
From the 1Department of Orthopaedics, University of Szeged, Szeged, Hungary, 2The Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust, UK and 3The Orthopaedic Research Institute, Bournemouth University, Bournemouth, UK
Objective: To establish whether attendance at an education class prior to total hip or knee replacement surgery as part of an enhanced recovery after surgery pathway could decrease length of hospital stay.
Methods: A single-site, retrospective cohort study comparing length of stay in hospital for patients who attended and did not attend an education class prior to hip or knee replacement surgery. Patients were stratified into 3 groups according to the predicted likelihood of an extended inpatient hospital stay using the Risk Assessment and Predictor Tool.
Results: Mean length of stay reduced by 0.37 days for patients who received hip replacement (n = 590) (95% confidence interval (95% CI) –0.74, –0.01, p = 0.05) and by 0.77 days for patients who underwent knee replacement (n = 643) (95% CI –1.23, –0.31, p = 0.001) following attendance at a preoperative education class. Patients undergoing knee replacement who were considered at high risk of an extended hospital stay stayed a mean of 2.59 days less in hospital after attending the class (mean length of stay: 4.52 (standard deviation (SD) 1.26) vs 7.11 (SD 4.18) days (95% CI –4.62, –0.54, p < 0.02).
Conclusion: This study supports the inclusion of a preoperative education session in this context for both hip and knee replacement procedures, and indicates that this may be most beneficial for patients undergoing knee replacement who are at risk of an extended length of stay.
Key words: arthroplasty, replacement, hip; arthroplasty, replacement, knee; preoperative care; education; enhanced recovery after surgery.
Accepted Sep 2, 2019; Epub ahead of print Sep 12, 2019
J Rehabil Med 2019; 51: 788–796
Correspondence address: Thomas Wainwright, Orthopaedic Research Institute, Bournemouth University, 89 Holdenhurst Road, Bournemouth, BH8 8EB, UK. E-mail: twainwright@bournemouth.ac.uk
The aim of this study was to compare length of stay in hospital between patients who attended an education class prior to elective total hip or knee replacement surgery, and those who did not attend. A further aim was to establish which patients would benefit most from a preoperative education class, using the Risk Assessment and Predictor Tool. The study showed that patients who attended the class spent 0.38 days less in hospital following hip replacement, and 0.77 days less following knee replacement surgery. Patients undergoing knee replacement who were considered at high risk of an extended hospital stay spent a mean of 2.58 days less in hospital after attending the class. These results support the inclusion of a preoperative education class in this context for both hip and knee replacement procedures, and indicate that this may be most beneficial for patients undergoing knee replacement.
The volume of total hip and knee replacement surgeries occurring annually in the United Kingdom (UK) for the treatment of end-stage degenerative joint disease continues to grow linearly with the ageing population (1). The application of enhanced recovery after surgery (ERAS) (also termed fast-track) programmes, a multidisciplinary approach to patient care (2), combined with the improvement of surgical techniques and better pain management, has improved postoperative outcomes (3, 4). In addition, the influence that psychological factors may have on recovery from joint replacement surgery has become increasingly recognized (5, 6). Patients affected by osteoarthritis may experience worse symptoms in terms of mental health, including anxiety and depression (7, 8). Optimizing the psychological status of patients pre-surgery through education is recommended by the ERAS Society (9); however, current literature is contradictory regarding the effect of preoperative education on length of stay. Although some studies have shown improvement in length of stay with the use of a preoperative education class (10, 11), the majority of the current evidence base does not support the inclusion of routine (non-selective) psychological or educational intervention in total hip or knee replacement pathways (12–15).
