model of Self-Regulation; pain catastrophizing.
Accepted Sep 13, 2019; Epub ahead of print Sep 23, 2019
J Rehabil Med 2019; 51: 761–769
Correspondence address: Janke Oosterhaven, Research Group Lifestyle and Health, University of Applied Sciences Utrecht, Utrecht, The Netherlands. E-mail: janke.oosterhaven@hu.nl
Interdisciplinary pain management programmes have high dropout rates. Patient dropout from these programmes is associated with poor treatment outcomes and high financial costs for society. To improve the overall effectiveness of these programmes more insight is needed into predictors of dropout. This study explored whether patient beliefs (emotional and cognitive) about illness and treatment are related to dropout. The results revealed that patients with chronic pain who catastrophize were more prone to dropout.
Although interdisciplinary pain management programmes (IPMPs) have been shown to be moderately effective for patients with chronic pain (1, 2), there is still room for improvement, because dropout has been reported to range from 10% to 51% (3, 4) and is considered high. A recent systematic review confirmed that dropout is still a neglected topic in research in this domain, and that more high-quality research is needed based on a conceptual framework (5).
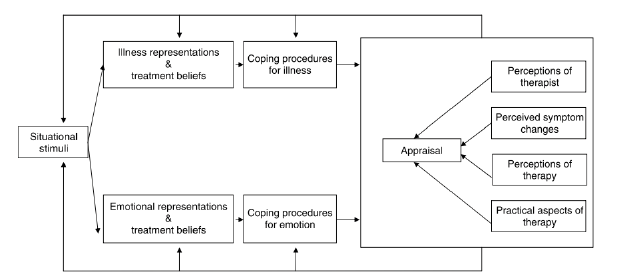
A conceptual framework to study dropout is the Extended Common-Sense Model of Self-Regulation (E-CSM of Self-Regulation) (6, 7) (Fig. 1). The E-CSM of Self-Regulation, like cognitive behavioural therapy, a central element in IPMPs, is based on social cognitive theory. Patients learn to identify, monitor and change maladaptive cognitions and feelings related to pain and behaviour. According to the E-CSM of Self-Regulation, patients with chronic pain develop simultaneous cognitive and emotional representations (beliefs/perceptions) about their illness and treatment, as a response to continuous interruptive painful stimuli. These representations guide the patient towards coping strategies, a “common sense” solution to the painful stimuli. Representations are dynamic and may change over time, influenced by perceived symptom changes and appraisal of the therapy (6, 8).
Fig. 1. A dynamic extended model of treatment and illness representations (E-CSM of Self-Regulation). Reprinted with permission of “Treatment appraisals and beliefs predict adherence to complementary therapies: a prospective study using a dynamic extended self-regulation model” by F. Bishop, L. Yardley, G. Lewith, 2008. Br J Health Psychol. 13 (4): 701–718. ©2008 The British Psychological Society (6).
Research has shown that maladaptive cognitions (ideas of suffering from a severe illness with a long duration, experiencing low personal control) or feelings of extreme worry (anxiety, depression and catastrophizing) and low self-efficacy are related to poor treatment outcomes (8, 9). Stronger beliefs in the necessity, and fewer concerns regarding the effects, of treatment lead to higher adherence rates. When treatment does not correspond to patients’ expectations, patients can become frustrated and dropout may follow (10, 11).
Published work shows that when healthcare providers fail to explore patients’ illness representations and treatment beliefs, a “mismatch” in communication can be the result (11–13). These unaddressed beliefs and treatment expectations may result in non-adherence and dropout by individual patients, both associated with poor treatment outcomes. Patient dropout may cause feelings of demoralization in providers and may lead to overutilization of the healthcare system and high financial costs at the societal level (14).
To improve the overall effectiveness of IPMPs, more insight is needed from studies which are designed a priori to predict dropout, such as prospective cohort studies (5). The central aims of this study were to explore predictors of dropout of patients with chronic musculoskeletal pain in an IPMP, and to develop and validate a multivariable prediction model based on the E-CSM of Self-Regulation.
Design
This study used a prospective cohort design. The study was registered with the Medical Ethics Committee of the Academic Medical Centre of Amsterdam, which declared that it does not fall under the scope of the “Medical Research Involving Human Subjects Act”. All patients provided written informed consent.
