
From the 1Department of Medicine, Vestre Viken Hospital Trust, Bærum Hospital, Bærum, 2Department of Medicine, Oslo University Hospital, Ullevål, Oslo, 3Department of Physiotherapy, Oslo Metropolitan University, Oslo, 4Sunnaas Rehabilitation Hospital, HF, Nesoddtangen, 5Regional Centre for Child and Youth Mental Health and Child Welfare, Department of Mental Health, NTNU, Norwegian University of Science and Technology, 6Department of Neuromedicine and Movement Science, Faculty of Medicine and Health Sciences, NTNU, Norwegian University of Science and Technology, and 7Department of Medicine, Stroke Unit, Trondheim University Hospital, Trondheim, Norway
Objective: To examine the effects of individualized regular coaching and exercise on post-stroke cognitive and emotional function.
Methods: The Life After STroke (LAST) study investigated the differences between intervention and care-as-usual between 3 and 21 months post-stroke. Outcome measures were the Trail Making Test (TMT) A and B, Mini Mental State Examination (MMSE), Hospital Anxiety and Depression Scale (HADS), and adherence to the intervention.
Results: Of the 362 patients included in the study, 177 were assigned to the intervention. The mean age was 71.7 years (SD 11.3) and 39.5% were female. The adjusted mean difference between groups for TMT A was 8.54 (95%CI 0.7 to 6.3), p = 0.032, for TMT B 8.6 (95%CI –16.5 to 33.6), p = 0.50, for MMSE –0.1 (95%CI –0.8 to 0. 6), p = 0.77, for HADS A –0.2 (95%CI –0.9 to 0.5), p = 0.56 and for HADS D –0.1 (95%CI –0.7 to 0.5), p = 0.76). A higher level of adherence to the intervention was significantly associated with increased MMSE (B = 0.030 (95%CI 0.005–0.055), p = 0.020).
Conclusion: No clinically relevant effects on cognitive or emotional function were found of individualized regular coaching for physical activity and exercise. However, increased adherence to the intervention was associated with improved cognitive function.
Key words: stroke; intervention; physical activity; cognition.
Accepted Jul 17, 2019; Epub ahead of print Aug 20, 2019
J Rehabil Med 2019; 51: 00–00
Correspondence address: Hege Ihle-Hansen, Department of Medicine, Oslo University Hospital, Postboks 4950 Nydalen, NO-0424 Oslo, Norway. E-mail: hmihle@ous-hf.no
Physical activity may help to keep the brain healthier and preserve cognitive ability and mood years after a stroke. In The Life After STroke (LAST) study, stroke survivors were allocated into 2 groups. A training group was encouraged to perform physical activity for 30 min daily, and 45–60 min of moderate-to-intense physical exercise every week. A control group was followed by their general practitioner as usual. This study aimed to measure the effect on cognitive and emotional function in both groups after 18 months. Of the 362 participants, almost half were in the training group. The mean age was 72 years and 40% were female. There were no differences between the groups regarding effect on cognitive or emotional function. In conclusion, this study did not show an effect of the physical training programme on cognition or mood after stroke.
Physical activity and exercise is recommended to stroke survivors for prevention of stroke recurrence (1) and to improve functional outcome (2). Best practice recommendations include promotion of physical activity and advice to engage in regular exercise of moderate-to-high intensity levels on most days of the week (1). However, the levels of intensity in post-stroke physical activity are often light-to-moderate (3).
Interventions based on risk assessment and risk factor management post-stroke are increasingly common, with stroke recurrence or physical function as outcome (4, 5). Prevention of cognitive decline in high-risk persons is shown to be possible when physical, cognitive, vascular and nutritional interventions are given regularly (6). A recently published meta-analysis of randomized controlled trials (RCTs) showed a positive effect of physical activity on cognitive performance post-stroke (7), especially on attention and processing speed and through programmes combining aerobic interventions and stretching. However, the included studies involved young patients, small sample sizes, and interventions lasting from 4 to 24 weeks. So far, multifactorial interventions aiming to prevent post-stroke cognitive decline have not been shown to be effective, possibly due to heterogeneity, short follow-ups, and low intensity (8).
The Life After STroke (LAST) study assessed the effect on motor function of individualized regular coaching on physical activity and exercise for 18 months post-stroke (9). Despite neutral results on primary outcome, the aim of the current study was to investigate whether the intervention could improve cognitive or emotional function in stroke survivors. In addition, this study explored the association between adherence to the intervention and the outcome variables.
LAST is a prospective, randomized, single-blinded, multicentre, 2-arm parallel group clinical trial. Between October 2011 and January 2016, patients were recruited 3 months post-stroke from 2 Norwegian hospitals; Trondheim University Hospital and Bærum Hospital with intervention and follow-up for 18 months in the primary healthcare services in the municipalities of Trondheim, Asker and Bærum (NCT01467206) (10). The current study analysed secondary outcomes.
