
From the 1Department of Neurology and Tianjin Neurological Institute, 2Department of Rehabilitation, Tianjin Medical University General Hospital, and 3Department of Paediatrics, Tianjin Hospital of ITCWM Nankai Hospital, Tianjin, China
Objective: To provide detailed data on the effects of multidisciplinary rehabilitation for patients with neuromyelitis optica spectrum disorder with moderate to severe disability.
Design: A pilot randomized control study.
Subjects/patients: A total of 39 patients with neuromyelitis optica spectrum disorder were randomized into intervention or control groups.
Methods: The intervention group received multidisciplinary rehabilitation 5 times/week for 4 weeks in a hospital, and the patients were guided to continue community- or home-based rehabilitation for 3 months. The control group did not receive any specific rehabilitation intervention. Disability was assessed using the Extended Disability Status Scale (EDSS) and Functional Systems (FS) scores after 4 weeks of rehabilitation and 3 months of follow-up.
Results: The mean EDSS score was 7.5 at admission for both groups. Improvements (p<0.05) in the EDSS score and domains of bowel, bladder and motor functions (pyramidal and walking function) were noted in the multidisciplinary rehabilitation group after 4 weeks. After 3 months, the patients in the usual care group showed improvement in EDSS score and walking ability score; however, no significant changes in other variables were noted.
Conclusion: These results suggest that multidisciplinary rehabilitation potentially promotes motor functional recovery in patients with neuromyelitis optica spectrum disorders.
Key words: neuromyelitis optica spectrum disorders; multidisciplinary rehabilitation; disability.
Accepted Jul 17, 2019; E-pub ahead of print Aug 16, 2019
J Rehabil Med 2019; 51: 00–00
Correspondence address: Li Yang, Department of Neurology and Tianjin Neurological Institute, Tianjin Medical University General Hospital, Tianjin 300052, China. E-mail: yangli2001@tmu.edu.cn
The aim of this study is to investigate the effects of multidisciplinary rehabilitation for patients with neuromyelitis optica spectrum disorders who have moderate to severe disability. In 39 patients with neuromyelitis optica spectrum disorders, disability was assessed after 4 weeks of rehabilitation and 3 months of follow-up. In the patients who underwent multidisciplinary rehabilitation, bowel and bladder and motor functions (pyramidal and walking function) were improved compared with those with usual care. These results confirm the short-term effectiveness of multidisciplinary rehabilitation in patients with neuromyelitis optica spectrum disorders in terms of improving impairment. The results also suggest that multidisciplinary rehabilitation is a safe and feasible therapy for adults with neuromyelitis optica who have severe disability.
Neuromyelitis optica (NMO) is an inflammatory disease of the central nervous system that selectively targets the optic nerve and spinal cord (1). In 2007, the term NMO spectrum disorders (NMOSD) was introduced to include AQP4-IgG-seropositive patients with limited or inaugural forms of NMO (e.g. first-attack longitudinally extensive transverse myelitis (LETM) or recurrent or bilateral optic neuritis) who were at high risk of future attacks (2). NMOSD is relatively frequent worldwide. In Asia, NMOSD represents approximately 50% of all demyelinating disorders (3). NMOSD displays a relapsing-remitting course (2), and severe disability remained after immunotherapy with recurring relapse (4). Moreover, a large number of studies have shown that patients with multiple sclerosis, the most common demyelinating disorder of the central nervous system, can benefit from rehabilitation therapy (5–8). However, evidence regarding the benefits of rehabilitation in patients with NMOSD remains insufficient.
EDSS is the standard for evaluating the clinical treatment of multiple sclerosis, while NMO and multiple sclerosis (MS) are both demyelinating diseases of the central nervous system. However, few studies have used the Expanded Disability Status Scale (EDSS) to evaluate disability after multidisciplinary rehabilitation (MDR) in patients with NMOSD. In addition, the effect of MDR treatment on NMOSD is unclear. Hence, the aims of this study were: (i) to evaluate the effectiveness of MDR rehabilitation therapy in patients with NMOSD; and (ii) to explore which functional systems may benefit from MDR in patients with NMOSD.