Subjects and recruitment
Patients with chronic pain were recruited and followed up (July 2013 to May 2015) in an interdisciplinary outpatient rehabilitation centre, Heliomare Wijk aan Zee, in the Netherlands. Chronic pain was defined as pain that persists for longer than 3 months, or pain that extends beyond the expected period of healing (15). The inclusion criterion was: having chronic musculoskeletal non-cancer pain eligible for an IPMP. The exclusion criteria were: (i) patients with chronic musculoskeletal pain with serious interfering psychiatric problems; (ii) patients not motivated for behavioural change; (iii) patients unable to read or speak Dutch; and (iv) patients involved in a health-related legal procedure of conflicting interest.
Intervention
The outpatient IPMP in Heliomare is based on cognitive behavioural therapy with patient pain neuroscience education, based on a biopsychosocial explanation of chronic pain. The programme lasts 16–20 weeks and comprises a diagnostic phase of 4 weeks, and a treatment phase of 12–16 weeks. Individual illness representations, treatment beliefs, emotional representations and coping procedures of the patients are addressed in the interdisciplinary assessments, resulting in an individually-tailored intervention programme. The treatment phase focuses on personal rehabilitation goals, enabling patients to use adequate coping strategies to improve self-management behaviour with chronic pain. The individually-tailored intervention programmes takes the form of 2–3 meetings per week for 1 h with professionals from different disciplines, such as physiotherapy, social work, occupational therapy or psychology (16).
Procedure
Study assessments were integrated into the clinical baseline assessments (T0) and post-rehabilitation assessments (T1). A total of 208 consecutive patients were invited before the start of the clinical baseline assessment by an assistant psychologist (WW) to participate in this study, of which 195 (94%) agreed. Thirteen patients refused to participate in the study for the following reasons: concentration problems, poor vision, and refusal to participate in clinical assessments. Another 7 patients were excluded as they did not have a diagnosis of chronic musculoskeletal pain. All 188 included patients completed baseline assessments as part of the intake of the IPMP and received standard rehabilitation care for 16–20 weeks (Fig. 2).
Fig. 2. Patient flowchart.
For all patients the dropout status was determined from patient registries in the institution by 2 independent researchers (JO, JD). Each patient was classified as either a programme completer (0) or dropout (1). Dropout was defined as: “patients with chronic pain, who were referred to a chronic pain management programme, who initiated (participated in the baseline assessments), but discontinued prior to completion of the entire programme” (17).
Baseline assessment measures
Sociodemographic data. To describe the research sample in this study the following sociodemographic factors were collected at baseline: age, sex (male, female), ethnicity (Dutch, non-Dutch), marital status (single, living together), educational level: low (level 0–2 early: primary education, lower secondary education); intermediate (level 3–5: upper secondary, post-secondary, short cycle tertiary), and high (level 6–8: bachelor, master, doctoral))); work status (employed, unemployed, retired, school/study); and ability to work (perceived ability to work 0–10 NRS) (16).
Pain intensity and pain duration. Other important pain-related factors that were used to describe the research sample were pain intensity (using a 0–10 numeric rating scale (NRS)) and pain duration (pain duration 0–2 years, between 2–5 years, more than 5 years). These were derived from the intake questionnaire (16).
Potential predictors for dropout derived from E-CSM of Self-Regulation. To develop a model to predict dropout in IPMPs 18 potential predictors were derived from 4 categories of the E-CSM of Self-Regulation (8, 18): 1: Illness representations; 2: Treatment beliefs; 3: Emotional representations: pain self-efficacy, pain catastrophizing, anxiety and depression; and 4: Coping procedures for illness and emotion: pain catastrophizing (see Fig. 1), as described below. All 18 potential predictors were collected during baseline assessment.
Illness representations (category 1). The Brief Illness Perception Questionnaire Dutch language version measured illness representations and emotional representations (Brief IPQ-DLV) (19). The Brief IPQ covers 5 domains of illness representations, as described in the E-CSM of Self-Regulation by Leventhal (7, 18): consequences, timeline, control, identity, cause. The Brief IPQ-DLV has 8 items rated using a 0–10 NRS for each item. The Brief IPQ is a reliable instrument to measure illness representations (19).
