
From the 1Division of Exercise Science and Sports Medicine, Department of Human Biology, Faculty of Health Science, FIMS International Collaborating Centre of Sports Medicine, 2Clinical Research Centre, University of Cape Town and 3Department of Sports Management, Cape Peninsula University of Technology, Cape Town, Western Cape, South Africa
Objectives: To evaluate the effectiveness of over-ground robotic locomotor training in individuals with spinal cord injuries with regard to walking performance, cardiovascular demands, secondary health complications and user-satisfaction.
Data sources: PubMed, Cochrane, Web of Science, Scopus, EBSCOhost and Engineering Village.
Study selection: Trials in which robotic locomotor training was used for a minimum of 3 participants with spinal cord injury.
Data extraction: Independent extraction of data by 2 reviewers using a pre-established data abstraction table. Quality of evidence assessed using Grading of Recommendations, Assessment, Development and Evaluation (GRADE).
Data synthesis: Total of 27 non-controlled studies representing 308 participants. Most studies showed decreases in exertion ratings, pain and spasticity and reported positive well-being post-intervention. Seven studies were included in meta-analyses on walking performance, showing significant improvements post-intervention (p < 0.05), with pooled effects for the 6-min walking test and 10-metre walking test of–0.94 (95% confidence interval (95% CI) –1.53,–0.36) and –1.22 (95% CI –1.87,–0.57), respectively. The Timed Up and Go Test showed a positive pooled effect of 0.74 (95% CI 0.36, 1.11). Improvements in walking parameters were seen with an increase in session number; however, no significant cardiovascular changes were found over time.
Conclusion: Robotic locomotor training shows promise as a tool for improving neurological rehabilitation; however, there is limited evidence regarding its training benefits. Further high-powered, randomized controlled trials, with homogenous samples, are required to investigate these effects.
Key words: spinal cord injury; over-ground robotic locomotor training; exoskeleton device; exercise therapy; gait; blood pressure; muscle spasticity; pain.
Accepted Aug 30, 2019; Epub ahead of print Sep 11, 2019
J Rehabil Med 2019; 51: 00–00
Correspondence address: Yumna Albertus, Division of Exercise Science & Sports Medicine Division, University of Cape Town, Boundary Road, Newlands, Cape Town, South Africa. E-mail: yumna.albertus@uct.ac.za
The benefits of using robotic suits for rehabilitation in patients with spinal cord injury have been tested in many studies. This review assessed the findings of these studies with regards to how over-ground robotic training could improve walking parameters, cardiovascular fitness and health outcomes for people with spinal cord injuries. Twenty-seven studies met the inclusion criteria for an in-depth analysis. The results showed that walking parameters were improved after the training interventions, but that there were no changes in cardiovascular outcomes. Health outcomes, including pain and muscle spasms, decreased after the intervention. This highlights that robotic walking has the potential to advance care for patients with spinal cord injuries by improving walking capacity, reducing pain and muscle tightness, and improving psychological well-being. However, the available evidence could be enhanced by further research using larger sample sizes, randomized control designs, sensitive interventions and tests.
Spinal cord injury (SCI) is a devastating and life-altering condition. The primary neurological effects can lead to serious disability by impacting on physical functioning and independence and increasing the risk of secondary complications associated with a lack of weight-bearing activity (1). Secondary complications include osteoporosis, cardiovascular disease, spasticity, pain, pressure ulcers and depression (1, 2). In order to combat the negative health outcomes associated with SCI and to improve daily independence and social reintegration, recovery of locomotion and functional ability is a top priority for individuals with SCI (3). SCI rehabilitation should not focus primarily on compensation for impairment, but also on maximizing the individual’s potential for recovery through neuroplasticity changes in the central nervous system (CNS). Retraining of motor function and recovery via neuroplasticity is the focus of recently developed locomotor training techniques, which involve the use of wearable robotic exoskeletons (3, 4). The first widely adopted powered exoskeleton, the Lokomat (Hocoma, Switzerland), is a fixed exoskeleton suspended over a treadmill. Robot-assisted technology has advanced in recent years to move away from body-weight supported treadmill training (BWSTT) to over-ground powered lower limb exoskeletons, including Ekso (Ekso Bionics, Richmond, CA, USA) and ReWalk (ReWalk Robotics Inc., Marlborough, MA, USA) (5–8). These lightweight exoskeletons are rechargeable bionic devices with motorized joints that are worn over the lower extremities (4). They enable individuals with lower extremity weakness to stand up and walk with a natural, full weight-bearing, and reciprocal gait (3).
