
From the 1St Vincent’s Hospital, Sydney, 2St Vincent’s Clinical School, 3South Western Sydney Clinical School, University of New South Wales, Wales, 4Whitlam Orthopaedic Research Centre, Ingham Institute for Applied Medical Research, Sydney and 5School of Public Health and Community Medicine, University of New South, Wales, Australia
Objectives: To assess the feasibility of in-reach rehabilitation for critical care survivors following discharge from the intensive care unit. To determine whether additional in-reach rehabilitation reduces hospital length-of-stay and improves outcomes in critical care survivors, compared with usual
therapy.
Participants: A total of 66 consecutively-admitted critical care survivors with an intensive care unit stay ≥ 5 days were enrolled in the study. Of these, 62 were included in the analyses.
Methods: Pilot randomized control trial with blinded assessment at 6 and 12 months. The intervention group (n = 29) received in-reach rehabilitation in addition to usual ward therapy. The usual-care group (n = 33) received usual ward therapy. The primary outcome assessed was length-of-stay. Secondary outcomes included mobility, functional independence, psychological status and quality-of-life.
Results: The intervention group received more physiotherapy and occupational therapy sessions per week than the usual-care group (median = 8.2 vs 4.9, p < 0.001). Total length-of-stay was variable; while median values differed between the intervention and usual care groups (median 31 vs 41 days), this was not significant and the pilot study was not adequately powered (p = 0.57). No significant differences were observed in the secondary outcomes at hospital discharge, 6- or 12-month follow-ups.
Conclusion: Provision of intensive early rehabilitation to intensive care unit survivors on the acute ward is feasible. A further trial is needed to draw conclusions on how this intervention affects length-of-stay and functional outcomes.
Key words: critical illness; rehabilitation; critical care; treatment outcome; rehabilitation research; outcomes research
Accepted Jun 14, 2019; Epub ahead of print Jul 8, 2019
J Rehabil Med 2019; 51: 00–00
Correspondence address: Jane Wu, St Vincent’s Hospital, Sydney, New South Wales, Australia. E-mail: jane.wu@svha.org.au
This pilot study aimed to assess whether early, structured rehabilitation can be provided to critical care survivors and aid physical and psychological recovery. The study recruited 66 participants who were critically ill and were in intensive care for at least 5 days. The study compared patients receiving early rehabilitation in addition to usual therapy, vs usual therapy on the acute ward. Both participant groups were assessed at hospital discharge and at 6 and 12 months. The outcomes assessed included: length of hospital stay; mobility ability to carry out activities of daily living; psychological symptoms; and quality of life. The results showed that early rehabilitation was feasible, could be provided to critical care survivors, and suggested that these patients may have a shorter length of stay in hospital. While both groups improved in their other outcomes, there were no major differences between the groups.
Critical care survivors experience long-term physical and functional impairments, neurocognitive deficits, impaired mental health, decreased quality of life, and decreased rates of return to work (1). Existing guidelines for the rehabilitation management of critical care survivors, such as those developed in the UK (2), encourage the commencement of rehabilitation “as soon as possible” and “as much as possible”.
Of the research published to date investigating early rehabilitation of critical care survivors, interventions are primarily delivered within the intensive care setting. This includes a recent trial that found that a combined physiotherapy and occupational therapy programme delivered in the intensive care unit (ICU) resulted in improved functional outcomes at hospital discharge and a shorter duration of delirium (3). Furthermore, the effectiveness of early mobilization of patients in the ICU has been examined in several systematic reviews (4–7) and a meta-analysis (8), where it was also found to improve physical function and reduce the duration of mechanical ventilation. In keeping with Australian guidelines (9), early mobilization in the ICU has been adopted as part of standard care in some hospitals.
In Australia, early co-ordinated rehabilitation is routinely provided in the following hospital settings: stroke units (10), orthogeriatric services (11) and aged care services (12). For patients not receiving care in one of these settings, early rehabilitation would typically commence only after a referral was made by the acute medical or surgical treating team to rehabilitation services. Early rehabilitation for such patients is often now provided by an in-reach rehabilitation team. This model of care has emerged over the last decade and has been adopted by a number of Australian hospitals since 2010 (13). In-reach rehabilitation teams are mobile (treating patients on different wards), multidisciplinary (involving at least 3 disciplines), coordinated, and are staffed to provide an intensity of therapy that is comparable to the rehabilitation setting (at least 2 therapy sessions per day).
At the time this pilot study was conceived, there were no randomized controlled trials to guide the provision of early rehabilitation for critical care survivors on an acute ward after discharge from ICU (14). This study therefore aimed to explore the feasibility, efficiency and effectiveness of a coordinated inpatient early rehabilitation programme, delivered by an in-reach rehabilitation team as early as possible to critical care survivors on the acute ward.
Objectives
The trial was granted ethical approval by the Human Research Ethics Committee of St Vincent’s Hospital Sydney (HREC/12/SVH/324), and was retrospectively registered with the Australian New Zealand Clinical Trials Registry (Trial Id: ACTRN12618000539235). The trial is reported according to the Consolidated Standards of Reporting Trials (CONSORT) guidelines.