Treatment beliefs (category 2). Treatment beliefs were measured with the Dutch translation and adaptation of the Treatment Beliefs Questionnaire (TBQ), as designed by Cooper et al., (20, 21). The translated TBQ consists of 11 items on a 5-point Likert scale (“totally disagree”, “disagree”, “neutral”, “agree” and “totally agree”). Confirmatory factor analysis determined that there were 3 domains: “necessity”, “concerns” and “practical barriers”. Psychometric properties were investigated and considered to be fair to good. Internal consistency was fair to good, with alpha values ranging from 0.66 to 0.87. Reproducibility was high, with a small measurement error for both the “necessity” and “concerns” subscales. Reliability for the “practical barriers” subscale was fair.
Emotional representations (category 3):
Pain self-efficacy (category 3). Pain self- efficacy (emotional representations) was measured with the Dutch Pain Self Efficacy Questionnaire (PSEQ) (16, 22, 23). The PSEQ asks patients to take the pain into account when rating their self-efficacy in certain activities and tasks grouped within 10 items. Each item was scored on a 7-point scale, ranging from 0 (“not at all confident”) to 6 (“completely confident”). Total scores ranged from 0 to 60, with higher scores indicating stronger self-efficacy beliefs. This instrument has been shown to be valid and reliable (22, 23).
Anxiety and depression (category 3). Anxiety and depression (emotional representations) were measured with the Hospital Anxiety and Depression scale (HADS) (24, 25). The HADS is a valid and reliable 14-item short self-rating screening tool of anxiety (7 items) and depression (7 items), scored on a 4-point Likert scale (0–3) (24, 25). Higher scores on the 2 domains indicate greater levels of depression or anxiety.
Pain catastrophizing (categories 3, 4). Pain catastrophizing (emotional representations and coping procedures for illness and emotion) was assessed with the Dutch version of the Pain Catastrophizing Scale (PCS) (26, 27). Pain catastrophizing can be defined as: “an exaggerated negative mental set brought to bear during actual or anticipated painful experience”. One’s imagination plays a role in anticipating negative outcomes, which results in a cascade of negative cognitive and emotional responses to pain: rumination (“I can’t stop thinking about how much it hurts”), magnification (“I worry that something serious may happen”), and helplessness (“It’s awful and I feel that it overwhelms me”) (26, 27). Patients were asked to reflect on past painful experiences and to indicate whether they experienced one of the 13 thoughts or feelings during pain on a 5-point scale. A PCS total score is calculated by summing the scores for all 13 items; thus, total scores range from 0 to 52. Higher scores correspond to more catastrophizing thoughts. The PCS has been shown to be valid and reliable (26, 27, 39).
Statistical analysis
All analyses were performed with the statistical software package SPSS (version 23) for Windows (IBM SPSS Statistics 23). First, descriptive statistics (frequencies, QQ plots, means and standard deviation (SD)) were computed for all potential predictors to check the quality of the data. To check for multicollinearity, Spearman correlations were calculated between the potential predictors of dropout, and a cut-off score of 0.70 was used (28) (Table SI1). Baseline differences were tested between the dropout group (DG) and the completer group (CG) for demographic and clinical variables derived from the E-CSM of Self-Regulation, with Pearson’s χ2 tests for categorical variables and independent Welch t-tests for continuous variables.
Statistical analyses were carried out in 2 phases. First, exploratory univariate logistic regression analyses were performed on 18 potential predictors (Brief IPQ – 8 items), (TBQ – 3 domains), (PSEQ – total score), (PCS total score and 3 domains) and (HADS –2 domains) to identify predictors of dropout, which could be considered for inclusion in multiple logistic regression analyses. The most significant variables with p-values < 0.20 were considered for inclusion in the multiple logistic regression model. To determine the model that best predicted dropout, a forward stepwise procedure was performed to select the variables that were most significant and had clinical relevance. The number of dropouts (n = 35) found in this study limited the possibilities of including more than 4 variables, as the minimum number of events per variable (EPV) required in multiple logistic regression analyses has been suggested to be at least 10 (29). First the potential predictor with the strongest association was considered for inclusion in multiple logistic regression analyses, followed by the next best one, etc. Estimates of association were presented as odds ratios (ORs), along with 95% confidence intervals (95% CI). The Hosmer-Lemeshow test was performed to assess how well the model fitted the data (28). To describe the discrimination of the model, the area under the receiver operating characteristic (ROC) curve (AUC) was calculated.