Several studies have investigated the benefits and safety of using powered robotic exoskeletons as a newly developed technology within SCI rehabilitation. However, these studies consist primarily of case-series or single-intervention trials, all with short intervention periods (5, 9). Several systematic reviews exist on the effectiveness of various forms of locomotor training after SCI, including over-ground and treadmill-based training, hybrid exoskeletons and orthotic walking aids (5, 9, 10). These reviews consider ambulatory function and safety as primary concerns, while user-satisfaction and other secondary health benefits are seldom reported. To our knowledge, no reviews have analysed cardiovascular outcomes from robotic locomotor training (RLT) interventions. Despite the depth of reviews covering RLT, to date, only a single review by Miller et al. (9) has performed a meta-analysis of the effect of over-ground RLT on functional and health outcomes.
Therefore, this systematic review aims to add to the growing field of interest and development surrounding RLT by updating and building on the quantitative results previously established by Miller et al. (9). In addition, with a larger amount of literature available on this topic, a comprehensive overview of all the available evidence is essential to support the clinical application of RLT for rehabilitation after SCI. Consequently, this review aims to examine the effectiveness of over-ground powered exoskeletons as a tool for SCI rehabilitation by investigating gait parameters, cardiovascular demands, secondary health outcomes, including spasticity, pain and user-satisfaction.
Search strategy
A comprehensive review of the existing literature was undertaken using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The following 6 electronic databases were searched for peer-reviewed journals published in English before 3 April 2018: PubMed, Cochrane Library, Web of Science, Scopus, EBSCOhost (CINAHL and Health Source Nursing/Academic) and EI Compedex Engineering Village. There was no limitation on included publication years, considering that the over-ground robotic exoskeletons did not receive USA Food & Drug Admministration/European Commision (FDA/CE) approval pre-2012. The PICOs framework was used to refine the search to individuals with SCI involved in over-ground locomotor training using robotic exoskeleton devices. The search terms included a combination of MeSH keywords and free-text terms (Table SI1).
Study selection
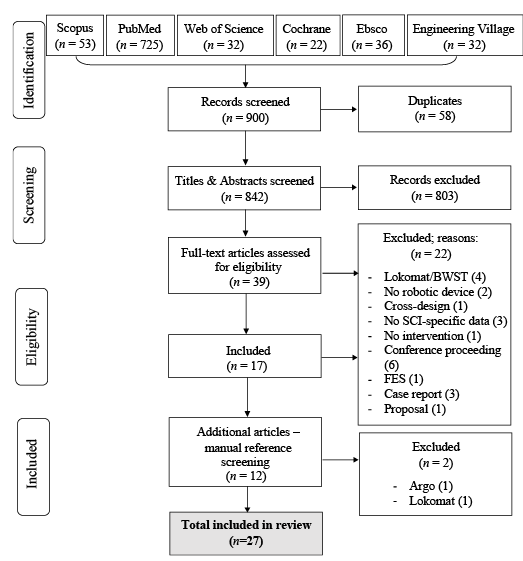
Two reviewers independently selected and assessed the studies for inclusion eligibility. With the assistance of a third reviewer, any disagreements were resolved by discussion and consensus. Titles and abstracts were initially screened to exclude all review articles, conference proceedings, commentaries, letters, book chapters, animal or in vitro studies. Studies with fewer than 3 participants were excluded to eliminate bias inherent with case reports. Full texts were excluded if mixed diagnoses were included, SCI-specific data were not reported, training was limited to a treadmill or the protocol utilized upper body exoskeletons, orthotic devices or hybrid (electrical stimulation) exoskeletons. Duplicate items were excluded preceding the screening process. Manual searches of reference lists from relevant articles were completed. Of the 900 articles initially identified, 39 met the selection criteria in both the title and abstract, and 22 of these were eliminated after reading the full text. Ultimately 17 studies were included from the online databases and an additional 10 from scanning the references of relevant articles (Fig. 1).
Fig. 1. Outline of the literature search procedure and article selection.
Data extraction
Two reviewers independently extracted the data from the included studies using a pre-established data abstraction table (Table I). Authors were contacted for further information if required. Participant and experimental details were summarized for each study, and outcome variables were tabulated provided they were reported by a minimum of 3 of the included studies. Non-tabulated results are shown in the Appendix SI1.