Orthopaedic surgeons have a pivotal role in transitioning the care of their patients from a biomedical to a biopsychosocial model; however, they may not always formally screen patients, and therefore refer for psychological treatment (16). Therefore, it may be that attendance at a preoperative education session could improve outcomes for some patients by inducing feelings of control and empowering patients to undertake positive health behaviours prior to admission to hospital. Although reported to have no effect on postoperative pain (17), there is evidence that preoperative education can attenuate anxiety (18, 19), encourage compliance with physiotherapy (20) and increase self-esteem (19), and may be most beneficial to high-risk patients, presenting with co-morbidities or impaired mental health as part of a targeted prehabilitation programme. The primary aim of the current study was to compare length of stay between patients who attended an education class prior to elective total hip or knee replacement surgery, and those who did not attend. The secondary aim was to establish which patients would benefit the most from a preoperative education class, using the Risk Assessment and Predictor Tool (RAPT) (21).
This is a single-site, retrospective cohort study, reported in accordance with the Reporting of Studies using Observational Routinely-collected Data (RECORD) statement (22). Patients were retrospectively, consecutively recruited between 27 July 2010 and 4 November 2011 from the Royal Bournemouth Hospital, Bournemouth, UK. Patients were considered eligible for inclusion if they had undergone elective total hip replacement or total knee replacement surgery. All patients were enrolled onto a standardised and previously published ERAS pathway (23), which included: a comprehensive preoperative assessment process, patient education, discharge planning, admission to hospital on the day of surgery, a default anaesthetic technique, effective pain management, and twice-daily physiotherapy until discharge (23). All hip replacements were performed using the posterior approach, whilst all knee replacements were carried out using the medial parapatellar approach. Revision cases and re-admitted patients were excluded from the study.
Outcome measures and data collection
The primary outcome measures were: (i) length of hospital stay; and (ii) attendance at the preoperative education class, collected retrospectively. Attendance at the preoperative education class was recorded routinely on an attendance register prior to admission. Length of hospital stay was recorded routinely on the day of discharge as the number of days between hospital admission and discharge home. The 2 outcome measures were compared in order to establish if there was a relationship between attending a preoperative education class and the time spent in hospital following surgery. The discharge criteria following total hip replacement at the Royal Bournemouth Hospital includes: (i) being able to safely walk independently around the ward either with crutches or with walking sticks; (ii) being able to stair climb; being able to get on and off a bed, chair and toilet independently; (iii) dry wound (with no significant discharge), showing signs of healing; (iv) satisfactory blood results and X-ray; (v) controlled pain; and (vi) being medically fit.
The RAPT questionnaire was originally designed to identify a patient’s risk of needing extended inpatient rehabilitation following total hip or knee replacement (21) and was included within the current study to compare outcomes between different groups of patients. At the education session, all patients were asked to complete a RAPT questionnaire (Appendix I) to aid the therapists’ discharge planning (21). If patients did not attend their education session, the RAPT was completed on the day of surgery. Scores were categorized into red (high-risk of needing extended inpatient rehabilitation services, score <6), amber (medium-risk of needing extended inpatient rehabilitation, score 6–9) and green (low-risk of needing extended inpatient rehabilitation, score >9) (21), and then compared with length of stay and class attendance data.
Data access
Data were accessed through the hospital’s online administrative system. The researchers were granted access as they all held professional positions at the Royal Bournemouth Hospital at the time of data collection.
Preoperative education
Following a phone call to arrange their operation date, all patients received a letter with specific instructions to attend a preoperative education class. The session was delivered within 2 weeks of the date of surgery, by a physiotherapist, occupational therapist and nurse, who all worked on the ward where the ERAS programme was delivered. The personnel delivering the class were regularly rotated and all new staff were trained to deliver the content. The aims of the 1-h session were: (i) to reduce anxiety; and (ii) to provide a detailed explanation of the pathway. Patients were encouraged to ask questions and bring carers so that their expectations could also be managed. Education topics included: what to bring and how to prepare preoperatively, exercises to start before the operation, post-operative pain control and anaesthetic protocols. The patients were also given the opportunity to practice walking with crutches, and to discuss any equipment they required for their return home (23). All patients were given a series of knee range of movement and quadriceps-strengthening exercises (Appendix II) preoperatively and were instructed to complete these 3 times a day.