Of the 188 included patients 35 (19%) were classified as dropouts, 14 of whom were male (40%) and 21 female (60%). Patients dropped out at different phases of the treatment: 10 dropped out in the diagnostic phase and 25 dropped out in the treatment phase. Overall, there were no statistical differences in age, sex, ethnicity, marital status, work status, ability to work and pain intensity between the DG and the CG (Table I). The mean age of the DG was 47.9 years (SD 9.9), compared with 46.7 years in the CG (SD 12.3); approximately 40% of the DG were male compared with 28% in the CG. Statistically significant differences were found between the DG and the CG in educational level: 11.4% of the DG vs. 3.9% of the CG had a low educational level (p = 0.009). Pain duration was statistically different between the DG and the CG (p = 0.027): 57% of DG had chronic pain for more than 5 years vs. 34% of the CG.
Table I. Participants characteristics of completers and dropouts in a chronic pain rehabilitation programme
Table II shows the baseline scores for the dropouts and the completers on the variables derived from the E-CSM of Self-Regulation. Although some differences were small, the dropouts scored, on average, worse than the completers on almost all of these baseline scores. Statistically significant differences were found for the PCS domain scores; helplessness (p = 0.001), rumination (p = 0.009) and for the PCS total score (p = 0.001). On the PCS the dropouts in our study scored in total a mean (SD) of 27.43 (SD 10.98) vs. completers 20.08 (SD10.59), indicating that the dropouts were significantly more likely to catastrophize than the completers in this study.
Table II. Scores of completers and dropouts on categories of the Extended Common-Sense Model of Self-Regulation
Univariate logistic regression analyses
Illness representations (Brief IPQ – 8 items). Just 1 item of the Brief IPQ was significantly associated with dropout in univariate regression analysis (p = 0.041): Brief IPQ treatment control, covering the illness belief on how much you think your treatment can help your illness (0 not at all, 10 extremely helpful). Lower scores on the Brief IPQ item were associated with dropout (Table SII1).
Treatment beliefs (TBQ – 3 domains). One domain of the TBQ scored below a p-value < 0.20: Practical Barriers (p = 0.072). This domain identified treatment beliefs in relation to practical barriers, such as costs for and availability of public transport. Higher scores on the TBQ Practical Barriers domain were associated with dropout (Table SII1).
Pain self-efficacy (PSEQ – total score). Another potential predictor that scored below a p-value < 0.20 was the total score of the PSEQ (p = 0.063). Lower scores on the PSEQ – total score were associated with dropout (Table SII1).
Anxiety and depression (HADS – 2 domains). No associations with dropout were found for the 2 domains of the HADS: Anxiety (p = 0.735) and Depression (p = 0.444) (Table SII1).
Pain catastrophizing (PCS total score and 3 domains). In univariate logistic regression analyses significant associations with dropout were found for all 3 domains of the PCS: Helplessness (p < 0.001), Magnification (p = 0.034), Rumination (p = 0.009) and the PCS total score (p = 0.001). Higher scores on the all 3 domains of the PCS and the PCS total score were associated with incidence of dropout (Table SII1).
Multiple logistic regression analyses
Based on the univariate logistic regression analyses 7 predictors for dropout of the 18 selected potential predictors (out of four categories of the E-CSM Self-Regulation were eligible for inclusion in the multiple logistic regression analyses. Because the number of dropouts in this prospective cohort study was limited, maximal 3 of the 7 potential predictors could be included in the multiple logistic regression model (29). The Brief IPQ item treatment control was chosen for inclusion above the TBQ domain Practical Barriers, since the psychometric properties of this measurement were better than the TBQ (21). In addition, the PCS total score was preferred to the 3 domains of PCS for multiple logistic regression analyses, as these domains were highly correlated with each other (helplessness, magnification and rumination).