Outcome measures
Walking performance outcomes included: (i) the 6-min walk test (6MWT), measures the distance and velocity walked over a 6-min period, and serves as an indicator of submaximal
aerobic capacity; (ii) the 10-metre walk test (10MWT) measures the velocity achieved during a 10-m walk; (iii) Timed Up and Go (TUG) tests the time required to stand up, balance and sit down again. Cardiovascular demand outcomes included heart rate (HR), blood pressure (BP) and rating of perceived exertion (RPE). RPE values were self-reported according to the Borg 6–20 scale. Secondary complications, including spasticity and pain, were measured using subjective ratings: numeric rating scale of 0–10 for spasticity and 0–6 for pain, as well as visual analogue scales (VAS) using a 10-cm ruler and a marker that the participant moves to the point indicating the intensity of pain. Clinical tests included the Modified Ashworth Scale and the Spinal Cord Assessment for Spastic Reflexes. User-satisfaction utilized a variety of subjective rating questionnaires assessing the acceptability of the exoskeleton device and quality of life (QoL) scores.
Quality criteria
The quality of evidence of the extracted data was assessed according to the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) system. The quality of the studies was extracted independently by 2 reviewers using a standardized protocol and data collection table according to STROBE (Table SII1) guidelines adapted from the Equator system.
Data analysis
Meta-analyses were completed for the walking performance tests. Random effects models were reported based on the high variability noted between studies. The standardized mean differences and 95% confidence interval (95 % CI) were calculated. To ensure positive estimates for all meta-analyses, the study means were multiplied by –1 according to the statistical correction described in the Cochrane Handbook. Forest plots were used to illustrate the individual study findings and the pooled estimate results. Statistical significance level was set at p < 0.05. The I2 statistic was used to estimate heterogeneity of effects across studies, with values of < 25%, 50% and > 75% representing low, moderate and high inconsistency, respectively. Statistical analyses were performed using RevMan Review Manger 5.3. Participant and intervention characteristics were summarized using means and standard deviations (SD) for continuous data, and counts and percentages for categorical data.
Study characteristics
All studies included in this review were prospective non-randomized, uncontrolled trials, of which all, except 3, were single-centre studies conducted in the USA (12), Italy (3), Canada (3), Japan (2), Germany (1), Netherlands (1), UK (1) and Israel (1). A single study was conducted at multiple centres across the UK, Europe and Australia (11), and 2 others were conducted across 5 centres within the USA (12) and 9 centres within Europe (13). Sample sizes ranged from 3 to 44 participants.
Participant characteristics
Mean participant age was 40 years (SD 7) , with males accounting for 78% of the sample. The majority of participants presented with complete SCI between T1 and T12 (Fig. S11). Time since injury varied considerably between studies, with the majority of participants presenting with chronic injuries (> 1 year).
Training protocols
The ReWalk™ (ReWalk Robotics Inc., Marlborough, MA, USA) powered exoskeleton was evaluated in 11 studies, Ekso® (Ekso Bionics, Richmond, CA, USA) in 10 studies, Indego™ (Parker Hannifin Corp.,
Cleveland, OH, USA) in 3 studies, WPAL (Fujita Health University, Japan) in 2 and REX (Rex Bionics plc, London, UK) in one study. The mean intervention length was 12.1±19.6 weeks, with a wide range of 1–24 weeks, 8 weeks being the most common. Typically, training was conducted 3 times per week for 60 min per session (Table I).
Table I. Baseline participant characteristics and robotic locomotor training (RLT) design
Ambulatory outcomes
Walking performance. Meta-analyses were performed on the 7 studies that assessed walking performance tests, including the 6MWT (Fig. 2), the 10MWT (Fig. 3) and the TUG (Fig. 4). Five studies reported a positive pooled effect of –0.94 (95% CI –1.53, –0.36) with moderate heterogeneity (I2 = 27%, p = 0.002) for the distance achieved during the 6MWT. Six studies reported a positive pooled effect of –1.22 (95% CI –1.87, –0.57) with high heterogeneity (I2 = 60%, p = 0.0002) for the speed achieved during the 10MWT. Five studies reported a positive pooled effect of 0.74 (95% CI 0.36, 1.11) with no heterogeneity (I2 = 0%, p = 0.0001) for the time required to complete the TUG. Importantly, 4 of the 7 studies included in the meta-analyses involved chronic recovery phases (7, 14–16), one involved both acute and chronic phases (13) and one study did not report on this recovery period (12). Variations in other participant characteristics, including age, level of injury, and intervention protocols differences, could also act as cofounders to the results observed between studies. This variability between studies is evident in the moderate-high heterogeneity scores observed in Figs 2 and 3.