Participants
Inclusion criteria were: patients aged over 18 years, with first-ever or recurrent stroke due to infarction and intracerebral haemorrhage, community-dwelling with modified Rankin Scale (mRS) score < 5. Exclusion criteria were serious medical co-morbidity with short life-expectancy, cognitive deficits, as evaluated by Mini Mental State Examination (MMSE) < 21 points (or < 17 points for patients with aphasia) and contraindication to participate in motor training (10). Neurological impairment was measured by the National Institute of Health Stroke Scale (NIHSS), which ranges from zero to 42. The patients were treated in the acute and subacute phase according to international and national guidelines from 2011 (11). Risk assessment and individualized secondary prevention was initiated at discharge from hospital after the index stroke, with recommendation for long-term risk factor control as part of usual care.
Randomization
Participants were stratified according to functional level post-stroke (mRS > 2 points), age ≥ 80 years and recruitment site, and randomized by a web-based randomization system developed and administered by the Unit of Applied Clinical Research, Faculty of Medicine and Health Sciences, Norwegian University of Science and Technology, Trondheim, Norway. Patients randomized to the control group received usual care.
Intervention
In addition to usual care, the intervention group received regular individualized coaching performed by physiotherapists, aiming to achieve physical activity 30 min daily, and 45–60 min physical exercise including 2–3 bouts of vigorous activity every week. The intervention did not include supervised or observed training. The physiotherapists carried out home visits to provide education and tailored training programmes, based on the patient’s preferences and goals. The patients were encouraged to report their activities in standardized training diaries. The patients had a monthly meeting with their coach, going through training diaries, with reassessment according to needs. These meetings were face-to-face in the first 6 months. For the next 6 months, every second meeting could take place as a phone meeting. During the final 6 months, 4 of the 6 meetings could take place as a phone meeting.
Outcomes
Cognitive function was measured using standardized neuropsychological tests assessing for global function, processing speed and executive function (normal scores); MMSE (minimum score 0 to maximum score 30), Trail Making A and B (TMT A (< 60 s considered a normal score) and B (< 180 s considered a normal score) (12, 13) at inclusion 3 months post-stroke and at 18 months follow-up. Symptoms of anxiety and depression were assessed by Hospital Anxiety and Depression Scale (HADS A and D) (14). Each domain consists of 7 questions with scores ranging from 0 (no symptoms) to 3 points. The outcomes were changes in cognitive and emotional measures from baseline to 18 months follow-up.
Adherence to the intervention was measured using self-reported activity through the diaries and evaluation by the physiotherapists, defined as the number of weeks patients in the intervention group completed at least 210 min of physical activity (minimum 30 min every day) and 45 min of exercise (in total per week). Despite considerable variation, it has been shown that the participants established and maintained moderate-to-good adherence to the intervention (15).
Statistical analyses
Sample size was calculated according to the primary outcome (Motor Assessment Scale) in the main study (9). Descriptive statistics are given as mean (SD), median (interquartile range), or frequency (percentage), where relevant. According to the CONSORT instructions, all outcomes underwent intention-to-treat (ITT) analysis (16). Linear regression analyses were used, with TMT A and B, MMSE and HADS A and D, respectively, as dependent variables, and intervention group, age, sex, stroke severity (measured by mRS), hospital site, treatment group, and cognitive or emotional status at inclusion as covariates.
For patients in the treatment arm, linear regression analyses were carried out with the cognitive and emotional outcome measures, TMT A, TMT B, MMSE, HADS A, and HADS D, at 18-month follow-up from baseline, as dependent variables, 1 at a time, with adherence to physical activity and exercise as primary covariate. These regression analyses were carried out both unadjusted and adjusted for the following covariates, one at a time and simultaneously: age, sex, mRS, MMSE, if appropriate, and the corresponding outcome variable score, all measured at baseline 3 months post-stroke.
On HADS and MMSE, the subjects with less than 50% missing values on a scale, the missing values were imputed singly using the expectation–maximization algorithm on that scale. Thereafter, multiple imputation was used to impute missing scale sums and other missing values, with m = 100 imputation, as recommended by van Buuren (17). Patients who died during follow-up were excluded from the analyses. The normality of residuals was checked by visual inspection of QQ plots. Two-sided p-values < 0.05 were considered statistically significant, and 95% confidence intervals (95% CI) are reported where relevant.
Ethics
The study was approved by the Regional Committee of Medical and Health Research Ethics (REK no 2011/1427) and registered with ClinicalTrias.gov, number NCT01467206. All participants provided informed consent.