Participants and clinical parameters
A total of 39 consecutive patients with NMOSD were recruited from the Neurology Department of Tianjin Medical University General Hospital from January 2014 to November 2016. The diagnosis of NMOSD fulfilled the 2015 Wingerchuk criteria (9). The inclusion criteria for this study were: (i) disability as a result of NMOSD (4≤ EDSS score ≤9); (ii) patient receiving 500 mg methylprednisolone intravenously, which was reduced by half every 3 days, followed by a gradual tapering until 40 mg was reached (14–16 days from the acute attack). The exclusion criteria were: (i) acute attack within 14 days; (ii) other conditions that may affect motor function or impaired cognitive functioning; (iii) severe concurrent diseases (i.e. cancer, cardiopulmonary diseases or severe psychiatric disorders). The subjects were divided randomly into 2 groups: a rehabilitation group (MDR) and a control group (usual care; UC). A random sequence was created by a computer. Patients in the UC refused or voluntarily ceased rehabilitation treatment (due to dissatisfaction or for economic reasons).
Demographic and clinical data, including sex, age, and disease duration, were collected. Informed consent was obtained from all participants, and the study was approved by the Tianjin Medical University General Hospital institutional review board and ethics committee.
Intervention
Multidisciplinary rehabilitation (MDR). Medical rehabilitation is defined as “a set of measures that assist individuals who experience disability to achieve and maintain optimal physical, sensory, intellectual, psychological and social functioning in interaction with their environment” (8). Since clinical manifestations of NMO and MS overlap and NMO was thought to be a variant of MS, some rehabilitation therapies in this study were co-opted from treatments used for MS and NMO.
For pyramidal function and walking ability, patients were offered physiotherapy. Physiotherapy typically involved at least 30 min of daily exercise. These exercises included active or passive range-of-motion exercises; strengthening exercises; hand function exercises; transfer exercises; balance training aimed at increasing muscle strength, improving balance and gait, decreasing spasticity and improving functional activities of daily living; and 20 min of robot-assisted gait training according to the patient’s needs. In addition, occupational, cognitive, respiratory and/or phoniatric therapy were provided when necessary (10).
For sensory function, patients were provided sensory re-education techniques and occupational therapy.
For bladder and bowel, patients received physical treatments, including pelvic floor exercises and/or intermittent cleaning and/or self-catheterization (11, 12), according to their dysfunction.
Patients were allowed to rest before becoming fatigued. Multidisciplinary inpatient rehabilitation was performed 5 days/week for 2–4 h/day for 4 weeks. After 4-week inpatient rehabilitation, the patients were guided to continue community or home-based rehabilitation (walking training, wheelchair operation training) for 3 months.
Robot-assisted gait training: LokoHelp (Germany)(13) practical design offered therapists economically feasible access to quick and convenient body weight support (BWS), including ergonomically adjustable seating for assistance with manual treatment. This training was performed in the hospital.
Usual care. The control group (usual care; UC) did not receive any specific rehabilitation treatment for gait performance and mobility improvement.
During the entire study, both groups were authorized, at will, to exercise in non-rehabilitative contexts.
Outcome measures
NMOSD impairment was evaluated using EDSS and Functional Systems (FS) scores before the treatment and 4 weeks and 3 months after the treatment. EDSS is based on a detailed neurological examination that combines impairment and disability on a 10-step ordinal scale, ranging from 0 (normal) to 10 (death), and was performed by 2 neurologists who were both certified by Neurostatus for EDSS competency (14, 15). The patients’ FS were described on 8 subscales, including visual (or optic) functions, brain stem functions, pyramidal functions, sensory functions, bowel and bladder functions, cerebellum functions, cerebral (or mental) functions, and walking functions. If the walking distance is < 500 m, the EDSS score depends on walking ability (16). The EDSS scores were evaluated at the start and end of the training period.