Walking velocity and distance. Six studies considered the mean distance and velocity achieved during a 6MWT showing a range from 47 to 129 m and 0.22 to 0.36 m/s, respectively (6, 17–20, 22) (Appendix I). Six studies considered the velocity required to complete a 10MWT (Appendix II), ranging from 0.25 to 0.38 m/s across 4 studies (17, 18, 20, 21). The remaining 2 studies indicated that different injury levels can affect walking velocity (22), as can the level of assistance provided while walking (23).
Fig. 2. Effect of robotic locomotor training on 6-min walk test (6MWT) distance (m) using a random effects model. Standardized mean difference –0.94 (95% confidence interval (95% CI) –1.53,–0.36; I2=27%; p = 0.002).
Fig. 3. Effect of robotic locomotor training on 10-metre walk test (10MWT) speed using a random effects model. Standardized mean difference –1.22 (95% confidence interval (95% CI) –1.87,–0.57; I2 = 60%; p = 0.0002).
Fig. 4. Effect of robotic locomotor training on the Timed Up and Go test (TUG) time (in s) using a random effects model. Standardized mean difference 0.74 (95% CI 0.36, 1.11; I2 = 0%, p = 0.0001).
Cardiovascular demand. Four studies considered HR measures across the intervention (Table II), where no significant changes were found (2, 13, 14, 20). Three other studies, in addition to studies by Bach Baunsgaard et al. (13) and Spungen et al. (20), considered HR changes within an exercise session. HR was reported to be highest during walking, compared with that of sitting or standing, and post-walking HR was higher than pre- or mid-walking HR (6, 7, 13, 24). Spungen et al. (20) determined HR to be highest during a 6MWT compared with other phases of the session. Four studies considered BP changes with exoskeleton walking (Table II). Two of the studies found a significant increase in BP from pre to post session (7, 24). However, Bach Baunsgaard et al. (13) found no change in BP within the session or across the intervention. Spungen et al. (20) also found no changes in BP across the walking intervention.
Six studies investigated changes in RPE (Table II). Two studies showed a significant decrease in walking RPE from baseline to post-intervention (13, 20). The other 2 studies showed no significant changes in RPE across walking sessions (15, 16). Two studies demonstrated that RPE within a session increased post- compared with pre-walk (6, 24).
Table II. Cardiovascular outcomes in individuals with spinal cord injury (SCI) using robotic locomotor training (RLT)
Spasticity and pain. Five studies considered spasticity measures (Table III), 2 studies used clinical measures only (7, 25), while the other 3 considered both clinical and subjective ratings (2, 18, 26). Of those presenting clinical measures, 2 found significant improvements in spasticity from pre to post walking (7, 26), one showed reduced spasticity across the intervention (18) and one indicated no change (25). All the studies using self-reported measures indicated improvements in spasticity ratings across the intervention (2, 18) and a significant reduction in RPE within a walking session (26). The majority of the pain findings indicated significant reductions in pain intensity both within a session (4, 7, 26) and across the intervention (2, 18). Three of the 8 studies reported no change in pain perception within a session (19) or across the intervention (15, 16) (Table IV).
Table III. Spasticity assessments in individuals with spinal cord injury (SCI) using robotic locomotor training (RLT)
Table IV. Pain assessments in individuals with spinal cord injury (SCI) using robotic locomotor training (RLT)
User-satisfaction. Nine studies considered the participant satisfaction with using a robotic exoskeleton for rehabilitation (Table V). Four studies used a VAS of agreement from 1 to 5 regarding 10 statements (15, 16, 18, 19). Three of these studies showed that more than 80% of those statements were rated as above mean agreement (> 3 score). Two studies indicated a disagreement (< 3 score) with the statements regarding bowel function, ease of use of the device, and safety in the device. Esquenazi et al. (18) stated that all participants (n = 12) reported that using the device caused no pain, and the majority (90%) found that it caused no fatigue. Some participants (27%) reported improved spasticity, and 45% reported improvements in bowel function. Two studies considered the use of a different VAS to rate the acceptability of the device from 1 to 7. One of these studies indicated a majority positive response (93.7%) for the statements, with only one negative response, related to transfer ability into the device (11). Stampacchia et al. (26) found that participants rated the positive sensations with high scores (mean VAS score 6) and the negative experiences with low scores (mean VAS score 2.5). Gagnon et al. (27) used a VAS of 0–100%, in which the mean percentages for each question indicated that participants were satisfied with the training (mean score 95.7%), felt motivated to continue training (91.3%), and that there was strong ability to use the device (79.6%). A mean score of 67.9% was given for the perceived health benefits and 16.7% for complications and risks of using the device (27).