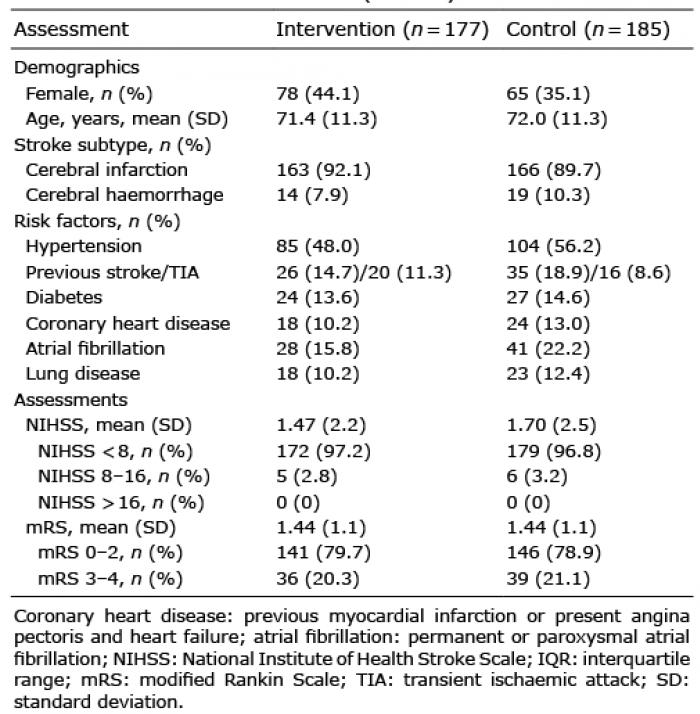
In total, 380 patients were recruited and randomized in the main study (the trial profile is reported elsewhere; 186 patient were randomised to intervention and 194 to standard care (9). After exclusion of 18 patients who died during follow-up (9 from the control group and 9 from the intervention group), 362 patients were included in these ITT analyses; 185 were assigned to control and 177 to intervention. Mean age was 71.7 years (SD 11.3), 39.5% were female and 329 (90.9%) had had ischaemic stroke. The baseline characteristics are shown in Table I.
Table I. Baseline characteristics (n = 362)
Measures of cognitive function and emotional symptoms showed a slight decline in both groups during follow-up (Table II). The adjusted mean difference between groups for TMT A was 8.54 (95% CI 0.7 to 16.3), p = 0.032, for TMT B 8.6 (95% CI –16.5 to 33.6), p = 0.50, for MMSE –0.1 (95% CI –0.8 to 0.6), p = 0.77, for HADS A –0.2 (95% CI –0.9 to 0.5), p = 0.456 and for HADS D –0.1 (95% CI –0.7 to 0.5), p = 0.76). The results based on multiple imputations are presented in Table II. The results from complete case analyses showed the same trends (data not shown).
Table II. Results of the intervention. Analyses based on multiple imputation of missing values
Unadjusted regression analysis applied to the intervention arm showed a significant association between increasing adherence to the intervention and improvement on TMT A, TMT B and MMSE. However, only MMSE remained significant in the adjusted analysis (B = 0.030 (95% CI 0.005–0.055, p = 0.020) (Table III).
This study investigated the effectiveness of an individualized physical activity and exercise intervention programme on cognitive and emotional function post-stroke compared with usual care. The intervention involved regular coaching to perform 30 min physical activity daily every day and 45–60 min of physical exercise with 2–3 bouts of vigorous intensity levels every week. No clinically relevant effect of this programme was found on cognitive or emotional functioning after 18 months compared with usual care. However, regression analysis applied to the treatment arm only showed a positive association between increasing adherence to the intervention and cognitive function.
To our knowledge, this is the first RCT to investigate the effect of a long-term physical activity programme on cognitive and emotional function post-stroke in a rather large cohort with high mean age. The lack of clinical impact on cognitive measures is in line with the neutral results shown by the primary and secondary functional measures (9). There was no effect on emotional function, which is in contrast to a recent study published by Graven et al. (18), who also included life-management, barriers and social network. How-ever, our explorative analysis showed an association between good adherence to the intervention and better cognitive function, in line with the findings from the meta-analysis (7).
Since motor recovery after stroke tends to reach a plateau phase after 10 weeks (19), the initial improvement in cognitive function may follow a similar pattern (20), suggesting that earlier initiation, and perhaps more specific and intensive, future interventions would be beneficial. In addition, the intervention was based on patient’s preferences more than the type of training aiming at cognitive gain. Combining aerobic exercise with other training programmes seems to achieve better cognitive function and might be applied in future trials (7, 21).