The following 3 potential predictors were included in the multiple logistic regression analysis: IPQ-B treatment control item, PSEQ- total score and PCS total score. Only the PCS total score (p = 0.001) was retained as a predictor for dropout in these analyses. Brief IPQ item treatment control (p = 0.081) and PSEQ- total score (p = 0.770) were not significantly associated with dropout, when adjusted for PCS total score (Table III).
In this IPMP an increase of 1 point on the PCS total score resulted in an 1.1 higher odds of dropping out (95% CI 1.028; 1.1071).
Bootstrapping was performed using the Bias-Corrected and Accelerated (BCa) bootstrap method with 10,000 draws from the data to internally validate the prediction model. This led to a somewhat broader CI: Pain catastrophizing total score (95% CI 1.027; 1.117), but it did confirm the results of the prediction model.
To determine the performance of the prediction model, a parameter of calibration and a parameter of discrimination were calculated (30). For calibration, the Hosmer-Lemeshow test identified a good fit for the model (p = 0.508) (Table III). For discrimination the ROC curve was calculated and its area under the curve (AUC). The AUC for the model was 0.688 (95% CI 0.589; 0.786) (Table III).
Table III. Result of multiple logistic regression analysis of potential predictors for dropout (PCS total score, Brief IPQ item treatment control, PSEQ total score)
The aims of this prospective cohort study were to explore predictors for dropout of patients with chronic musculoskeletal pain during an interdisciplinary pain management programme, and to develop a multivariate model to predict dropout. Based on the conceptual framework of the E-CSM of Self-Regulation 18 potential predictors were investigated for associations with dropout. The results from univariate logistic regression analysis identified 7 potential predictors for dropout eligible for inclusion in multiple logistic regression analyses. Just one of the potential predictors was retained in the multiple logistic regression model; the pain catastrophizing total score.
Relating findings to the literature
Since multivariate prediction models in different studies often contain different predictors and are therefore not comparable, the findings from univariate analyses in our study were compared with results from other studies on dropout in IPMPs.
Although we focused in this prospective cohort study on potential predictors that were derived from the E-CSM of Self-Regulation, it is also important to reflect on differences on other sociodemographic baseline items between the dropouts (DG) and the program-completers (CG). This study found significant differences between the DG and the CG in educational level: there were more patients with low educational levels in the DG vs. the CG. Despite the fact that the findings of our systematic review revealed no significant results for educational level as a predictor for dropout in IPMPs (5), the findings of our qualitative study indicated that it is important to take educational level into account1. This study on health literacy in IPMPs emphasizes that to engage patients with low health literacy levels (which is strongly associated with low educational levels) a more tailored IPMP is needed for patients to make sense of health information in pain neuro-science education1. Further research in other pain management programmes should reveal whether participants with low educational levels (low health literacy levels) are more prone to dropout.
1Oosterhaven J, Wittink H, Pell CD, Schröder CD, Popma H, Spierenburg L, Devillé W. Health literacy and pain neuro education: a qualitative study on patient perspectives. 2019. Manuscript submitted for publication.
Pain duration may be considered as an important potential predictor for dropout based on the results of the current study: we found a greater proportion of participants with chronic pain for more than 5 years in the DG than the CG. To date, pain duration has not been investigated for an association with dropout in other interdisciplinary pain management programmes. However, our systematic review identified length of disability and duration of work disability as predictors for dropout (5). Pain duration is related to length of disability; therefore this could be an interesting potential predictor for dropout for future research.
All dropouts scored worse on all items of the brief IPQ and the TBQ. Just 2 items were eligible for inclusion in the multivariate logistic regression analyses: the Brief IPQ treatment control item and the item practical barriers of the TBQ. Although in a recently published meta-analysis (31) questions were raised with regard to the predictive capacity of the E-CSM of Self-Regulation in association with outcomes, our study indicates that it may be important to consider patients’ views regarding their treatment at baseline in association with dropout. This is line with recommendations from 2 studies on dropout in the mental health literature, which emphasized the importance of the identification of patients’ treatment expectations at the start of the treatment (32, 33). Further research should focus on confirmation and external validation to confirm whether these beliefs are important potential predictors for dropout.
