
From the 1Department of Rehabilitation and Brain Trauma, Division of Clinical Neurosciences, Turku University Hospital and University of Turku, 2Department of Biostatistics, University of Turku and 3Department of Physical and Rehabilitation Medicine, Turku University Hospital and University of Turku, Turku, Finland
Objective: To compare short generic International Classification of Functioning, Disability and Health (ICF)-based measures of functioning with traditional measures of stroke severity and dependence in subacute stroke.
Methods: In this cross-sectional study patients with stroke (n = 195) and their significant others completed the 12-item World Health Organization Disability Assessment Schedule (WHODAS 2.0) at discharge from rehabilitation. A neurologist assessed functioning with the 7-item World Health Organization (WHO) Minimal Generic Set of domains of functioning and health. These scores were compared with assessments of severity of stroke (National Institutes of Health Stroke Scale; NIHSS) and dependence (modified Rankin Scale; mRS; and Functional Independence Measure; FIM).
Results: From mild to severe stroke, increasing disability was found in single items and sum scores of WHODAS and the WHO Minimal Generic Set. Al-though proxies rated 6 out of the 12 separate WHODAS functions more impaired than did the patients, correlations between the different measures (proxy- and patient-WHODAS, the WHO Minimal Generic Set, mRS, NIHSS and FIM total and sub-scores) were strong to very strong, except for moderate correlations between patient-WHODAS, and NIHSS or FIM cognitive sub-score.
Conclusion: Despite their brevity, both generic ICF-based tools were useful in finding disabilities for patient- and family-centred goal-setting and service-planning after subacute rehabilitation.
Key words: disability; Functional Independence Measure; modified Rankin Scale; National Institutes of Health Stroke Scale; stroke; subacute; WHODAS; WHO Minimal Generic Set of domains of functioning and health
Accepted Jul 4, 2019; Epub ahead of print Aug 12, 2019
J Rehabil Med 2019; 51: 00–00
Correspondence address: Sinikka Tarvonen-Schröder, Division of Clinical Neurosciences, Turku University Hospital, PO Box 52, FI-20521 Turku, Finland. E-mail: sinikka.tarvonen-schroder@tyks.fi
This study compared short generic International Classification of Functioning, Disability and Health (ICF)-based measures of functioning, the patient- and proxy-reported 12-item World Health Organization Disability Assessment Schedule (WHODAS 2.0) and the 7-item WHO Minimal Generic Set of domains of functioning and health assessed by a neurologist, with traditionally used measures of stroke in the subacute phase. Although proxies rated 6 out of 12 separate WHODAS functions more impaired than did the patients, the scores of patient- and proxy-reported WHODAS 2.0 and the WHO Minimal Generic Set correlated well with each other and with older measures of stroke severity (National Institutes of Health Stroke Scale) and dependence (modified Rankin Scale and Functional Independence Measure). Both ICF-based tools, despite their brevity, were useful in finding disabilities for patient- and family-centred goal-setting and service-planning after subacute stroke rehabilitation.
Stroke is a leading cause of severe long-term disability. The incidence of stroke is increasing globally, especially in low- and middle-income countries. At the same time, advances in healthcare, including the use of technology, have led to higher survival rates (1–3). Consequently, there is a greater demand for interdisciplinary rehabilitation and for individual goal-making and service-planning, in which patient- and family-centred functional assessments are needed.
There is a vast number of generic and specific scales and measures for post-stroke patients (4–7), but no gold standard or single instrument to address the concepts of medical and social disability as a composite of ICF domains body structure, functions, activity, and participation. However, all these aspects should be included in the assessment of recovery after stroke. The National Institutes of Health Stroke Scale (NIHSS) is the most widely used severity scale for acute and subacute stroke, also predicting survival, functional recovery and patient’s post-acute care disposition (5, 8–10). Although the NIHSS has been used as a tool for goal-setting and rehabilitative clinical decision-making, it is not directly associated with an individual’s ability to compensate for a neurological deficit, and therefore it is not an ideal measure of functional outcome after stroke (5). Hence, measures of dependence, such as modified Rankin Scale (mRS), Barthel Index (BI) and Functional Independence Measure (FIM) are widely used in stroke trials and rehabilitation (6, 8, 11, 12). However, measures of participation are not included in these traditional outcome measures (13, 14), although participation would appear to be the most meaningful measure for the patient (6). So far, there is no agreement about which critical measures should be routinely captured (4, 15, 16). Instead of a single instrument, a standard set of patient-centred and patient-reported outcome measures after stroke have been suggested to quantify outcomes accurately with validated instruments (16, 17).