Using the Assistive Technology Device Predisposition Assessment questionnaire, Benson et al. (7) showed that QoL improved by 4 points and the mean device form score decreased by 7 points across the intervention. This study also showed that the mean disability appraisal score decreased across the intervention by 3 points (7). Platz et al. (25), which used the SF-12v2 questionnaire, indicated that physical functioning improved across the intervention by 0.38 z-score, and that emotional well-being was rated higher than that of the normal population.
Table V. User-satisfaction of individuals with spinal cord injury (SCI) using robotic locomotor training (RLT)
Quality of evidence
As a consequence of important limitations in study design, inconsistency and lack of directness in the results, the overall quality of evidence was judged to be very low using the GRADE system (Table VI). Further research on RLT for SCI rehabilitation is highly likely to have an important impact on confidence in the estimate of effect.
Table VI. Quality of evidence using the GRADE system
This systematic review aimed to provide an overview of the current evidence on RLT rehabilitation after SCI, focusing on walking performance and secondary measures including cardiovascular demands and health-related benefits. A total of 27 non-randomized, non-comparative observational studies, representing 308 participants, were included in the analysis.
Gait parameters
The meta-analyses performed on the relevant included studies showed that RLT can be used as an effective rehabilitation method to significantly improve walking capacity (p < 0.001). Positive pooled effects were found for the 6MWT, 10MWT and TUG meta-analyses from pre to post RLT interventions (Figs 2–4). Other studies have shown similar positive effects of RLT on walking function in several neurological diagnoses, but the mechanism behind this restored function is still debated (15).
Walking function is correlated with an increase in session number (p < 0.001), as participants were able to walk greater distances with improved velocities over more training sessions (2, 7, 18, 20, 21). This general trend of improved walking capacity suggests a training effect due to the increased proficiency in ambulating within the exoskeleton device over time (4). Longer training periods ensure repetitive task practice, improving performance through increased motor learning and neuroplasticity (3, 8, 16, 17, 28). Walking capacity is also dependent on level, severity and time since injury (15, 22). Participants with lesions at a lower level walked longer distances and faster than those with lesions at a higher level (19, 22). Individuals with recent injuries were more likely to respond to training stimuli and achieve greater velocities than those with chronic injuries (8, 15). Therefore, implementation of more formalized SCI training programmes based on level and time since injury may result in improved outcomes for functional mobility after RLT interventions.
The mean velocity achieved across the studies for the 6MWT ranged from 0.22 to 0.36 m/s and the mean velocity in the 10MWT ranged from 0.25 to 0.38 m/s. A previous meta-analysis investigating a similar group of heterogeneous individuals, with various RLT protocols encompassing a wide range of training sessions, found a similar weighted mean gait velocity of 0.25 m/s (5). The review by Miller et al. (9) suggests that these gait velocities are encouraging for independent ambulation in home and community environments. However, currently, it is only the ReWalk exoskeleton that is designed for use in settings outside of rehabilitation facilities. Other authors report that these velocities are not considered sufficient for community ambulation. Forrest et al. (29) found a threshold of 0.44 m/s for limited community ambulation after incomplete SCI, Yang et al. (17) suggested that a gait velocity of 0.40 m/s enables an individual to participate in community living, while Andrews et al. (29) determined the mean velocity necessary to cross an intersection at traffic signals to be 0.49 m/s. Potentially, such differences in gait velocities exist between studies due to the variability in population, training methods and the outcome measures used for assessing walking performance. This inter-study variability is highlighted in the moderate-to-high heterogeneity scores of 27% and 60%, respectively, for the 6MWT and 10MWT meta-analyses performed in this review (Figs 2 and 3).
Cardiovascular demand
As a result of the unstable autonomic control after a SCI, these individuals have an increased risk of developing heart disease and stroke, with cardiovascular and respiratory dysfunctions being among the leading causes of death for people with SCI (30). This increased mortality risk means that early recognition and accurate management of cardiovascular dysfunctions are crucial to reducing their secondary risk profile (23, 36, 38).In this review, studies considering cardiovascular changes in HR and BP indicated no significant changes in HR with RLT interventions and reported variable BP changes within and post RLT. Two studies reported a significant increase in BP post-RLT (7, 24), while the other 2 studies showed no changes across the intervention (13, 20). It is important to note that the studies that reported on these cardiovascular outcomes were all highly variable in terms of the level and severity of injury across participants. The higher the level of the SCI, the greater the degree of sympathetic nervous system dysfunction and quadriplegia results in lower maximal HRs compared with high and low paraplegia (33). Thus, rehabilitation interventions should consider these factors when assessing changes in cardiovascular function between individuals with SCI.