Non-attendance at preoperative education
Regardless of whether the patient attended the preoperative education class, all patients received an education booklet at pre-assessment when they were listed for surgery and there were no other differences in treatment pathways. The booklet included advice on protection, rest, ice, compression and elevation (PRICE) principles to help manage postoperative pain and swelling. All patients had standardized inpatient physiotherapy and occupational therapy postoperatively until they met the joint-specific discharge criteria and were discharged from hospital.
Sample size
No formal power analysis was performed. The initial 15-month period of the implementation of a modified ERAS pathway (23) was chosen as study interval, between July 2010 and November 2011 to allow for a minimum of 1,200 consecutive cases.
Statistical analysis
The data were analysed using IBM SPSS Statistics 19. The normality of the data was tested using the Shapiro–Wilk test, and a 2-sample t-test was used to detect if there was a statistically significant relationship between attending a preoperative education class and length of hospital stay following total hip and knee replacement surgery. Patients who did or did not attend the pre-operative group, based on 3 sub-categories for each group of RAPT (red, amber and green), were compared using the Kruskal–Wallis test to establish if the score was evenly distributed. A p-value of 0.36 showed that the samples came from the same population. All data were analysed at a level of statistical significance of 0.05 and a power of 0.95.
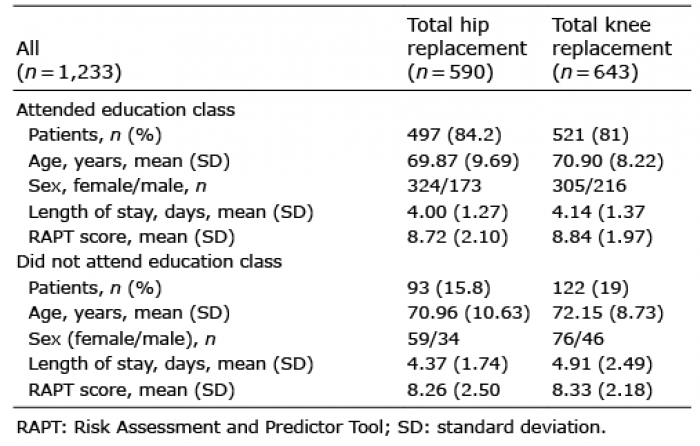
Table I presents mean data from 1,233 patients with elective total hip or knee replacement, sourced from the hospital database. A total of 1,018 patients (82.5%) attended their preoperative education session (hip replacement: 497 (84.2%), knee replacement: 521 (81%)) and 215 (17.5%) did not attend (hip replacement: 93 (15.8%), knee replacement: 122 (19%)). The mean time between the education class and surgery was 7.1 days (range 2–21 days). Mean length of stay was reduced by 0.37 days for patients who had received total hip replacement surgery (95% CI –0.74, –0.01, p = 0.05) and by 0.77 days for patients who had undergone total knee replacement (95% CI –1.23, –0.31, p = 0.001) following attendance at a 1-h preoperative education class.
Table I. Characteristics and length of stay for patients who underwent total hip and knee replacement between 27 July 2010 and 04 November 2011
Total hip replacement
There were no statistically significant differences in mean length of stay between patients undergoing hip replacement who did and did not attend their preoperative education class when data were categorized into red, amber and green RAPT scores (Table II).
Total knee replacement
Patients who received total knee replacement with a red RAPT score and attended the preoperative education class stayed a mean of 2.59 days less in hospital than those who did not attend (mean length of stay 4.52 (SD 1.26) vs 7.11 days (SD 4.18) (95% CI –4.62, –0.54, p < 0.02). Patients with an amber RAPT score who attended the preoperative education class stayed 0.56 days less in hospital than those who did not attend (mean length of stay 4.34 (SD 1.46) vs 4.90 days (SD 1.99) (95% CI –1.10, –0.03, p < 0.04). However, there were no significant differences between patients who attended and did not attend the class with a green RAPT score (Table II).