Statistical analysis
The data for the MDR group were compared with the respective results of the parallel UC group. Descriptive statistics (median, minimum and maximum) are given for all variables. Non-parametric testing (Wilcoxon signed-rank) was performed to compare the EDSS and FS scores. A p-value of 0.05 or less was considered significant for all statistical analyses. All statistical analyses and graphs were performed using GraphPad PRISM 5 (Graph Pad Software Inc., San Diego, CA, USA).
Demographic and clinical features
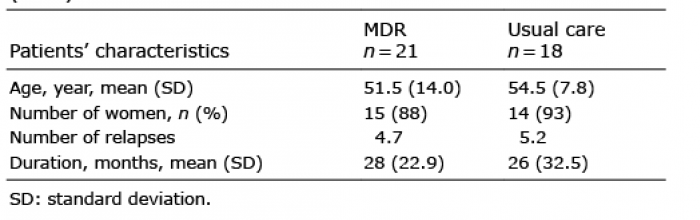
A total of 39 patients with NMOSD were assessed for eligibility and randomized into 2 groups: an MDR group (n = 21) and a UC group (n = 18). One patient in the MDR group and one patient in the control group were lost at the 4-week assessment due to relapse. Three patients in the MDR group and 2 patients in the UC group dropped out due to refusal to continue, and these patients did not perform evaluations at 3 months (Fig. 1). The patients’ demographic and clinical characteristics are reported in Table I. In total, 39 patients with NMOSD (29 females, 10 males) were included in the study. A final total of 32 patients completed the study. The median EDSS score at admission was 7.5 (range 6.0–9.0) All patients with NMOSD had lesions in the spinal cord. No statistically significant baseline differences between 2 groups were found at baseline (Fig. 2).
Table I. Baseline characteristics of people with neuromyelitis optica spectrum disorders allocated to multidisciplinary rehabilitation (MDR) or usual care
Fig. 1. CONSORT diagram for multimodal exercise training intervention.
Table II shows the median EDSS and FS scores for the MDR and UC groups before treatment. No statistically significant baseline differences were found between the 2 groups (p > 0.05). EDSS and FS scores are shown in Table III and Fig. 3.
Table II. Extended Disability Status Scale (EDSS) and Functional System scores to multidisciplinary rehabilitation (MDR) or usual care (UC) before treatment
Table III. Changes in Extended Disability Status Scale (EDSS) and Functional System (FS) scores after treatment
Fig. 2. Extended Disability Status Scale (EDSS) and Functional System (FS) scores for the multidisciplinary rehabilitation (MDR) (n = 21) or usual care (UC) (n = 18) groups before and after 4 or 12 weeks of MDR treatment. Numbers are statistically reported as the mean and standard deviation (SD). ***p < 0.001; **p < 0.01; ***p < 0.05. FS-WA: walking function. FS-PF: pyramidal functions. FS-SF: sensory functions. FS-BB: bowel and bladder functions. FS-CF: cerebral (or mental) functions.
Fig. 3. Extended Disability Status Scale (EDSS) and Functional System (FS) scores for multidisciplinary rehabilitation (MDR) (n = 21) before and after 4 or 12 weeks of MDR treatment. Numbers are statistically reported as mean and standard deviation (SD). ***p < 0.001; **p < 0.01; ***p < 0.05. FS-WA: walking function. FS-PF: pyramidal functions. FS-SF: sensory functions. FS-BB: bowel and bladder functions. FS-CF: cerebral (or mental) functions.
The results showed significant differences between the 2 groups in EDSS total scores, walking ability scores. Furthermore, the patients in the MDR group recovered faster than those in the UC group. Neither the patients in the MDR group nor those in the UC group showed a statistically significant change in median scores for sensory function.