To unify the assessment of functioning globally, regardless of health condition, the World Health Organization (WHO) has developed a generic patient- and proxy-reported instrument to measure both activities and participation, the WHO Disability Assessment Schedule (WHODAS 2.0), which has been validated in various conditions, including stroke (18). The short 12-item form of WHODAS 2.0 has been found to be practical for use in various clinical settings (19–24). Another short ICF-based instrument, the 7-item WHO Minimal Generic Set of domains of functioning and health, has been suggested for use as a starting point to address comparability of data across studies (25).
As far as we know, there are no studies investigating the utility of these 2 short ICF-based instruments in subacute stroke. It is essential to assess patient and proxy experiences of difficulties in activities and participation early in post-stroke rehabilitation in order to plan rehabilitation goals, discharge dispositions and future community services. To find suitable tools for this planning, we decided to compare these short ICF-based tools (the 12-item WHODAS 2.0 and the 7-item WHO Minimal Generic Set) at discharge from the stroke rehabilitation ward with 2 commonly used outcome measures of dependence, FIM and mRS, in different severity groups of stroke based on NIHSS score.
In this observational cross-sectional study, 195 consecutive patients in intensive subacute inpatient stroke rehabilitation were recruited between August 2015 and August 2018. Questionnaires, including the 12-item WHODAS 2.0 (18), and personal background information (age, sex, accommodation, marital status, educational level, and working status), along with informed consent, were completed by 167 (of 195) patients and 195 significant others at discharge from rehabilitation. Based on clinical judgement, 28 patients were not capable of completing the WHODAS scale because of the cognitive impairment caused by a severe stroke and aphasia (Table I). The patients and their significant others were blinded to each other’s evaluations. Clinical information (date of diagnosis and comorbidities) was gathered from the hospital records and by interviewing the patients and their significant others, and the total number of comorbidities was counted (26, 27). The stroke survivors (diagnosis according to the International Classification of Diseases, 10th revision (ICD-10) criteria) were mostly referred to the neurological rehabilitation unit from the acute stroke unit of the same university hospital. Sometimes the patient had to wait on a general ward for stabilization of the medical condition after acute stroke unit care before intensive rehabilitation or because of lack of capacity of the rehabilitation ward. For admission to intensive rehabilitation, the patients had to be able to sit for a minimum of 30 min. Exclusion criteria were age under 16 years at time of stroke onset, previous stroke, a current major medical or psychotic condition, or another neurological diagnosis with functional impairment, brain injury without radiological findings, and medical reasons for interrupted rehabilitation.
The severity of stroke was classified by a neurologist into mild, moderate or severe according to NIHSS (5) firstly in the acute phase (initial and 24-h NIHSS), and secondly on admission to rehabilitation unit. The participants were divided into 3 severity groups according to the 24-h NIHSS sum score (28); 0–5 was considered mild, 6–14 moderate, and 15–42 severe stroke.
At discharge from inpatient rehabilitation, a neurologist assessed the dependence of patients with the mRS, ranging from 0: no dependence to 6: death (5), and their disability with the 7-item WHO Minimal Generic Set (25). A rehabilitation nurse, trained as a FIM rater, assessed the level of dependence of each patient at admission and discharge using an electronic FIM tool (FIM™ version 5.2, Uniform Data System for Medical rehabilitation, Amherst, NY, USA) rating all items on a scale 1–7 (“total dependence” to “complete independence”) to sum score (18–126) and motor and cognitive sub-scores (29).