Table II. Attendance at class, mean length of stay and RAPT scores for hip and knee replacement
This retrospective analysis demonstrates a general reduction in mean length of stay for patients undergoing total hip and knee replacement surgery who attended a preoperative education class, compared with those who did not. The benefits were greatest for patients presenting with a high or medium risk of needing extended inpatient rehabilitation, as classified by RAPT score, and were more clinically significant for patients at high risk and who received knee replacement surgery. Other factors previously reported to contribute to differences in length of stay are: age, use of preoperative walking aid, anaemia, diabetes, hypertension, use of anticoagulants, cardiopulmonary disease, and psychiatric disease (24–27).
The results of the current study are similar to those of Yoon et al. (10), whereby patients who attended an education session experienced a significantly shorter length of stay than non-participants for both total hip replacement (3.1 (SD 0.9) vs 3.9 days (SD 1.4); p = 0.001) and total knee replacement (3.1 (SD 0.9) vs 4.1 days (SD 1.9); p = 0.001). However, Yoon et al.’s study included a much smaller number of patients (n = 261 vs 1,233 in the current study) over a similar time period, with a much higher rate of non-participation (36% vs 17.5%). Similarly, in a study on patients undergoing primary and revision knee replacement (11), implementation of an education session led to a reduction in length of stay from 7 days to 5 days (p < 0.01). However, the current study differs in that it evaluates attendees and non-attendees, and is not a before and after comparison.
The RAPT questionnaire was originally designed to identify a patient’s risk of needing extended inpatient rehabilitation following total hip or knee replacement (21). Seven risk factors related to discharge were recognized as: age, sex, preoperative walking distance, preoperative gait aid, community support, the presence of a caregiver on return home, and patient expectation (21). Patient expectation was found to significantly impact outcome, but was considered unstable due to a range of influences, including patient and caregiver’s perceptions of efficacy, and was therefore removed from the final RAPT model (21). Recommendations were given to discuss patient expectations during preadmission assessment to help clinicians and patients mutually agree a discharge plan (21). Therefore, it is possible that the significant reduction in length of stay between RAPT- graded high-risk patients who did and did not attend a preoperative education class was due to altered patient expectations. The specific aims of the session were to reduce anxiety and provide a detailed explanation of the pathway to both patients and their carers (23), since procedure-related uncertainty in addition to unrealistic expectations of outcome can contribute to anxiety and negatively affect postoperative recovery (28). Anxiety is adaptive in motivating behaviour that helps patients to cope with threatening situations, such as surgery, and, as feelings of control encourage anxiety to become facilitative, it is important that a patient receives sufficient information in order to improve their coping ability. The amount of information required to be facilitative is patient-dependent (18) and therefore personalizing preoperative education to complement the patient’s RAPT score, or other preoperative risk screening tools, can help to manage patient expectations.
Furthermore, adequate screening of physiological and cognitive reserves in patients scheduled for surgery can identify those who are elderly, isolated, or functionally impaired preoperatively and enable proactive perioperative management strategies to reduce adverse postoperative outcomes or readmission (29). During the education class, patients were encouraged to discuss any equipment they required for their return home (23). Subsequently, appropriate discharge arrangements could be made preoperatively in order to facilitate the return home. For example, where community support or additional care was lacking, home health services could be arranged. Failure to attend the class may have resulted in the communication of needs occurring post-operatively, which could delay discharge. Given that outpatient or day-case surgery is now possible for hip and knee replacement procedures (30), healthcare professionals may have less time to identify patients who require additional support. Therefore, attendance at a preoperative education class is important to facilitate the management of high-risk patients.