Following the 4-week MDR treatment, a significant improvement in the EDSS was observed compared with that at admission in the MDR group (p < 0.001). Moreover, in the subscale analyses, significant improvements were demonstrated in bowel and bladder function, pyramidal function, and walking function scores in patients in the MDR group (2 to 1.5, p = 0.001; 4.0 to 3.0, p < 0.001; and 7.5 to 7.0, p = 0.003; respectively), while sensory function and cerebral (or mental) func-tion remained unchanged (3 to 3, p = 0.083; 2.0 to 1.0, p = 0.083; respectively). Furthermore, after 3 months of treatment, the trends in the FS were the same as those at discharge, except that fatigue in the cerebral (or mental) function score had improved (from 2.0 to 1.0, p = 0.002; Table IV).
In the UC group, no significant differences in the EDSS scores and FS scores were noted after 4 weeks (p > 0.05). However, significant improvements in the EDSS scores, pyramidal function, and walking function scores were noted after 3 months.
Table shows the differences in the changes in median scores between the 2 groups at 4 weeks, 3 months and baseline.
Table IV. Extended Disability Status Scale (EDSS) and Functional System (FS) scores to multidisciplinary rehabilitation (MDR) or usual care (UC) 4 week after MDR
This study demonstrated the benefit of MDR in patients with disability resulting from NMOSD, as assessed by EDSS and FS. The study also suggested that MDR was effective in improving the clinical status of patients with NMOSD in terms of impairments. In the UC group, the EDSS score did not change at 4 weeks and improved at 3 months, which indicated that patients with MNOSD are taking corticosteroids (1 month) and exhibit a certain degree of self-healing ability (3 months) (17). The EDSS score improved at 4 weeks after treatment in the MDR group, which indicated that rehabilitation treatment promotes or speeds up the patient’s recovery process. Moreover, the results indicated that the bowel and bladder, pyramidal, and walking functions of patients with NMOSD might recover after 4 weeks with MDR treatment.
To the best of our knowledge, this is the first study investigating which FS may benefit more from MDR treatment in an NMO population in MDR programmes. Three previous studies (2 case reports and 1 research article) described the rehabilitation outcomes of patients with NMO. One case report on the effect of vibration stimulation (VS) on NMO discovered that standing up and walking performance improved with VS, and this finding may support the hypothesis of neuronal plasticity on central pattern generators by VS (18). Plasticity is a result of the creation of new circuitry through sprouting and alterations of synaptic strength. Appropriate rehabilitation could modify and enhance the plasticity process (19). Vahdat and colleagues provided strong evidence for local spinal plasticity over the course of human motor learning using functional magnetic resonance imaging (20). Similarly, Nechemia et al. (21) described 15 in-patients with NMO and 32 in-patients with MS who received MDR and found that both groups benefitted. Moreover, at discharge, the NMOSD group showed greater improvement in FIM scores and lower EDSS scores.
The current study investigated bowel and bladder, cerebral (or mental), pyramidal, and walking functions, which may benefit more from MDR. However, sensory dysfunction required the longest period for recovery. Intermittent catheterization, suprapubic tapping, and physical treatments, including pelvic floor exercises, have been applied to aid voiding for urinary retention. Thus, bowel and bladder functions were improved. Similarly, a systematic review reported that physical therapy techniques were effective for urinary disorders in MS populations with mild disability (22).
Walking function is a central outcome of rehabilitation intervention (23). Grasso and colleagues suggested that rehabilitation for patients with MS should be initiated early while the patient can walk independently or with assistance and lacks severe sphincteric and cognitive deficits (23). Accordingly, in this study, patients with NMOSD received MDR immediately after they completed high-dose intravenous methylprednisolone therapy (2–3 weeks after the acute attack). The regimen achieved a good effect, even compared with previous trials implementing rehabilitation in the MS population (24). In the current study, patients’ disability levels were more severe (EDSS score ≥ 6). Furthermore, there were no adverse events during the entire rehabilitation programme, indicating that it is relatively safe and effective to introduce MDR early to adults with NMOSD despite severe disability. Nechemia et al. reported that inpatient MDR programmes available for patients with MS might be implemented successfully for patients with NMO (21). In the control group, some patients exhibited improvements in walking ability scores and pyramidal function. We hypothesize that this therapy may affect the natural course of the disease.