The 12-item WHODAS 2.0 includes 12 items assessing 6 disability domains in 2 components. The component “activities” includes cognition (learning and concentration), mobility (standing and walking) and self-care (washing and dressing oneself), and the component “participation” includes getting along (dealing with strangers and maintaining friendships), life activities (doing housework and working ability), and social participation (emotional functions and engaging in community). Each of the 12 items is rated according to a 5-point Likert-type scale, which grades the difficulty experienced by the participant in performing a given activity. The scoring is from 0 to 4, where 0 means no (0–4%), 1 means mild (5–24%), 2 means moderate (25–49%), 3 means severe (50–95%), and 4 means extreme or complete (96–100%) difficulty in this specific activity. The total score of WHODAS is the sum of all these 12 sub-scores and ranges from 0 to 48, with lower scores indicating better functioning. Total scores of 1–4 belong to mild disability, 5–9 to moderate disability, and 10–48 to severe disability (18, 19, 30, 31) (http//www.who.int/classifications/ICF/who/whodasii/en/).
The WHO Minimal Generic Set consists of 7 ICF domains: energy and drive functions, emotional functions, sensation of pain, carrying out daily routine, walking, moving around, and remunerative employment. Generic means that this assessment scale is applicable to all people despite of their health conditions. Minimal means that the scale consists of the least number of domains of functioning that can be used to explain significant differences between people with health issues. The scoring system is similar to WHODAS, the sum score ranging from 0 to 28, with lower scores indicating better functioning (25).
The ethics committee of the University of Turku and Turku University Hospital approved the study (19.5.2015, 73/2015). The ethical standards of the World Medical Association Declaration of Helsinki 1975, revised 1983, were followed.
Statistical analysis
Categorical variables were described using frequencies and percentages and, for continuous variables, medians with range of values and 25th and 75th percentiles were used. The comparison between different severity groups of stroke was carried out within categorical variables using χ2 test, or, in the case of small cell frequencies, Fisher’s exact test. In numerical variables the comparisons between the patient groups were carried out either by one-way analysis of variance, or by the non-parametric Kruskal–Wallis test when the distribution of an outcome variable was skewed. The Spearman correlation coefficient was used to test the correlation between variables. Correlations of 0–0.29 were considered weak, 0.30–0.49 moderate, 0.50–0.69 strong, and 0.70–1.00 very strong. Patient and proxy WHODAS responses were analysed pairwise using test of symmetry and weighted kappa (wK) coefficient to evaluate the correspondence of the answers of a patient and his or her proxy. Cronbach’s alpha was calculated to evaluate the reliability of WHODAS and the WHO Minimal Generic Set questionnaires. Statistical analyses were performed using SAS 9.4 for Windows. p-values below 0.05 (2-tailed) were considered statistically significant.
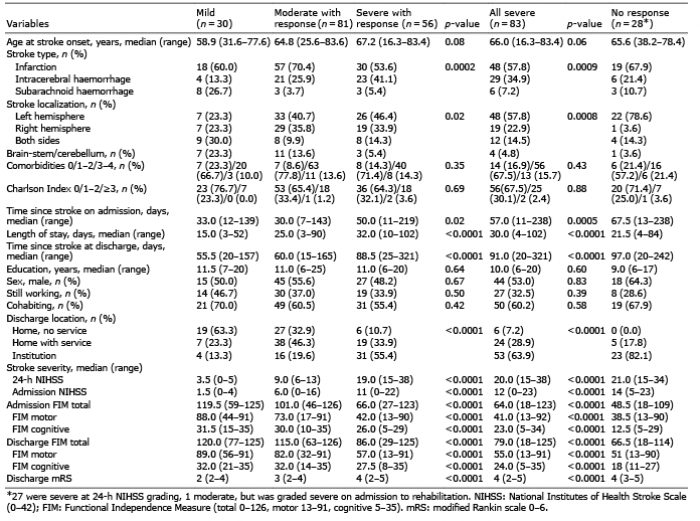
Demographic and clinical background data for all 195 patients are shown in Table I. Responses to the WHODAS questionnaire were received from 167 patients and from all 195 significant others. When comparing background data in different severity groups of stroke, rehabilitants with a WHODAS patient response were divided into 3 groups: 1: mild (n = 30), 2: moderate (n = 81), and 3: severe stroke (n = 56). Since the intention was for the study to cover all levels of severity of patients in intensive post-acute rehabilitation, including those with the most severe stroke and aphasia, an “all severe” group (n = 83) of significant others’ responses was also formed, consisting of all patients with severe stroke according to 24-h NIHSS, i.e. including also the 27 rehabilitants without a WHODAS patient response. Finally, a group of “patients not able to respond to WHODAS” questionnaire (n = 28, i.e. 27 with severe and one with moderate stroke at 24 h NIHSS assessment) with only significant others’ responses was formed.
