
From the 1Department of Biomedical and Neuromotor Science, Physical and Rehabilitation Medicine Unit, IRCCS Rizzoli Orthopaedic Institute, Lanciano, Italy, 2Department of Physical Medicine and Rehabilitation, Physical Medicine and Rehabilitation Hospital, Kuwait and 3Hacettepe University Medical School, Department of Physical and Rehabilitation Medicine, Ankara, Turkey
E-mail: vincenzo.ricci58@gmail.com
Accepted Jun 19, 2019; Epub ahead of print Jun 28, 2019
Ultrasound (US) imaging has consolidated its place among the other routine evaluation/imaging methods used by physiatrists in daily clinical practice (1, 2). There is an ever-increasing need for its prompt technical application and interpretation (3, 4). The aim of this letter is to clarify a particular issue as regards the orientation between probe positioning and the corresponding images on the US screen. Independent of the probe type (linear, convex, hockey-stick) selected for imaging various structures/pathologies at different depths or with different surface properties, getting well-oriented is not as easy as might initially be thought. In addition, questions often arise, such as “which plane is the probe in?” or “’which plane of the patient am I looking at?”, etc. Worse would be the scenario whereby the sonographer is unware of these issues or does not care, but instead has a fixed image memory for different structures. This might pose significant additional challenges, especially if an intervention is planned (5, 6).
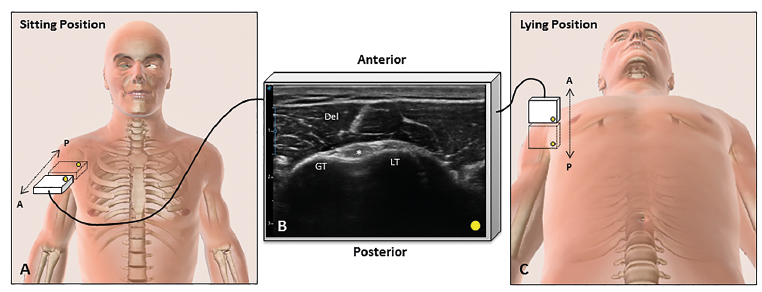
“Getting lost” in the US screen while the long injector/needle is inside an anxious patient would indisputably be terrifying. At this point, 3 noteworthy hints for “dummies” would be: (i) the US screen always corresponds to the coronal plane in the universe; (ii) US imaging is a sort of “tomographic examination” that permits the sonographer to “cut the body into slices” with a possibility of infinite planes; and (iii) the deeper you see on the screen refers to what resides “away” from the footprint of your probe (in the patient’s body). In order to clarify this discussion, we present here 2 common/exemplary imaging scenarios; shoulder (Fig. 1) and knee (Fig. 2). The knee imaging is easier to interpret because the plane of the probe and the US screen are parallel to each other; in this sense “spatial planning” of the interventional procedure (e.g. where can I enter with the needle?, where should the needle be directed?) is simpler and more intuitive (Fig. 2). Thus, static and dynamic imaging can readily be followed on the screen as long as the sonographer is knowledgeable about the local anatomy and the corresponding appearance (7). However, in the shoulder imaging, the planes of the probe and the US screen are perpendicular to each other (Fig. 1A, B), while scanning the long head of the biceps tendon in the (commonly applied) sitting position (8). Only if imaging is performed in a lying position do the 2 planes become parallel (Fig. 1B, C) and the scanning becomes more straightforward as regards ease of interpretation. To conclude, in light of the aforementioned tips, sonographers should be aware of the need for optimal orientation for better interpretation of daily scans/procedures.
Fig. 1. Anterior short-axis ultrasound imaging for the shoulder. While the patient is in a sitting position, the probe is naturally positioned in the transverse plane (A), whereas the image on the screen is in the coronal plane (B). While the patient is in a lying position (C), the 2 aforementioned planes are aligned parallel in universe. Del: deltoid muscle; GT: greater tuberosity; LT: lesser tuberosity; asterisk: long head of the biceps tendon.
Fig. 2. Anterior long-axis ultrasound imaging for the knee. As the patient is in sitting/lying position, the probe and the US screen are aligned in the same plane. Pa: patella; F: femur; PFP: prefemoral fat pad; SFP: suprapatellar fat pad; asterisk: suprapatellar bursa/recess; white arrowheads: quadriceps tendon.


 Click to show fullsize
Click to show fullsize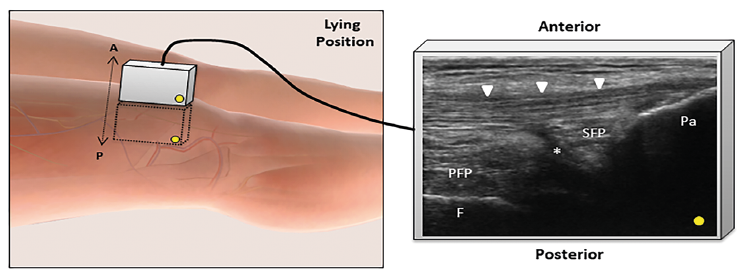 Click to show fullsize
Click to show fullsize