
From the 1Pain and Rehabilitation Centre, and Department of Medical and Health Sciences, Linköping University, Linköping, 2Department of Clinical Neuroscience, Karolinska Institutet, 3Department of Neuroradiology and Department of Perioperative Medicine and Intensive Care, Karolinska University Hospital, Stockholm, 4Department of Neuroscience and Physiology, Section of Health and Rehabilitation, Physiotherapy, Sahlgrenska Academy, University of Gothenburg, 5University of Gothenburg Centre for Person Centred Care (GPCC), Sahlgrenska Academy, Göteborg and 6Department of Dental Medicine, Karolinska Institutet, and Scandinavian Centre for Orofacial Neurosciences (SCON), Huddinge, Sweden
*These authors are joint first authors. **These authors are joint last authors.
Background: The pathophysiology of fibromyalgia includes central and peripheral factors. Neurotro-phins, such as nerve growth factor and brain-derived neurotrophic factor, are involved in peripheral and central nervous system development of pain and hyperalgesia. Few studies have examined circulating nerve growth factor and brain-derived neurotrophic factor in fibromyalgia or have investigated whether exercise interventions affect the levels of these peptides.
Objectives: To compare plasma levels of nerve growth factor and brain-derived neurotrophic factor in fibromyalgia and in healthy controls, to investigate correlations between levels of nerve growth factor, brain-derived neurotrophic factor, and cytokines and clinical variables, and to investigate the effect of exercise on these levels.
Subjects and methods: A total of 75 women with fibromyalgia participated in blood tests at baseline and after the 15-week intervention, and 25 healthy controls participated at baseline. Patients were randomized to a 15-week progressive resistance exercise intervention or a relaxation intervention.
Results: Brain-derived neurotrophic factor level was significantly higher (p < 0.001) and nerve growth factor level was significantly lower (p < 0.001) in fibromyalgia than in healthy controls. Neither resistance exercise nor relaxation interventions affected the levels of brain-derived neurotrophic factor or nerve growth factor. No significant correlations were found between brain-derived neurotrophic factor or nerve growth factor plasma levels in fibromyalgia and cytokine levels or clinical variables.
Conclusion: Changes in circulating nerve growth factor and brain-derived neurotrophic factor levels may affect nociception/pain in fibromyalgia. Clinical improvements were achieved following the exercise intervention, but the levels of brain-derived neurotrophic factor and nerve growth factor were not normalized.
Key words: brain-derived neurotrophic factor; biomarker; chronic pain; fibromyalgia; nerve growth factor; plasma.
Accepted Aug 16, 2019; Epub ahead of print Aug 30, 2019
J Rehabil Med 2019; 51: 00–00
Correspondence address: Emmanuel Bäckryd, Pain and Rehabilitation Centre and Department of Medical and Health Sciences, Linköping University, SE 581 85 Linköping, Sweden. E-mail: emmanuel.backryd@regionostergotland.se
Patients with fibromyalgia have treatment-resistant chronic pain. More research is needed in order to understand how and why fibromyalgia develops. Neurotrophins, such as nerve growth factor and brain-derived neurotrophic factor, are involved in peripheral and central nervous system development of pain and hyperalgesia, but few studies have examined circulating nerve growth factor and brain-derived neurotrophic factor in fibromyalgia or have investigated whether exercise interventions affect the levels of these peptides. This study compared blood levels of nerve growth factor and brain-derived neurotrophic factor in fibromyalgia with those in healthy controls, and investigated the effect of exercise on these levels. Brain-derived neurotrophic factor levels were higher and levels of nerve growth factor were lower in fibromyalgia, compared with healthy controls. Clinical improvements were achieved following the exercise intervention, but the levels of brain-derived neurotrophic factor and nerve growth factor were not normalized.