The results of the current study demonstrate a significant reduction in length of stay for high-risk total knee replacement patients who attended their preoperative education class; however, the effect within the cohort of patients undergoing hip replacement was non-significant. These results are consistent with the wider literature, since, although the 2 procedures are regularly investigated together, they are different procedures and there is a difference in the “success” rate of hip and knee replacements (31). Total hip replacement is considered highly successful, with very good long-term results (32); however, there is evidence that reports patient dissatisfaction (33, 34) and a prolonged recovery in the early and intermediate postoperative period following knee replacement surgery (35, 36). Patients have reported feeling “unsafe” undergoing total knee replacement on an outpatient basis (37), and there are differences in the characteristics of the population that develop knee and hip osteoarthritis, which may affect the psychological status of a patient (31). For example, a high body mass index is often correlated with the development and progression of osteoarthritis of the knee, but not of the hip (38), and obesity has been linked to an increased psychological burden (39). Impaired psychological health, uncertain expectations of surgery and fear of the operation are reported to affect decision-making regarding knee replacement (31), and therefore patients on the waiting list may catastrophize or engage in negative health behaviours. Fortunately, negative thoughts are susceptible to change and can be reframed using cognitive-restructuring techniques, and therefore, high-risk patients undergoing knee replacement may have the most to gain from attending a preoperative education class, as suggested by the results of the current study. Adopting a biopsychological model in education, which focuses on the complex interaction between psychological, social and biological factors that contribute to health problems can help patients to understand the thoughts and feelings that influence their behaviours (40). Therefore, incorporating cognitive-behavioural approaches into the preoperative class may provide additional benefits to high-risk patients undergoing hip or knee replacement surgery (41).
Retrospective analyses are limited by threats to both internal and external validity (42). As the current study utilized existing clinical data, data collection was secondary and therefore lacks reliability. In addition, the current study is limited by the fact that both patient groups received a procedure-specific information booklet