HR was highest during walking compared with sitting or standing in the devices (6, 13, 20, 24), and RLT sessions resulted in light-to-moderate levels of exercise intensity (6, 7, 13, 14, 20, 24). Evans et al. (14) suggested that this moderate intensity exercise is in accordance with the American of College of Sport Medicine guidelines for health-promoting activity levels, according to the percentage of predicted peak oxygen uptake (%VO2peak) and metabolic equivalents (METs) expended. These results align with previous findings of exoskeleton walking, in which studies concerned with RPE reported exercise sessions to be consistent with light-to-moderate exercise intensity (6, 13, 24). These data suggest that RLT allows patients with SCI to engage in physical activity at an intensity that provides health benefits, yet does not result in early fatigue. RPE values also showed that participants were able to tolerate longer sessions and walk greater distances during each session with lower reported RPEs over time (20).
Secondary complications
Weight-bearing activity and over-ground ambulation have been shown to reduce many of the secondary complications associated with SCI, by increasing body strength and aerobic capacity, minimizing declines in bone mineral density, improving circulation and countering the other health risks associated with prolonged sitting (9, 15). Exercise thus acts as a health-promoting activity following SCI (34).
Benson et al. (7) reported that the participants who reported mild spasticity pre-session, experienced a slight improvement post-session. The reduction in spasticity was observed in previous case reports evaluating the training effects of using powered exoskeletons (18, 35). Miller et al. (9) also reported that clinically relevant improvements were found in self-reports for muscle spasticity in various other RLT studies. The decrease in spasticity following RLT might be explained by the activation of neuronal circuits involved in walking, which is able to reduce the under-regulated hyperactivation present in spasticity (26). Another cause of the decreased spasticity may be the effect of the mobilization of usually unused muscles, which leads to muscular fatigue and muscular reductions in co-contraction and excitibility (18, 26). Pain reports were decreased during and after use of the robotic exoskeletons, with one study indicating as much as a 9% decrease in pain post-RLT (15, 24). The decreased pain reports could be attributed to the improved psychological benefit of walking again (26), endogen endorphins activated by the walking exercise (26) and reduced muscular spasticity (7, 26).
User-satisfaction
In addition to the physiological and functional benefits of RLT, there are many psychological and social benefits to standing, including improved self-image, eye-to-eye interpersonal contact and increased independence (2, 15, 20, 35). The majority of studies found that the users felt safe and comfortable in the device and had tendencies towards strong positive comments regarding the acceptability and emotional/health benefits of the training process (11, 15, 16, 18, 19, 25–27). Improvements in QoL and psycho-emotional wellness were also reported post-intervention (7, 25). Despite these positive perceptions, Benson et al. (7) showed that the mean device form score of 41 points indicated that participants initially had positive expectations of using the exoskeleton, but not all these expectations were met, as the mean study end-point score was 34. This reduced satisfaction may be due to the few reports that wearing or adjusting the device was not relatively simple, and that there were no real improvements in their bowel programmes. Unrealistic initial expectations and hopes of taking part in the RLT programme may also play an important role in user-satisfaction.
Study limitations
This review highlights the underpowered evidence base regarding the efficacy of RLT, primarily due to the heterogeneity in the study characteristics and small sample sizes. Significant bias further diminishes the power of the findings and generalizability to clinical practice. Six studies did not disclose their conflicts of interest. The remaining 21 studies did discuss potential biases, with 5 studies acknowledging competing interests, whereas the other 16 had none to declare. However, 9 of these 16 studies declared incorrectly, as they did not acknowledge the conflicts of interest related to being financially supported (11, 13) and receiving salaries from exoskeleton companies (14, 19, 21, 22, 36) or performing the study to achieve FDA clearance for the exoskeleton company (12, 24). It is relevant to note that due to the high cost of the robotic devices, subsidization is often required from the relevant companies for access and/or maintenance of the devices. This support is crucial to research being undertaken by independent researchers, but the potential for reporting/publication bias is therefore increased, as companies try to gather evidence to support their devices.