Fibromyalgia (FM) is a characterized by chronic widespread pain and generalized hyperalgesia. FM in the western world has high comorbidity with other chronic pain conditions and somatic and psychological symptoms/disorders. The prevalence of FM is 2–8%, depending on the diagnostic criteria used. No definite pathophysiology has been established. Anatomical and functional changes in the brain, neuroinflammation including activation of glia cells, opioidergic dysregulation, nociception-driven amplification of neural signalling (central sensitization), and impaired top-down modulation have been reported, as well as systemic low-grade inflammation and nociceptor and muscle alterations (1–6). Taken together, these alterations may indicate complicated interactions between peripheral nociception and central processes.
Nerve growth factor (NGF) and brain-derived neurotrophic factor (BDNF) are proteins involved in sensitization processes reasonably associated with hyperalgesia (1, 7), an important characteristic of FM. They are neurotrophins (NTs), which regulate the growth and apoptosis of neurones in the developing nervous system and repairing injured neurones. NGF and BDNF are mostly synthesized in the dorsal root ganglia of the spinal cord (7).There are 4 NTs in humans: NGF, BDNF, neurotrophin 3 (NT-3), and neurotrophin 4 (NT-4). NTs bind with high affinity to their specific tyrosine receptor kinase (Trk); NGF binds to TrkA, BDNF and NT4 to TrkB, and NT3 to TrkC. All NTs can also bind with lower affinity to the neurotrophin receptor p75 (7).
NGF is a key molecule for the sensitization of primary nociceptors associated with tissue inflammation and it is increased in inflamed tissue (8). Preclinical data have revealed that neutralization of endogenous NGF prevents inflammatory hyperalgesia (8). The NGF-TrkA complexes are retrogradely transported by sensory fibres to the cell bodies, resulting in several genomic actions that increase the sensitivity of pain fibres. In addition to increased ion channel functions, NGF causes the release of substance P and CGRP at both peripheral and central levels and may contribute to sensitization (8). In addition, increased muscle and systemic and cerebrospinal fluid (CSF) levels of substance P have been found in FM (9–11). Higher concentrations of both NGF and BDNF have been reported in CSF of patients with FM (12, 13). However, to the best of our knowledge, no studies have reported circulating levels of NGF in FM.
BDNF regulates neuronal growth, recovery, development, and central and peripheral plasticity, as well as pre- and post-synaptic mechanisms (14, 15). A possible negative role of BDNF is the development and maintenance of central sensitization in chronic pain conditions (16). There are only a few studies of circulating BDNF in FM and they are not in agreement. Higher plasma levels of BDNF in FM have been reported (17), but another study found no difference (18). Serum studies are also conflicting (19, 20). Despite a possible role in sensitization mechanisms, only one study has investigated the relationship between circulating BDNF levels and pain sensitivity in FM; a high BDNF level was associated with low pressure pain thresholds (PPT) (21).
Several symptoms of FM, such as hyperalgesia, anxiety, pain, and cognitive dysfunction, can be induced by cytokines (22, 23). Binding of NGF to TrkA and p75 can activate transcription factors, such as nuclear factor NF-κB and production of tumour necrosis factor alpha (TNF-α), and interleukins IL-1β, IL-2, IL-6, IL-8, and IL-12 (24). Elevated levels of IL-8 in blood and in CSF have been reported in FM (25–27), but less consistent alterations have been reported in other cytokines, such as IL-6, IL-1β, and IL-2 (28, 29). More complex alterations in plasma patterns of inflammatory substances have been reported recently in FM/widespread pain (27, 30).
Exercise is an often-used intervention in FM (31). However, the effects of exercise on NGF and BDNF and their relationships to improvements in clinical outcomes are sparsely investigated. Increased levels of BDNF were found after an exercise intervention in patients with osteoarthritis (32). In FM, changes in fatigue after an exercise intervention correlated negatively with changes in NGF (33). No alterations in plasma levels of BDNF were found after whole-body vibration in FM (18).