Our finding that patients who had lower scores on the PSEQ total score, were more likely to dropout from this interdisciplinary pain management programme, was similar to the findings from a retrospective cohort study in an inpatient interdisciplinary pain programme (4). A meta-analysis revealed self-efficacy as a key influence on chronic pain outcomes, and it is identified as an important risk and protective factor for functioning in patients with chronic pain (34). Thus, we suggest that pain self-efficacy (as measured with the PSEQ) be taken into account in practice in IPMPs. Additional research is needed to investigate whether pain self-efficacy is an important predictor for dropout in IPMPs.
With regard to anxiety and depression, our results contrasted with findings from other research. Howard et al. (35) found significant associations with dropout for anxiety and depression, which we could not confirm with our study. This disparity may be caused by the inclusion of patients with more severe levels of anxiety and depression in the study of Howard et al. (35), who might have been excluded from our prospective cohort study. Another explanation may be found in differences in the instruments used in both studies. In the current study, the HADS was used to measure anxiety and depression, while the structural clinical interview for DSM-IV (SCID) and the Beck Depression Inventory (BDI) were used in the study of Howard et al. (35). The HADS differs from the SCID and the BDI in not including items regarding somatic and physical functioning. Taking into account the considerable overlap between the somatic symptoms of depression and chronic pain, research has suggested that the BDI may overestimate the occurrence of depression in patients with chronic pain (36, 37). In light of this, further research with validated instruments for anxiety and depression in patients with chronic pain may reveal whether these are associated with dropout.
This study demonstrated that pain catastrophizing was the main predictor of dropout in this IPMP. How-ever, one other study that investigated catastrophizing as a predictor for dropout in an IPMP did not find significant results (4). In Coughlan et al.’s study (4) pain catastrophizing was measured with a subscale of the Coping Strategies Questionnaire (these are the same items as the helplessness domain of the PCS) not with the PCS. In our study pain catastrophizing was operationalized as a multidimensional concept and includes 3 domains: helplessness, rumination, and magnification.
In this IPMP all completers showed significant improvement on all domains of the PCS. The dropouts scored significantly higher than the completers on all 3 domains of the PCS and for the PCS total score at the baseline assessments. No statistical analyses could be performed post-treatment for the dropouts, since only 6 of the 35 dropouts participated in these assessments. The literature provides different cut-off points for pain catastrophizing; above 23 and above 30 (38). The dropouts in our study scored 27.23 vs. completers 20.08, indicating that the dropouts were more likely to catastrophize than were the completers.
Pain catastrophizing
In the last 3 decades, pain catastrophizing has emerged as an important construct in the field of pain. It plays a role in the response to pain and in pain-related disability, and is a moderator of treatment outcomes (38). This study has identified pain catastrophizing as a potentially important variable in the prediction of dropout in IPMPs. Patients with higher pain catastrophizing scores, approaching the clinical relevance cut-off of 30 (scores around 27, the mean in this study) may need further follow-up by their clinicians to determine whether these patients are prone to dropout. Strategies can be developed to prevent early dropout from treatment and in order to tailor pain interventions to patients who are prone to dropout. Additional research is needed to investigate whether pain catastrophizing is an important construct to unravel with regard to dropout in IPMPs.
Strengths and limitations
A strength of this study is that it is one of the few prospective cohort studies on the topic of dropout in IPMPs (3, 35, 39). A further strength is that the development of the prediction model was based on a conceptual framework, the E-CSM of Self-Regulation. However, due to the small sample size and the exploratory nature of this study no firm conclusions could be drawn on the predictive value of the E-CSM of Self-Regulation for dropout in IPMPs.
In addition, the prediction model we developed was internally validated and was considered “good”. Bootstrap results confirmed those from multiple logistic regression analyses and identified a relatively low bias. Furthermore, the performance of the prediction model was also good, taking into account the calibration parameter (the good fit of the model being identified with the Hosmer-Lemeshow test) and the discrimination parameter (considering the AUC curve).