Sensory function recovery may occur over a long time, and these changes may have cumulative effects. Given the poor results for sensory function rehabilitation, we hypothesize that 4 weeks is not sufficient for the amelioration of this disability, but continued therapy may offer promising results.
None of the patients in our study had cognitive impairment (MMSE score > 27), but all had fatigue to different degrees. After 4 weeks of MDR, no obvious changes in patient fatigue were observed. This finding suggested that rehabilitation training did not exacerbate fatigue. However, after 3 months, the fatigue was resolved to varying degrees. Rehabilitation with a focus on relieving fatigue via an improvement in mood and cardiovascular reconditioning was previously reported by Judica & Romberg (25, 26). Therefore, our results indicated that training for patients with NMOSD should be continued in both hospital and home or community settings in order to maintain these benefits.
In this study, EDSS was applied to the evaluation of NMOSD. The EDSS provided a detailed evaluation (the 8 major system dysfunctions in MS are involved) (27). However, the EDSS has the disadvantage that it depends only on walking function in severe dysfunction (e.g. EDSS ≥ 6 points); therefore, the EDSS score cannot reflect the situation in which the walking function has not changed but other system functions have improved. Therefore, there is a need to modify the EDSS for use in the evaluation of NMOSD.
Study limitations
This study has some limitations. Most of the patients exhibited more serious disability (EDSS ≥ 6), which may affect the overall rehabilitation outcome (see above). Furthermore, NMOSD is a rare disease; therefore, the sample was small. A well-designed study should be performed on MDR of patients with NMOSD at different levels of disability. In future clinical trials, studies should compare the effectiveness of MDR in treating different degrees of NMOSD, and further research is required into the rationality of EDSS as an indicator for evaluating NMOSD.
Conclusion
This study confirmed the short-term effectiveness of MDR in patients with NMOSD in terms of improving impairment, as determined using the EDSS. Bowel and bladder, cerebral (or mental), pyramidal, and walking functions may benefit more from MDR, while sensory dysfunction required the longest period for recovery. The control group showed some improvement in walking ability scores and pyramidal function, although this improvement may be an effect of the natural course of disease.
Although this study is a pilot trial, the results suggest that MDR is a safe and feasible therapy for adults with NMOSD with severe disability. These primary observations will be helpful to all medical practitioners treating MDR in patients with NMOSD, and they advocate that patients with NMOSD should be candidates for early MDR in order to prevent the progression of neurological disability. A randomized controlled clinical trial should be performed to confirm these preliminary findings.
The authors wish to thank all participants in this research and all the staff and students involved in data collection.
This study was supported by the Tianjin Research Program of Application Foundation and Advanced Technology (15JCZDJC35700), the National Science Foundation of China (81171363 to L.Y.), and the National Key Clinical Specialty Construction Project of China.