To summarize, it is unclear whether BDNF and NGF levels in blood are altered in FM, whether these levels are associated with important clinical characteristics, whether physical exercise affects BDNF or NGF levels, and, if so, whether these changes are related to clinical outcomes. These knowledge gaps motivated this study, which compares patients with FM and healthy controls with regard to plasma levels of NGF and BDNF, and investigates the effect of a 15-week programme of progressive resistance exercise therapy on these NTs. Within these aims, this study investigated correlations between these NTs, cytokine levels, chemokine levels, clinical presentations, and outcomes.
Study design
This is a sub-study of a randomized controlled multi-centre study (34).
Recruitment process
Recruitment and intervention of the multi-centre study started in 2010 and ended in 2013. It was executed in 3 cities: Linköping, Stockholm and Gothenburg. A more detailed description can be found in previous publications (34).
Inclusion criteria for women with FM were being of working age (20–65 years) and a diagnosis according to American College of Rheumatology criteria from 1990. Exclusion criteria were high blood pressure (>160/90 mmHg), osteoarthritis in knee or hip, severe somatic or psychiatric disorders, causes of pain other than FM, high use of alcohol, and inability to understand or speak Swedish. Subjects were not allowed to participate in a rehabilitation programme within the past year or practice resistance exercise or relaxation therapy twice a week or more. Consuming analgesics, non-steroidal anti-inflammatory drugs (NSAID), or hypnotic drugs were not allowed for 48 h before examination (34).
Subjects with FM were recruited through local newspaper advertisements. As a result, 402 women with FM expressed interest in participating in the study. After telephone screening, 177 women took part in a medical examination, of whom 130 fulfilled the inclusion criteria and were included in the study. Age, weight, height, and blood pressure were registered, and body mass index (BMI) was recorded. Subjects answered a range of questionnaires about their pain and general and psychological health. Functional tests and tender-point thresholds testing were performed. A 20-ml blood sample was collected. Finally, the women with FM were randomized into 2 groups: those who received resistance exercise and those who received relaxation therapy (34). A 20-ml blood sample was also collected after the intervention.
The control group (healthy controls; HC) included 130 healthy, age-matched, and pain-free women. The control group underwent the same procedures and similar data were collected for baseline comparison (34).
Subjects
As described above, there were originally 260 participants in the multi-centre study: 130 women with FM and 130 HC. Plasma levels of cytokines and chemokines for the total cohort were previously analysed (28). Plasma samples from 100 participants were available for analysis of NGF and BDNF and consequently only those subjects were included in this study; 75 out of the 100 were women with FM and 25 were HC.
After receiving verbal and written information about the study, all subjects signed a consent form, which was in accordance with the Declaration of Helsinki. The study was approved by the Regional Ethics Committee in Stockholm (Dnr: 2010/1121-31/3) and was registered on 21 October 2010 (Clinicaltrials.gov NCT01226784).
Variables registered
Age, BMI, and systolic and diastolic blood pressures were registered at baseline, as well as FM duration and number of tender points. Psychometric variables and PPT were registered at baseline (both FM and HC) and after the interventions (only in FM). Data have previously been presented for the total cohort (FM: n = 130 and HC: n = 125) (28, 31). Details about the variables are presented in those studies (28, 31). Global pain intensity was measured using a 0–100-mm visual analogue scale (VAS), where 0=no pain and 100=worst pain imaginable. The Hospital Anxiety and Depression Scale (HADS) and Pain Catastrophizing Scale (PCS) were used to detect psychological distress of study participants. Two summary components from the Short-Form Health Survey (SF36), physical (SF36-PSC) and mental (SF36-MSC), were used to define quality of life; a high score indicates better health. The Fibromyalgia Impact Questionnaire (FIQ) was used to portray the grade of symptoms and disabilities. The Multidimensional Fatigue Inventory (MFI) was used to evaluate different dimensions of fatigue. A higher score on FIQ and MFI indicates lower health (28, 31). PPTs were measured with an electronic pressure algometer (Somedic, Hörby, Sweden) over 4 bilateral points, as recently described in detail (28, 31).