The lack of effect on cognition might be explained by lack of adherence to the intervention. However, another possible explanation for no effect on cognition is the heterogeneity of the stroke population and, probably also, the underlying brain pathology (22). Theoretically, the effect of physical activity on brain function includes neurogenesis, building brain reserve, angiogenesis and prevention of progressive small vessel disease (23). Light-to-moderate physical activity may represent a treatment strategy less likely to affect the underlying pathology in the chronic phase. How-ever, it might halt or slow decline through building brain reserve and thereby delay symptom onset. A potential benefit on vascular pathology, to prevent cognitive dysfunction due to chronic cerebral hypoperfusion may need longer follow-up. Physical activity could have a beneficial effect on cognitive flexibility and brain reserve, but an effect through neurogenesis and angiogenesis may be achieved through interventions with higher intensities (22). Secondary prevention after cerebrovascular disease involves both pharmacological treatment and interventions for behaviourally modifiable risk factors (24). A multimodal individualized intervention including optimal medication, dietary, social and cognitive stimulation in addition to physical activity might also be needed to improve cognition after stroke, perhaps with longer follow-up (25–27).
Post-stroke, there is also a wide spectrum of neuropsychological manifestations. Apparent brain damage gives rise to different cognitive deficits, especially executive function, attention and processing speed and working memory (28, 29). It is a limitation that HADS, MMSE and the Trail Making Tests are primarily designed as screening tools and might not be sensitive to detect changes that occur during follow-up after stroke. Hence, future research should investigate the psychometric properties of these measures in the stroke population. Furthermore, the study population may, due to the rather high mean age, have been too heterogeneous regarding both underlying additional degeneration and comorbidities. In addition, the study was designed or powered for a potential effect on functional outcome, and length of education was not registered. Furthermore, functional impairments in the dominant arm/hand may have affected the results on the cognitive test performance. The intervention was individualized coaching on physical activity and exercise, and did not include supervised exercise. Therefore, the actual performed training is self-reported regarding both length and intensity. Finally, only mild-to-moderate strokes were included, pre-stroke disability and comorbidities were not assessed, and the generalizability of the results may be affected by the fact that our sample may have been more motivated to undertake physical activity and exercise regardless of the result of the randomization.
In conclusion, this study found no effect of the intervention on cognitive function post-stroke compared with usual care. However, increased adherence to physical activity and exercise was associated with improved cognitive function, indicating that the intervention dose might be of importance to achieve a benefit. Future preventive trials should include education regarding healthy lifestyle and focus on motivation to adhere to the physical programme over time. In addition, participants should be stratified into subgroups based on supposed reversibility, especially those with small-vessel disease or pure vascular pathology, in order to prevent further decline.
The LAST study was funded by Norwegian Research Council, Liaison Committee between Central Norway Regional Health Authority and Norwegian University of Science and Technology (NTNU), Joint Research Committee between St Olav’s Hospital and NTNU, Norwegian Fund for Postgraduate Training in Physiotherapy, and Stroke Unit Research Fund at St Olav’s Hospital. The funders of the study had no role in study design, data collection, data interpretation, or writing of the report.
LAST Collaboration Group: Torgeir Engstad, Jon Magnussen, Anne Hansen, Rune Schjørlien, Stian Engen, Randi Moxnes Osmundnes, Anne-Britt Olerud, Camilla Knudsen, Trine Hansen, Walburga Schroeter, Gro Stensrud Fjelldal, Kristin Hovde, Kristine Helen Reneflot, Lisa Wennberg, Ole Petter Norvang, Ailan Phan, John Bjørn Storvoll, Brede Ørjaset, Marianne Syvertsen, Ingvild Berger, Anne Eitrem Dahl, Christine Lundemo Sandø, Veronica Kjølstad, Alexander Hansen, Helene Kverne Vileid, Maren Hjelle Giddal, Anne Wergeland, Anne Mette Brenden, Julie Bernhardt, Peter Langhorne.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize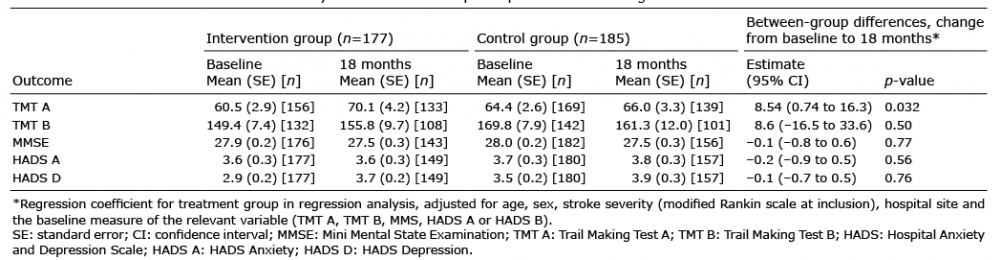 Click to show fullsize
Click to show fullsize