containing information that is also covered in the education class. This may have produced a smaller effect size than if the comparison group received no preoperative education at all. Likewise, the standardized discharge arrangements used in the ERAS pathway (23) may have limited between-group variations.
In conclusion, this study highlights that the inclusion of a preoperative education session in an ERAS path-way may be most beneficial for patients undergoing knee replacement, and who are identified as being at high risk of an extended length of stay. Future work should focus on identifying high-risk patients and subsequently personalizing their education class to meet their biopsychosocial needs.
Appendix I. Risk Assessment and Predictor Tool (RAPT) questionnaire.
Appendix 2. Physiothearapy exercises.
Appendix II. Cont.
Appendix II. Cont.


 Click to show fullsize
Click to show fullsize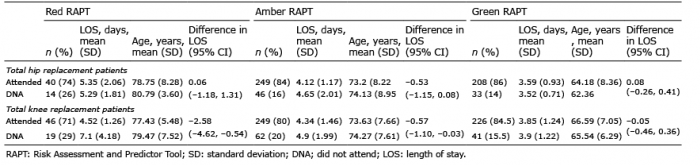 Click to show fullsize
Click to show fullsize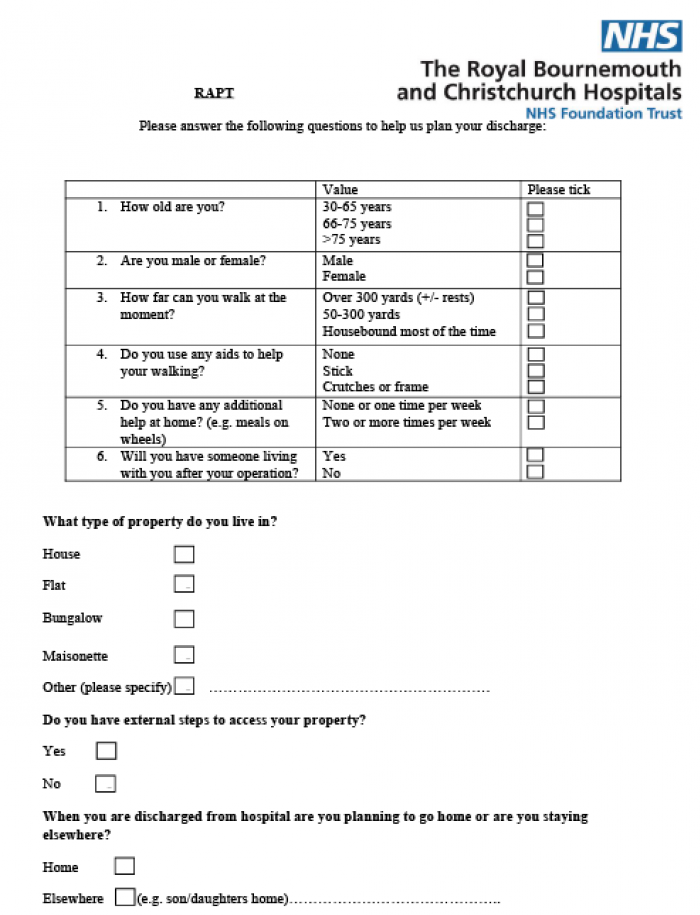 Click to show fullsize
Click to show fullsize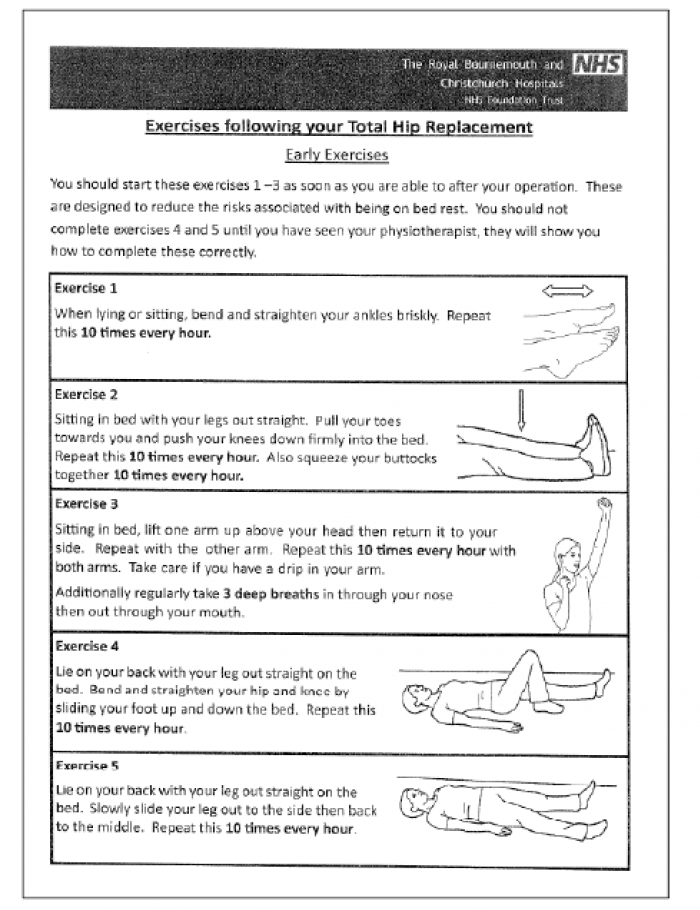 Click to show fullsize
Click to show fullsize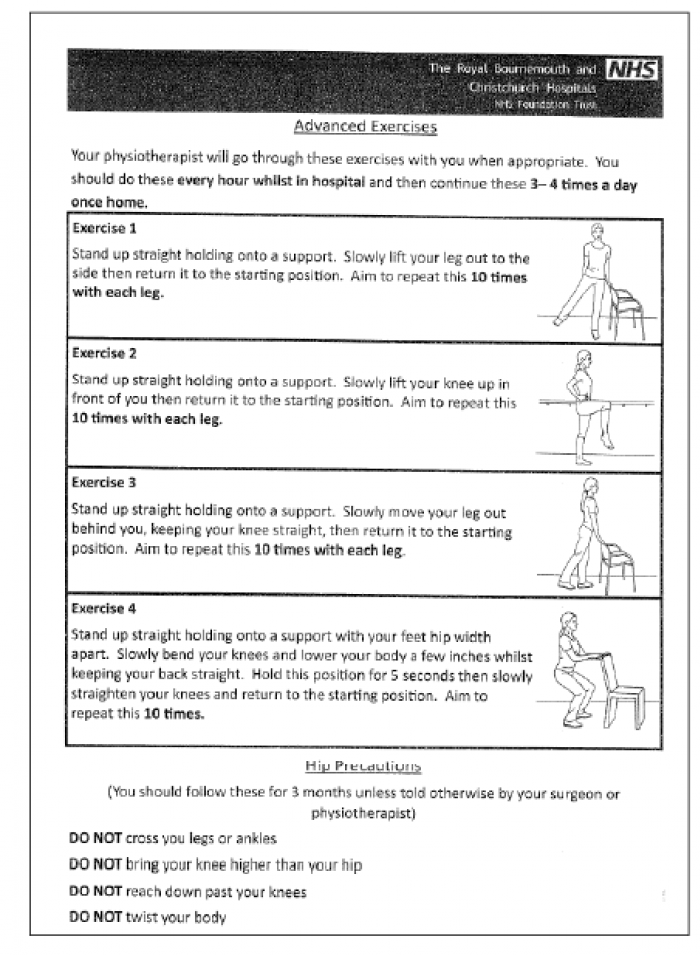 Click to show fullsize
Click to show fullsize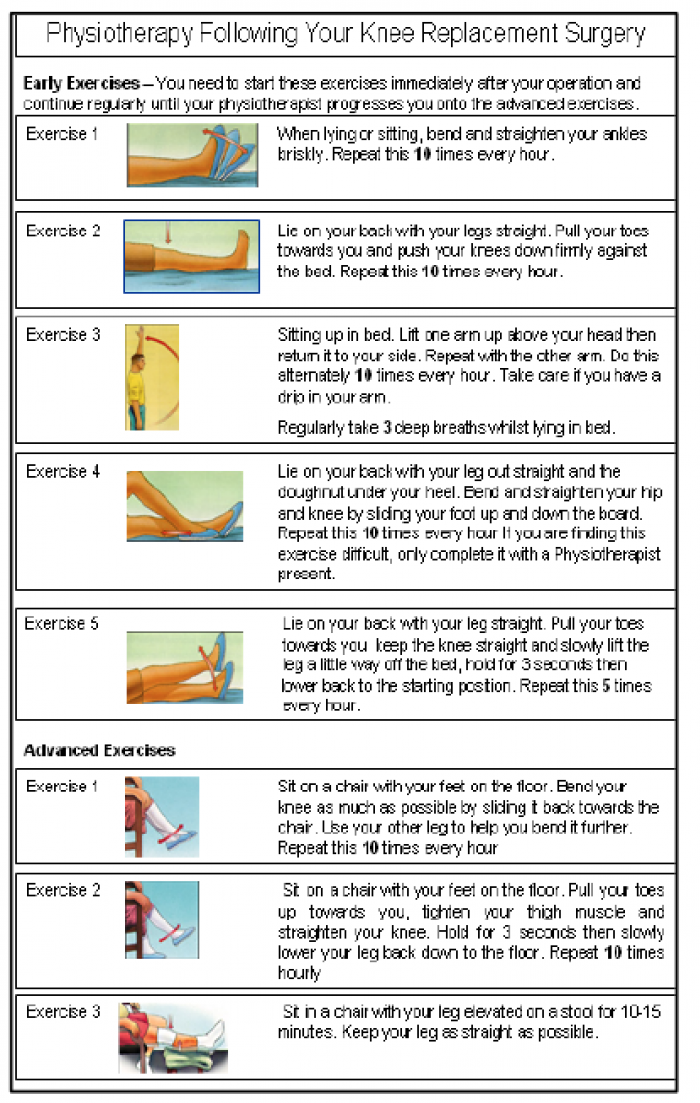 Click to show fullsize
Click to show fullsize