Resistance exercise therapy and relaxation therapy
The women with FM were randomized to 2 intervention groups: resistance exercise or relaxation therapy (as reported earlier) (31). In this sub-study, 41 out of 75 subjects (54.7%) were randomized to the resistance exercise group and 34 subjects were randomized to the relaxation therapy group. All the healthy controls underwent the resistance exercise intervention, but data from them were not collected afterwards.
Both interventions lasted 15 weeks and have been described in detail elsewhere (31). The programme of progressive resistance exercise included training twice per week and was supervised by physical therapists. All sessions started with a 10-min warm-up and continued with 50 min of strength training focussing on the lower body. The training programme started with 40% of the maximum voluntary capacity (MVC) and continuously developed up to 70–80% of MVC during the 15-week period (31).
The relaxation therapy was selected as an active control intervention. It was provided twice a week as a 25-min session under the supervision of physiotherapists. The intervention contained mental exercises, e.g. relaxation and autosuggestion. The patients were guided through all the body parts, where each part was in focus one at a time. All sessions ended with stretching (31).
Blood samples
At baseline and after the 15-week intervention, 20 ml of blood were collected from all study participants. The blood was taken from the decubital vein. Samples were directly placed on ice and transported to the local laboratories. Blood was centrifuged and plasma was separated, aliquoted, and stored at –86°C until analysis (28).
Biochemical analysis
Plasma samples were analysed for NGF and BDNF using the customized multiplex electrochemiluminescence assay panel from Meso Scale Discovery (MSD, Rockville, MD, USA) according to the manufacturer’s protocol. The limits of detection (LOD) were 0.33 pg/ml for NFG and 5.09 pg/ml for BDNF.
Levels of cytokines and chemokines (IFN-ɣ, IL-1β, IL-2, IL-4, IL-6, IL-8, IL-10, IL-17A, TNF-α, IL-1ra, eotaxin, IP-10, and MCP-1) have been reported for the total cohort (i.e. FM: n = 125 and HC: n = 130) (28). From these analyses, we have used results from 75 women with FM and 25 healthy controls, which were included in this study. Analyses were performed using Luminex technology (Bio-Plex, Bio-Rad Laboratories Inc., Hercules, CA, USA) standard kits.
Statistical analysis
Statistical analyses were performed using IBM SPSS Statistics (version 24.0: IBM Corporation, Somers, NY, USA) for traditional statistical analyses, and SIMCA v.14.0 (UMETRICS, Umeå, Sweden) was used for advanced multivariate analysis (MVDA). Mann–Whitney U test was used for comparisons between FM and HC. The Wilcoxon signed-rank test was used for comparisons within groups (i.e. before vs after the intervention). Significance of the statistical tests was set at p < 0.05. Unless stated otherwise, data are expressed as mean (standard deviation; SD). Survey data regarding FM duration, tender points, VAS global pain, PPT, and PCS were missing from 3 subjects in the FM group. Survey data regarding PPT, SF36, and MFI were missing from one healthy control. These subjects were excluded from the calculation regarding these variables.
To investigate the multivariate correlations between the neuropeptides, cytokines/chemokines, clinical outcomes, and group belonging orthogonal partial least squares discriminant analysis (OPLS-DA) were applied. First, data were overviewed by principal components analysis (PCA), which is an unsupervised statistical tool for data analysis and dimensionality reduction, which helps evaluating the quality and homogeneity of the dataset and identifies strong outliers using Hotelling’s T2, a multivariate equivalent of the 95% confidence interval (95% CI). Secondly, OPLS-DA was used to confirm group comparison of the NGF, BDNF, and cytokine levels, and to investigate the multivariate inter-correlations of NGF and BDNF with cytokines and clinical variables. The statistical significance of the regression was controlled using the p-value of the cross-validated analysis of variance (CV-ANOVA), which is diagnostic tool for assessing model reliability. The p(corr) value was used to investigate the importance of each variable in our MVDA models. |p(corr)| ≥ 0.5 was considered significant. Quality of the MVDA was controlled using R2 and Q2. The R2 value shows how well the model explains the dataset. Cross-validated Q2 is a measure of the predictive power of the model; in other words, it measures how well the model can predict a new dataset. In a high-quality model, Q2 and R2 values are close to each other.