Table I. Demographic and clinical data of the patients with mild, moderate, and severe stroke (according to the 24-h National Institutes of Health Stroke Scale; NIHSS)
When disability was rated by a physician (Table II), the overall disability and difficulties in all single items were found to increase from mild to severe stroke. Working ability was rated most affected, being very severely impaired in all subgroups.
Table II. World Health Organization (WHO) Minimal Generic Set scores in mild, moderate, and severe stroke according to the 24-h National Institutes of Health Stroke Scale (NIHSS) assessed by a neurologist
When functioning was rated by patients and their significant others (WHODAS 2.0, Table III), the total disability score (median) showed severe impairment in all severity groups. Between-group differences, with increasing impairment from mild to severe stroke, were found in all other items, except for concentrating. The most severely rated item was working ability, which was severely to very severely impaired in all groups; the only other items rated as severely affected were mobility and household tasks in the “severe stroke” group. Both significant others and a neurologist rated non-respondent patients as having severe difficulties in all assessed functions expect for moderate difficulties in emotions and concentrating (Tables II and III).
Table III. Functioning assessed with patient and proxy World Health Organization Disability Assessment Schedule (WHODAS 2.0) (12 items) in mild, moderate, and severe stroke according to the 24-h National Institutes of Health Stroke Scale (NIHSS)
The correlation coefficient between patient and proxy WHODAS sum scores was strong (0.62, Table IV). The correspondence between the answers of patients and their significant others was very strong to strong for mobility, self-care and household tasks, and moderate for all other functions, but weak for friendships. Significant others rated standing (wK 0.53, 95% confidence interval (95% CI) 0.43–0.62), learning (wK 0.35, 95% CI 0.25–0.46), joining in community (wK 0.41, 95% CI 0.30–0.51), concentrating (wK 0.26, 95% CI 0.15–0.37), washing (wK 0.55, 95% CI 0.47–0.64), and getting along (wK 0.25 95% CI 0.14–0.37) more impaired than did the patients themselves.
In mild, moderate, and severe stroke groups, the correlations between WHODAS patient and proxy sum scores varied between moderate and very strong, being 0.39, 0.66, and 0.55, respectively. In severe stroke, the significant others rated standing (wK=0.39, 95% CI 0.22–0.55), and working ability (wK=0.26, 95% CI 0.09–0.44) more impaired than the patients; otherwise we did not find any systematic differences in the levels of ratings by patients and proxies in different severity groups.
The Spearman’s correlation coefficients between different measures (WHODAS, the WHO Minimal Generic Set, NIHSS, FIM and mRS) were mostly strong to very strong, except for patient-rated WHODAS and NIHSS, or FIM cognitive sub-score (Table IV). The 6 WHODAS life domains’ and the 2 components´ correlations with sum scores of other measures were mostly strong (Table V). Cronbach’s alpha value for reliability of the sum scores of patient-rated WHODAS, proxy-rated WHODAS, and physician-rated WHO Minimal Generic Set were 0.88, 0.93 and 0.85, respectively.
Table IV. Spearman’s correlation coefficients of sum scores of the measures used (n = 195, only in World Health Organization Disability Assessment Schedule (WHODAS) patient n = 167)
Table V. Spearman correlation coefficients between patient (n = 167) and proxy (n = 195) World Health Organization Disability Assessment Schedule (WHODAS) domains and components and sum scores of the other measures used
This study compared the shortest generic ICF-based measures of functioning (the 12-item WHODAS 2.0 and the WHO Minimal Generic Set of domains of functioning and health) with traditionally used measures of dependence and severity of stroke. The results support the utility of both generic measures in subacute stroke rehabilitants. The degree of impairment was found to increase from mild to severe stroke. Both short measures were strongly associated with conventional measures of stroke severity and dependence. Patient and proxy WHODAS ratings also mostly correlated well with each other, better in activities such as mobility, household tasks and self-care than in participation, relationships and cognition. In severe stroke, working ability was rated more impaired according to significant others and a physician than according to patients themselves.