This prospective cohort study has some limitations that must be taken into consideration in interpreting the results. First, the study focused on the development of a multivariate prediction model for dropout, a type 1b study according to the TRIPOD statement (40). Due to the exploratory nature of the study, a relatively small dropout sample (35 dropouts), and to avoid “fishing” and the risk of “overfitting”, only one multivariate prediction model for dropout was fitted, which resulted in one predictor for dropout: pain catastrophizing. With regard to the small sample size, a forward method was applied to select the most significant and clinically relevant potential predictors for the multiple logistic regression model. A maximum of 3 out of 7 potential predictors was required in our model (29). We therefore elected not to perform a backward stepwise selection procedure, since this would entail initially entering all 7 predictors. Although efforts were made to evaluate the performance of our prediction model (with a description of the calibration and the discrimination of the model), the clinical usefulness still has to be identified. In other words, the question arises as to whether the prediction model for dropout informs healthcare providers in their decision-making to prevent dropout in IPMPs. Nonetheless, future research should first focus on confirmation and external validation of the findings of this study in larger samples and may reveal whether other predictors are involved.
In this study only reliable and valid measurements used in daily practice were chosen. However, one might criticize the instruments used to operationalize the E-CSM of Self-Regulation. Research has shown that the emotion part of the E-CSM Self-Regulation is less investigated. The Brief IPQ, the PSEQ, the TBQ and the PCS, used in this study to operationalize the emotional representations, may not be the most ideal instruments to measure emotions such as anger, shame, happiness/joy, depression/sadness and fear/anxiety (41).