Baseline characteristics
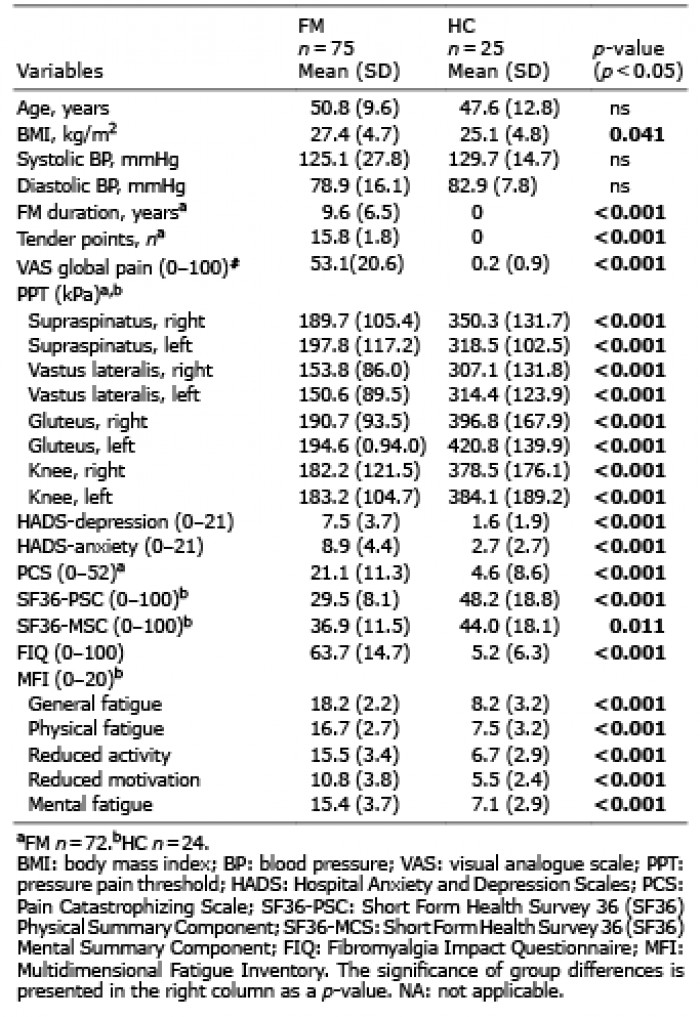
Table I shows the background data of both groups. BMI was significantly higher in patients with FM. There were no significant differences in age and blood pressures between FM and HC. FM and HC differed in the psychometric variables: patients with FM reported significantly worse health in all psychometric variables.
Table I. Background data of women with fibromyalgia (FM) and healthy female controls (HC)
Baseline levels of nerve growth factor and brain-derived neurotrophic factor
At baseline, there were significant differences in plasma levels of NFG and BDNF between FM and HC (Table II); FM had lower levels of circulating NGF than HC (p < 0.001), whereas the levels of circulating BDNF were higher in FM than in HC (p = 0.001).
Table II. Nerve growth factor (NGF), brain-derived neurotrophic factor (BDNF), cytokine, and chemokine levels at baseline from women with fibromyalgia (FM) and healthy female controls (HC)
Group differences at baseline in a multivariate context
To evaluate the importance of the bivariate statistical comparisons, including their relative importance, we performed an OPLS-DA of group membership (FM or HC) using NGF, BDNF, and the 13 cytokines and chemokines as regressors (i.e. x-variables reported in Table II). BDNF (p(corr) = –0.81) and NGF (p(corr) = 0.51) turned out to be the most important variables of this model representing the difference between FM and HC (R2 = 0.38, Q2 = 0.24, CV-ANOVA: p < 0.001). All the cytokines had |p(corr)|< 0.5 and were thus not of significant importance in the multivariate context for differentiating between FM and HC.