The relationship between the stroke severity scale NIHSS and different dependence measures has been poorly understood (11). The results of the current study, which show a strong inverse relationship between NIHSS and FIM scores, are in line with a recent study of patients with acute stroke (8). In previous stroke trials, NIHSS score has also been associated with scores of dependence measures, such as BI and mRS, as well as the Glasgow Outcome Scale at 90 days (11, 32). In the same way, the current study found clear correlations between different outcome measures in subacute phase of stroke. In addition to cross-sectional correlations, a clear relationship was found between acute phase NIHSS and other outcome measures 2–3 months later: dependence measures FIM and mRS, but also the functioning measures WHODAS and the WHO Minimal Generic Set ratings. These results suggest that using the shortest form of WHODAS is in agreement with other outcome measures. The slight differences across used scales in the current study reflect the differing emphasis on various outcome components (i.e. stroke severity, dependence or functioning including physical, cognitive and emotional difficulties, activity limitations and restrictions in participation) of the instruments used. In addition, the conventional instruments do not measure the way (quality) performance in activities of daily living is accomplished. All these scales may also be partly influenced by the new phase of life for the patients and their significant others, with the consequences of the cerebrovascular accident and recent big changes, loss and recovery of functioning. In this phase of rehabilitation before discharge, the patients had made home visits (minimum 1 weekend) with the aid of their significant others, but they had not yet fully resumed their usual roles and activities, while residing mostly in hospital since stroke onset (5). However, a clear relationship between initial physician-rated disability and self-rated functioning at discharge from subacute inpatient rehabilitation was found. The results are also in line with previous findings, that many patients even with mild strokes have significant disability at discharge from rehabilitation or 3 months post-stroke (33–35).
Previous studies of WHODAS 2.0 in stroke patients have usually been based on a longer version of this scale (36). The aim of the current study was to identify as simple validated functioning scales as possible, and the 12-item WHODAS 2.0 was found suitable, especially as, in previous studies among patients with amyotrophic lateral sclerosis, traumatic brain injury, spinal cord injury and spinal pain (20–24), this measure was easy to apply for both patients and significant others. As WHODAS includes not only activities, but also items of participation, it provides a wider perspective for goal-setting and service-planning than the conventional instruments. As a self-report instrument it enhances individual patient- and family-centred procedures in rehabilitation processes. The WHO Minimal Generic Set is very brief, but it captures 7 items in body functions, activities and participation. As these 2 ICF-based tools are short and concise, the burden to the respondents is minimized. Also, other ICF-based disease-specific functioning tools can be used in stroke patients, but other measures are usually more time-consuming (ICF checklist, ICF Comprehensive and Brief Core Sets for Stroke). In the current study, the 12-item WHODAS had a strong inverse relationship with the dependence measure FIM in the same way as in a previous stroke study comparing ICF Brief Core Set for stroke with FIM scores (37). In previous studies with different diagnostic patient populations a similar positive correlation has been found between WHODAS 2.0 and other measures of dependence (19).
Interestingly, in the current study, even if relationships between WHODAS ratings and other generic measures were strong to very strong, they were even stronger in proxy ratings compared with patient ratings. This result is also in line with a previous study of subacute stroke survivors (38). Significant others rated many activity items more impaired than did the patients. As stroke survivors in intensive rehabilitation are constantly encouraged to perform in activities of daily living, they may think more of the capabilities they still have left and perhaps the tasks they still can perform with assistance than the activities they have lost. Proxies, on the other hand, may think more of the capabilities lost, the changed role, the dependence and need for help of the patient at the time of discharge. In addition, patients with more severe stroke may lack insight into the situation at this early stage, especially in more complex items, such as work. Also, cognitive and emotional functions and, especially, relationships may be more difficult and subjective items to rate before discharge. Clearly, absolute comparisons between assessments by patients and proxies are not possible, as appropriate weight cannot be given to how a person will perceive his or her own, or someone else’s, severity. However, as the correlations between the patient and proxy WHODAS scores on the whole, and also in single items were mostly moderate to very strong, it seems possible, that, when assessing functioning 2–3 months post-stroke, most of the patients are able to make assessments reliably. The results of this study are in line with a previous study of subacute stroke survivors with moderate-to-strong correlations between patient and proxy ratings in many functional items (38).