This review indicates the need for well-designed, randomized clinical trials (RCTs), with homogenous samples and relevant control groups who received more conventional gait training. Future studies should be consistent in their training protocols and ensure adequate intervention length to allow for more meaningful comparisons. In addition, the inconsistency of outcome reporting among studies exposes the necessity of developing standardized protocols and sensitive outcome measures to evaluate RLT interventions in people with SCI.
Conclusion
Clinical application of these assistive devices appears promising as a tool to offer more comprehensive care for patients with SCI. This review indicates that RLT can provide individuals with SCIs the ability to walk safely while improving their walking performance as well as improved health outcomes and psychological well-being. Further large clinical trials with sufficient rehabilitation durations, as well as adequately powered homogenous studies, are required to better understand these effects of RLT on individuals with SCI.
This Study was supported by the National Research Foundation of South Africa, University of Cape Town and Oppenheimer Memorial Trust.
The authors have no conflicts of interest to declare.
Appendix I. Mean 6-min walk test (6MWT) outcomes in individuals with spinal cord injury (SCI) using robotic locomotor training (RLT)
Appendix II. Mean 10-metre walk test (10MWT) velocity in individuals with spinal cord injury (SCI) using robotic locomotor training (RLT).


 Click to show fullsize
Click to show fullsize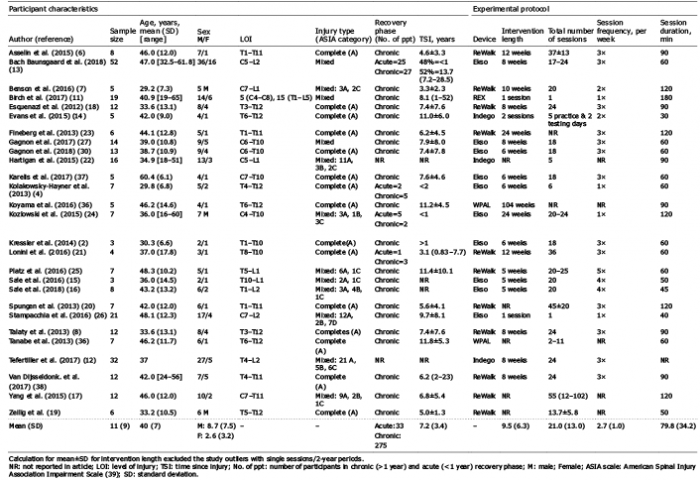 Click to show fullsize
Click to show fullsize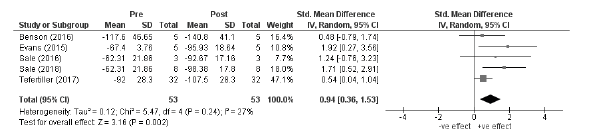 Click to show fullsize
Click to show fullsize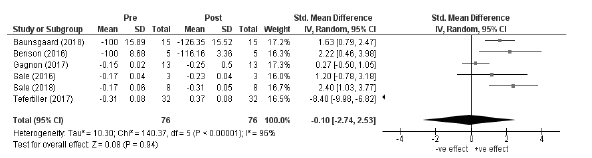 Click to show fullsize
Click to show fullsize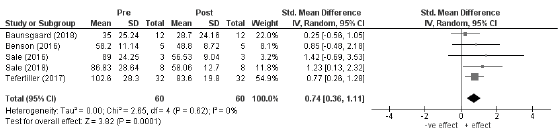 Click to show fullsize
Click to show fullsize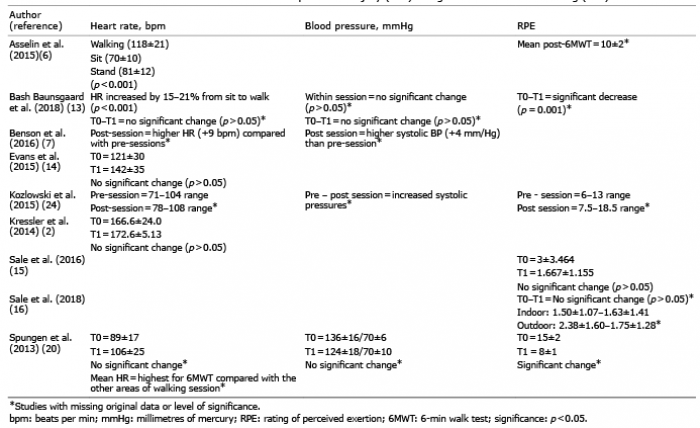 Click to show fullsize
Click to show fullsize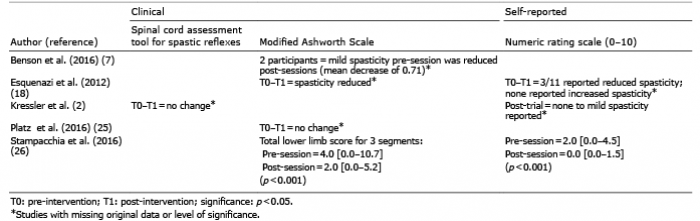 Click to show fullsize
Click to show fullsize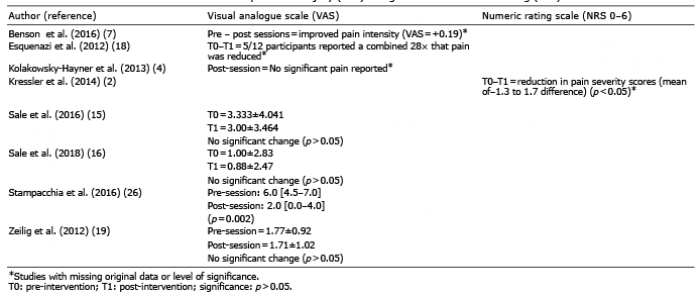 Click to show fullsize
Click to show fullsize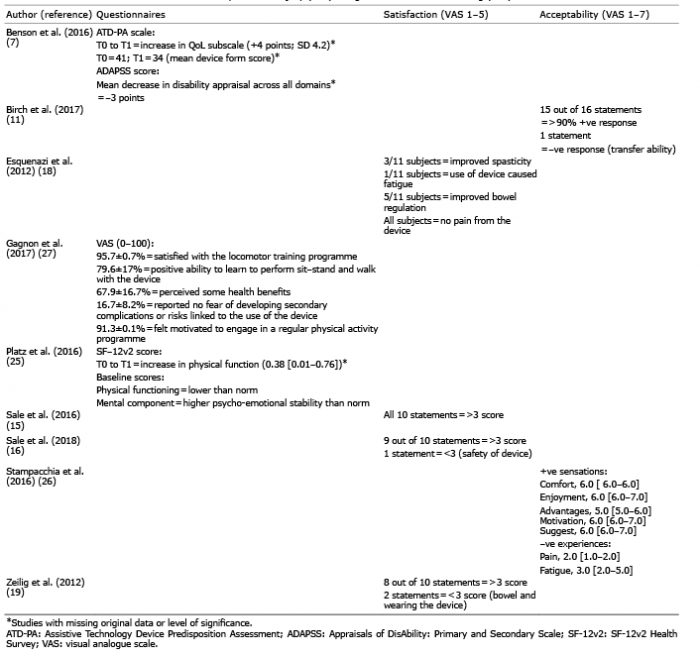 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize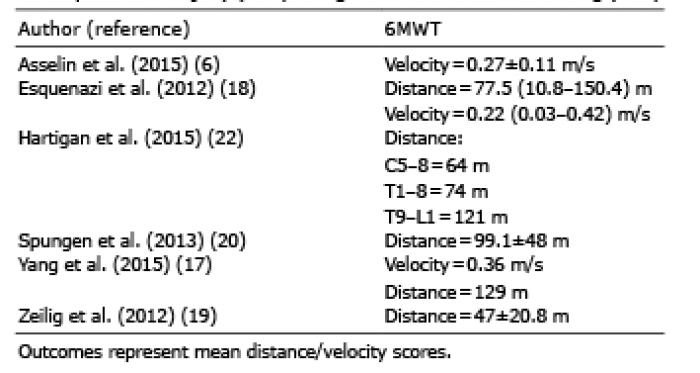 Click to show fullsize
Click to show fullsize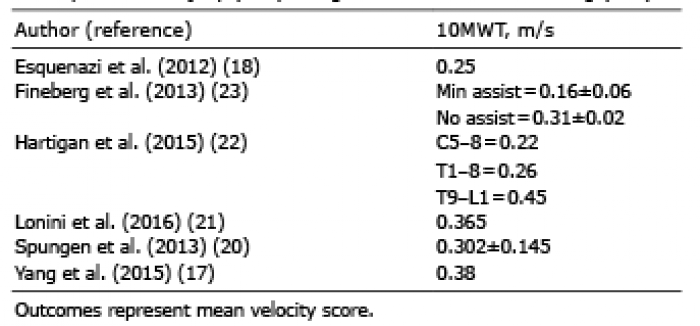 Click to show fullsize
Click to show fullsize