Regression of nerve growth factor and brain-derived neurotrophic factor with cytokines/chemokines at baseline
Using OPLS, it was not possible to significantly regress BDNF or NGF (i.e. Y variables) using cytokine and chemokine data as X variables, in all participants together (n = 100) or in each group separately (FM and HC, respectively). Hence, no significant multivariate associations existed between the 2 neurotrophins and cytokines/chemokines.
Regression of nerve growth factor and brain-derived neurotrophic factor with clinical variables at baseline
Using OPLS, it was not possible to regress BDNF or NGF using the clinical data shown in Table I as X variables, either in all participants together (n = 100) or in each group separately (FM and HC, respectively). Hence, no significant multivariate associations existed between the 2 neurotrophins and clinical data.
Changes in nerve growth factor and brain-derived neurotrophic factor levels after interventions in fibromyalgia
There was no significant difference in NGF or BDNF at baseline between the exercise and relaxation groups. No significant changes were found in NGF and BDNF levels in FM over time, i.e. before vs after interventions, either in the exercise or in the relaxation group (Table III).
Table III. Changes in nerve growth factor (NGF) and brain-derived neurotrophic factor (BDNF), levels after the interventions in women with fibromyalgia (FM)
Changes in clinical and functional measures after interventions in fibromyalgia
Marked differences in outcomes in favour of the exercise group were found for ratings of global pain, as well as for the physical subscale and the reduced activity subscale of MFI (i.e. absolute effects sizes > 0.70) (Table IV). No significant multivariate relationships were found between the changes in NGF and BDNF and the changes in the clinical variables shown in Table IV.
Table IV. Changes in clinical and functional measures after programme of progressive resistance exercise or relaxation therapy. Note: these results have been published elsewhere (31)
This study produced 4 major findings:
To the best of our knowledge, this is the first study to report circulating levels of NGF in FM; it found significantly decreased levels. Based on previous sparse studies of human conditions associated with chronic pain, one might expect higher levels of NGF in FM. Patients with chronic migraine had higher levels of plasma and saliva NGF than controls (35). In interstitial cystitis/bladder pain, significantly increased serum levels of NGF were found (36, 37). Increased NGF levels in the synovial fluid in patients with rheumatoid arthritis and in herniated discs of patients receiving surgery have been reported (24, 38). In contrast to these studies, the current study found the opposite; i.e. significantly lower levels of plasma NGF in FM. This study does not exclude that NGF levels may have been increased in the subacute and early chronic stage of FM. The fact that both IL-1β and NGF were significantly lower in FM may be due to the fact that NGF induces IL-1β release via TrkA (24), although we did not find any multivariate correlations between NGF and cytokines/chemokines.
A possible explanation for the lower levels of NGF might be related to the emotional situation of the patients with FM. Reduced levels of serum NGF were found in patients with major depression disorder (39) as well as in depressed elderly patients (40). However, against such an interpretation no significant associations with depressive symptoms were found in the present study. A highly conservative interpretation of our results could be that the lower levels of NGF are just random results and no peripheral alterations exist in FM. However, the study found increased levels of BDNF, and other studies of FM and of chronic widespread pain (mainly FM) have found altered levels of metabolites, cytokines, and anti-inflammatory lipids, and proteomic studies have reported prominent alterations both in muscle tissue and circulating proteins (28, 30, 41–43).