Although a physician who rated functioning using the WHO Minimal Generic Set and dependence with mRS was not blinded to background information, his or her ratings sounded reasonable and could be even more reliable through his or her insight into the clinical history of the participants. Physician-rated functioning, on the whole and in single items, correlated well with stroke severity. The fact that working ability was rated more impaired by a physician than by patients themselves is interesting. Only one-third of the patients were employed at the time of the stroke, and at the time of discharge all rehabilitants were on sick-leave trying to readjust to community life, which could influence the physician’s ratings. Many patients, as retirees, may have a more subjective view of their employment capabilities and the functioning ability they still have in diverse voluntary and domestic work possibilities, whereas a physician may think more of the requirements in the open labour market reflected by the activity restrictions and participation limitations the patients may have.
This study has some limitations. The cross-sectional study design does not allow confirmation of causal relationships of disability, i.e. whether they are based on the brain lesion itself or on its secondary consequences. The patient population in tertiary clinic intensive inpatient rehabilitation is always selected and is limited in number, but we find the sample size adequate for the purposes of the study. As different generic functioning scales were used, direct comparisons were not possible for all sub-items. Even if WHODAS is often used in chronic health conditions, it also appeared suitable in the subacute phase, as in our rehabilitant population. The patients with most severely impaired cognitive abilities, including aphasia, could not themselves respond to self-rating WHODAS. Usually these patients are omitted from studies on perceived functioning, but as we found it important also to obtain information about patients with very severe stroke, the assessments from their significant others were included.
In conclusion, both generic ICF-based functioning measures (the 12-item WHODAS 2.0 and the WHO Minimal Generic Set), despite their brevity, were useful in determining disabilities of subacute stroke patients for patient- and family-centred goal-setting and service-planning. These measures correlated well with each other and with other measures of dependence and severity of stroke. At discharge from subacute stroke rehabilitation, we recommend using the 12-item WHODAS 2.0. In the light of these results, assessment is easy, both for proxies and, with the exception of the most severe stroke, for patients themselves.
The authors have no conflicts of interest to declare


 Click to show fullsize
Click to show fullsize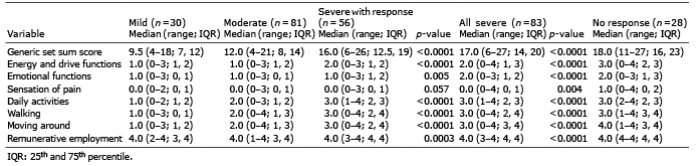 Click to show fullsize
Click to show fullsize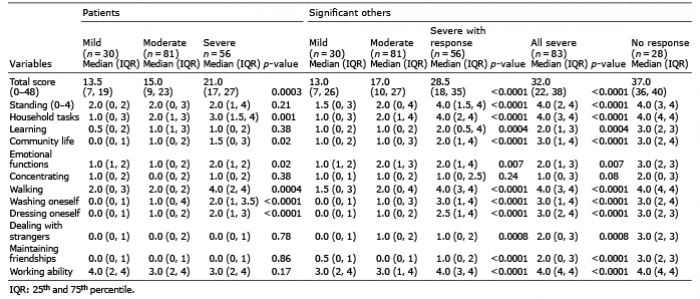 Click to show fullsize
Click to show fullsize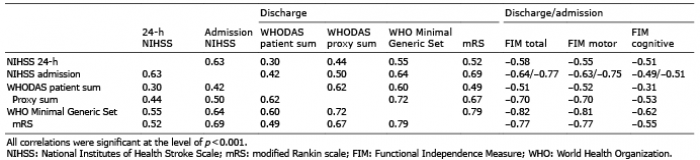 Click to show fullsize
Click to show fullsize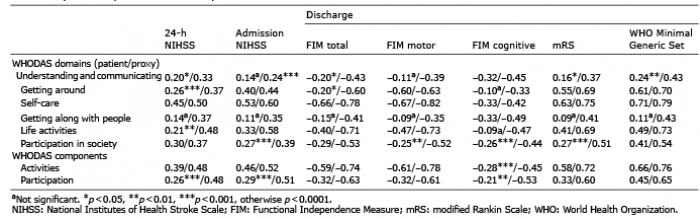 Click to show fullsize
Click to show fullsize