 Click to show fullsize
Click to show fullsize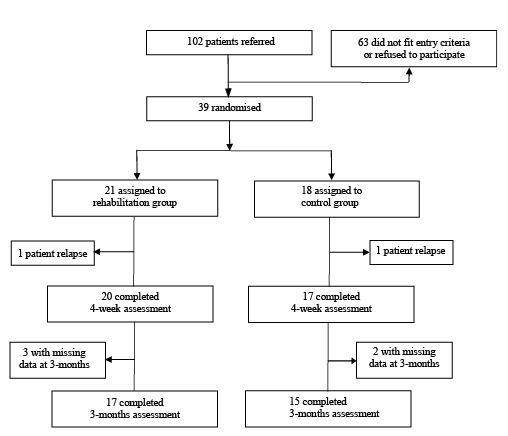 Click to show fullsize
Click to show fullsize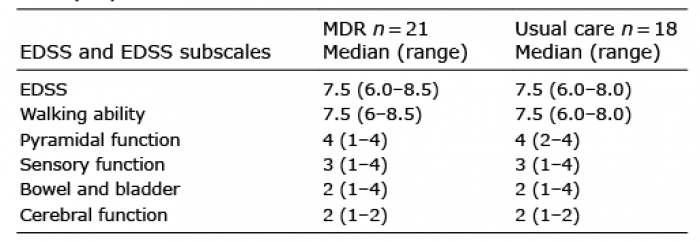 Click to show fullsize
Click to show fullsize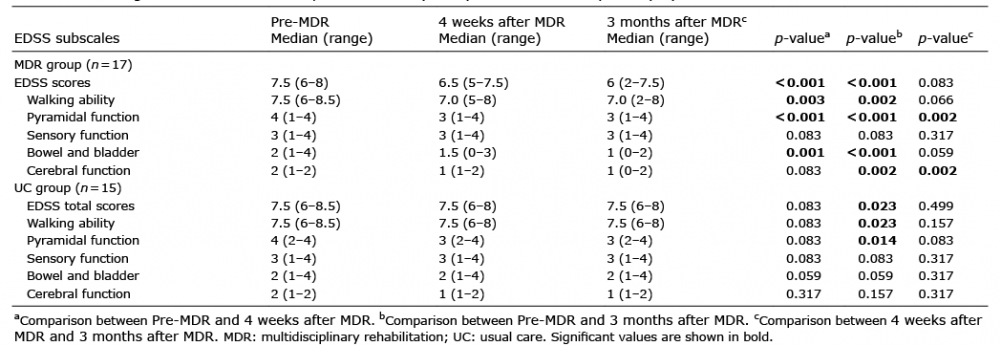 Click to show fullsize
Click to show fullsize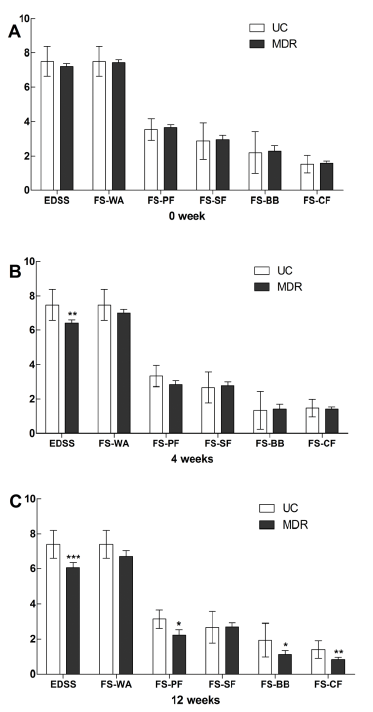 Click to show fullsize
Click to show fullsize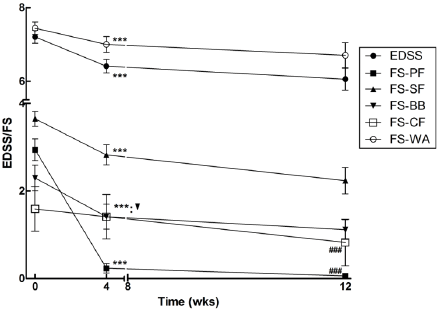 Click to show fullsize
Click to show fullsize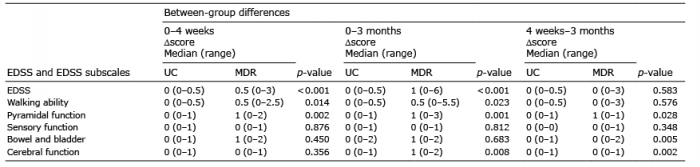 Click to show fullsize
Click to show fullsize