Our results of significantly lower levels of NGF may be consistent with other findings in the literature regarding patients with FM. NGF is a key molecule involved in the sensitization of primary afferent nociceptors associated with tissue inflammation and is increased in inflamed tissue (8). NGF may also be involved in sprouting of nociceptive fibres in peripheral tissues and promote pain (44). Several studies report a reduction in distal intraepidermal nerve fibre density (IENNFD) in the skin of prominent subgroups of FM, as well as a more prominent reduction in IENNFD with ageing in FM (3). Moreover, reduced nerve regeneration and growth factors were found in skin nerves of patients with FM (3). In addition, C-fibres with smaller diameters have been found in FM (3). These reports of small nerve fibre impairment may speculatively be due to lower levels of NGF in FM affecting development and regeneration of NGF-dependent neurones (45).
According to preclinical data, neutralization of endogenous NGF prevents inflammatory hyperalgesia (8), and the potential of anti-NGF antibodies have recently been the focus of intensive research, including several clinical trials in different chronic pain conditions. A review of low back pain with radiculopathy found positive evidence for small effects of anti-NGF treatment on pain relief and functional improvements (46). Our results with low NGF levels do not indicate a role of anti-NGF treatment in FM. The present results, with significantly lower levels of circulating NGF in FM, need to be confirmed before a definite conclusion can be drawn about the role of anti-NGF treatment in FM.
There are few studies of circulating BDNF in patients with FM and they are not in agreement. This, and a previous study, found higher plasma levels of BDNF in FM, but another study found no difference (17, 18). In addition, the results concerning serum levels of BDNF in FM are conflicting (19, 47). Conflicting results also exist for other pain conditions. Plasma levels of BDNF were higher in rheumatoid arthritis (RA) and in patients with osteoarthritis than in controls (48, 49). In contrast, a large study found no differences in serum levels of BDNF between patients with chronic pain (n = 764) and controls (n = 882) (50).
The significantly increased levels of BDNF cannot be explained by psychological factors according to the existing literature. As recently summarized, BDNF in serum was significantly decreased in depressed patients, whereas the results from plasma studies were inconclusive (51). In fact, several studies, including this study, have not been able to establish significant correlations between blood levels of BDNF and depressive symptomatology (17, 20, 47). Serum BDNF levels were significantly lower in subjects with insomnia compared with non-sleep disturbed control, and the BDNF levels correlated with severity of insomnia (52, 53). Insomnia is common in patients with severe chronic pain conditions. It was not registered in the present study; however, assuming that fatigue is a proxy for that, we found no relationship in a multivariate context between fatigue aspects and BDNF levels. Reasonably, and in agreement with the present multivariate analysis, the increased BDNF plasma levels in the present group of patients with FM cannot be explained by the presence of depressive symptoms or insomnia. Hence, this finding supports the interpretation that the increased levels of BDNF in FM are related to nociception and/or pain.
Taken together, these results for NGF and BDNF indicate alterations in the pattern of the 2 NTs, which are involved in important processes, such as growth, repair, and sensitization. However, with respect to the latter, no correlations were found between BDNF and NGF levels and PPT, which partially contradicts the results of an earlier study reporting that a high level of BDNF was associated with low PPT (21). It cannot be excluded that ceiling effects may be present for pain sensitivity (i.e. PPT) in patients with FM.
The current study found no associations between BDNF levels and other clinical characteristics in FM. This agrees with other FM studies, which have not been able to establish significant correlations between BDNF blood levels and age (17), gender (47), disease duration (17, 47), pain intensity (17), number of tender points (17), and disease severity according to FIQ (20).
As reported elsewhere, for the larger cohort of patients with FM we found positive clinical changes in the resistance exercise group (Table IV) (31). Previous studies of the same cohort have shown no, or only significant, effects in a few cytokines (IL-1ra and IL-1β) in plasma or in microdialysis samples from vastus lateralis after exercise, whereas levels of metabolites (glutamate and pyruvate) in muscle were normalized after the 15 weeks of exercise intervention (28, 54, 55). These findings, together with the present finding concerning NGF and BDNF, may suggest that the exercise programme affects the metabolic profile in muscle, but does not affect the immune profile in plasma in FM. Hence, the FM group shows a chronic inflammatory profile that is not normalized after 15 weeks of resistance exercise. Future studies analysing other specific proteins involved in muscle strength are warranted.