In addition, the conceptual overlap between the psychological concepts and measurements with regard to chronic pain might have hindered the efficient measurement of the E-CSM of Self-Regulation. Research has shown that catastrophizing overlaps with depression, anxiety, distress and self-efficacy (36). Another study has revealed that catastrophizing may be viewed as a subdomain of an overarching construct, such as emotional distress. In this view emotional distress is measured indirectly by the persons’ experience of pain (catastrophizing, emotional reactions and kinesio-phobia) and the persons’ self-view (pain self-efficacy) and directly by anxiety and depression (36, 41). This prospective cohort study could only find evidence for an association of indirect measures for emotional distress, such as pain self-efficacy and pain catastrophizing with dropout in this IPMP.
Conclusion
To our knowledge this is the first study to investigate the E-CSM of Self-Regulation as a conceptual framework for the prediction of dropout in IPMPs. Multiple regression analyses revealed that patients with chronic pain who catastrophize were more prone to dropout from this chronic pain management programme. However, due to the small sample size and the exploratory nature of this study no firm conclusions can be drawn about the predictive value of the E-CSM of Self-Regulation for dropout in interdisciplinary pain management. Future research should focus on confirmation and external validation of the findings of this study.
The authors thank all patients who supported the study, Josca Snoei, Willemien Wiersma, Irene Koss and Hans Popma from the Rehabilitation Centre of Heliomare, Wijk aan Zee for their help with the initial construction of this prospective cohort study. Thanks to Les Hearn (Scientific Editing and Proofreading: les_hearn@yahoo.co.uk).
Funding sources. This study is supported by grants of the Dutch government- NWO- 023.004.121 and SIA Raak 2012-14-12P.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize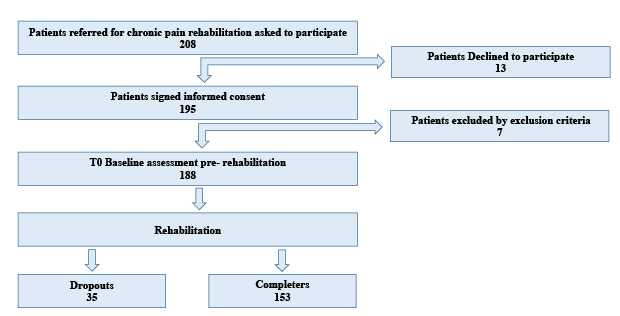 Click to show fullsize
Click to show fullsize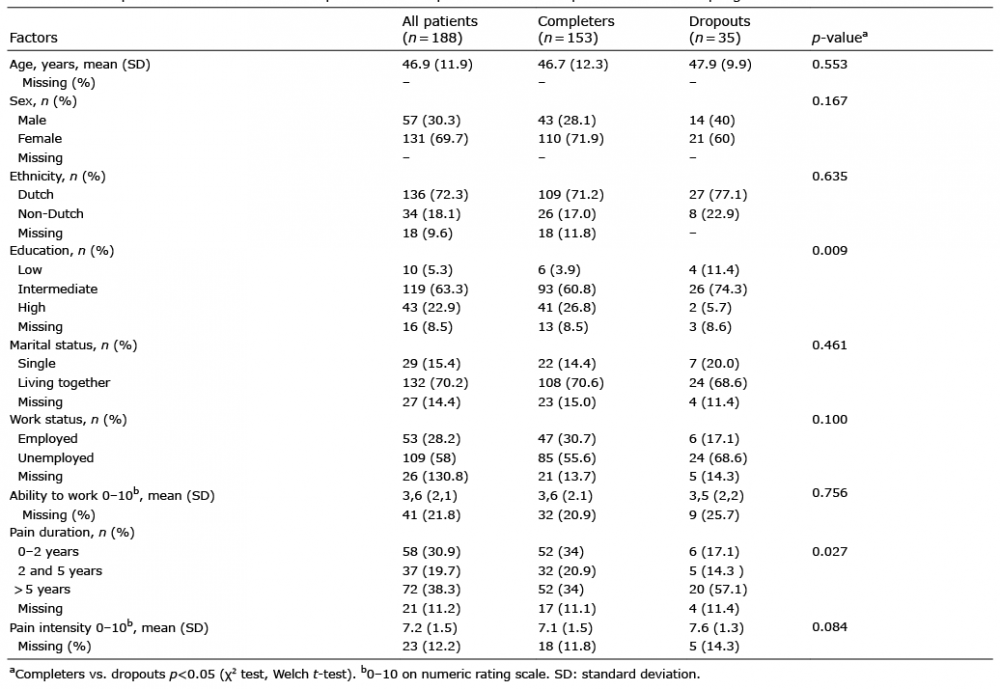 Click to show fullsize
Click to show fullsize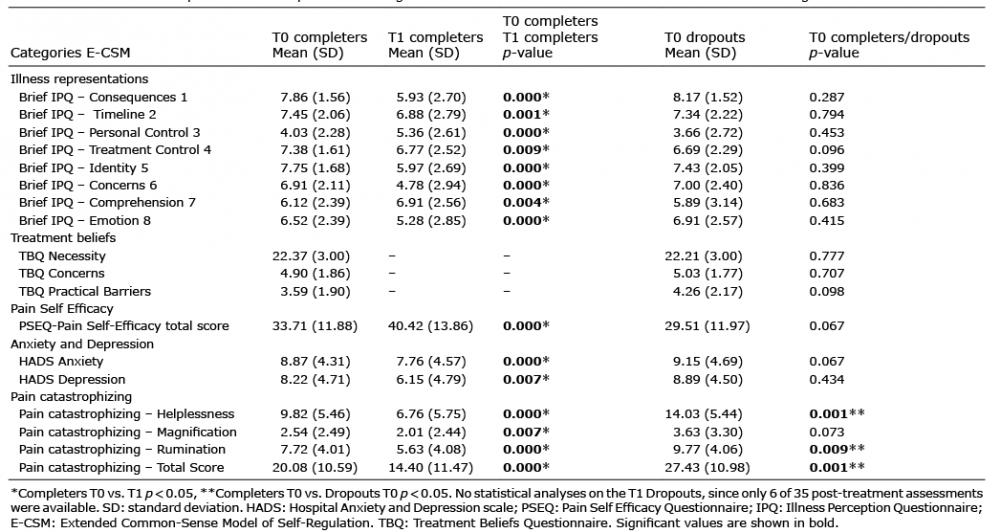 Click to show fullsize
Click to show fullsize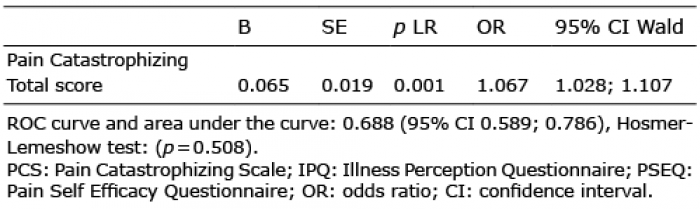 Click to show fullsize
Click to show fullsize