Strengths and limitations
One of the greatest strengths of this study is its design. Multi-centre study design provides relatively large study population, which would otherwise be difficult to achieve. The limitation of this study is the lack of recovery time after the interventions, which is possibly needed to normalize the plasma levels of NGF and BDNF. Post-interventional blood samples were taken one week after therapy programmes ended and there were no follow-up re-examinations. Some previous neuropeptide studies have reached a post-therapy reduction in neuropeptides when the follow-up time was several months (56).
Conclusion
This study found alterations in 2 molecules involved in sensitization and plasticity and recovery of the nervous system. This study, the first to investigate circulating NGF in FM, found significantly lowered levels of circulating NGF. These results do not indicate a role of anti-NGF treatment in FM. Plasma levels of NGF were significantly lower in patients with FM, whereas levels of BDNF were significantly higher in patients with FM. Progressive resistance exercise therapy or relaxation therapy for FM had no effect on the levels of these substances. No correlations existed between the 2 NTs and clinical characteristics, including pain sensitivity and intervention outcomes. The present study indicates that peripheral factors (i.e. alterations in NGF and BDNF) may be important for nociception and pain in patients with FM.
The study was supported by the Swedish Rheumatism Association, the Health and Medical Care Executive Board of Västra Götaland Region, ALF-LUA at Sahlgrenska University Hospital, Stockholm County Council (ALF), and ALF grants at Region Östergötland. Linköping University Hospital Research Fund. Swedish Research Council (K2013-52X-22199-01-3, K2015-99x-21874-05-4, 521-2010–2893), Karolinska Institute Foundation and AFA Insurance (140341) and NEURO Sweden. The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize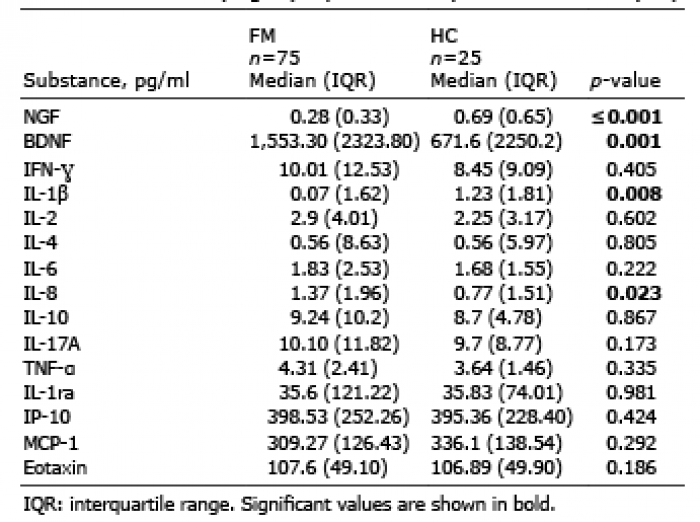 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize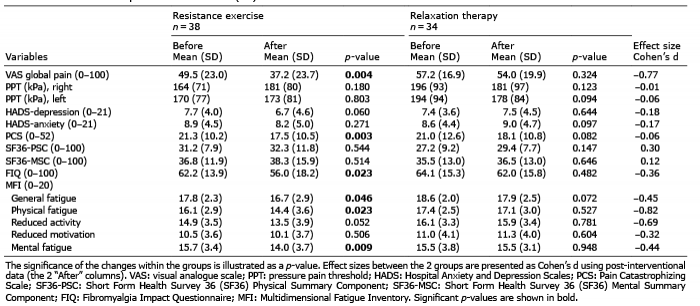 Click to show fullsize
Click to show fullsize