Design
A single-site, prospective pilot randomized controlled trial was conducted with blinded outcome assessment at 6 and 12 months.
Participants
Participants were recruited from the ICU of one metropolitan hospital in Sydney, Australia. The hospital is a tertiary referral and heart and lung transplant centre. The ICU is a 15-bed unit that cares for approximately 1,100 patients per year. Critical care survivors were included in the trial if they met the following inclusion criteria: aged 18–75 years; ICU stay ≥ 5 days; predicted LOS on the acute ward ≥ 5 days; and premorbid functional independence, defined a priori as a Barthel Index score ≥ 70, obtained from a proxy describing patient function during the 2 weeks prior to admission. Patients were excluded if they were not expected to survive their admission (e.g. withdrawal of life support and considered for palliation); were unable to be followed-up (e.g. overseas visitor, homeless, severe hearing impairment); were unable to speak English; had a pre-existing diagnosis of dementia (of any aetiology); severe psychiatric disorders with recent hospitalization (within 6 months) or an active substance use disorder.
Recruitment and allocation
Participants were recruited within 72 hours of transfer from ICU to an acute ward. After baseline assessment, participants were randomly allocated to 1 of 2 groups, either the early rehabilitation intervention group, or usual care. A web-based, computer-generated randomization procedure (accessed from: http://www.graphpad.com/quickcalcs/randomize1.cfm 12/11/2012) was used for random sequence generation. Group allocation was placed in sealed envelopes, prepared by an administrative staff member with no role in clinical care or the study procedures, and numbered sequentially.
Intervention
The intervention group received involvement of an in-reach mobile rehabilitation team. This multidisciplinary team consisted of a rehabilitation physician (0.2 full-time equivalent), nurse (0.2 full-time equivalent), full-time physiotherapist and full-time occupational therapist. The mobile rehabilitation team had a caseload of 6–8 patients at any one time. This team was available 5 days per week and commenced rehabilitation immediately after baseline assessment, as soon as possible after ICU discharge to the acute ward.
Participants in the intervention group were all visited by the rehabilitation physician for an initial assessment. Subsequent visits by the physician were based on clinical need, typically once or twice per week. A structured multidisciplinary rehabilitation programme was devised for each patient. This aimed to address individual patient needs, involved the patient in decision-making and goal-setting, and was reviewed regularly during the patient journey via twice weekly multidisciplinary team meetings. The in-reach therapists worked with ward therapists so that the therapy frequency delivered was over and above what the patient would normally receive from acute ward therapists. The expected frequency was a 2-fold increase in therapy sessions for the intervention group compared with usual care.
The duration of the study intervention was also determined by clinical need, i.e. patients could be discharged from the service once all rehabilitation goals during the acute stay were achieved. For those patients who required inpatient rehabilitation, the in-reach team remained involved until acute hospital discharge and transfer to rehabilitation.
Control
The control group received usual care, as directed by the acute physicians or surgeons on the acute ward. This involved acute ward allied health and nursing interventions, which were not coordinated by a rehabilitation physician or nurse. Each therapy discipline prioritized their interventions based on resources, clinical need and patient flow pressures, without reference to other team members. However, the in-reach rehabilitation team is well established at the hospital, and referrals based on clinical grounds by the acute medical/surgical teams can be considered part of usual care. The treating team always had the option of referring patients for additional therapy via the in-reach rehabilitation team at any time-point during the acute ward stay, if they perceived a clinical need.
Both intervention and control groups had the same access to weekend physiotherapy as part of usual care, which prioritizes patients discharging home. No routine occupational therapy was available to any participants on the acute ward over weekends. Participants were not blinded to group allocation.
Outcome measures
A baseline assessment was completed with all participants by a blinded assessor within 72 hours of transfer from the ICU. Baseline measures included: premorbid Lawton’s Instrumental Activities of Daily Living Scale (15); the Functional Independence Measure (FIM) (16); the Confusion Assessment Method for the ICU (CAM-ICU) to assess for the presence/absence of delirium (17); and the Medical Research Council (MRC) muscle scale (18) to assess for the presence/absence of ICU-acquired weakness (defined as MRC sum score < 48 (19)). Additional data were extracted from participants’ medical records, including principal diagnosis of admission, the Charlson Comorbidity Index (20) (a global measure of illness severity), and duration of delirium (based on daily CAM-ICU assessment (17)).
LOS was collected from the medical records. ICU LOS refers to the first admission to ICU (if there was more than one admission to ICU). Acute LOS refers to all acute care days (including ICU readmission(s)) before acute discharge or transfer to inpatient rehabilitation. Total LOS refers to all admitted bed days including transfers back to acute care from rehabilitation and subsequent acute care days if they were transferred to another hospital.
In order to monitor fidelity and describe the rehabilitation treatments received by each participant, therapy dosage was collected from each participant’s medical record and quantified as the number of therapy occasions of service undertaken by discipline.
During their acute ward admission, the physical activity of each participant was quantified using a physical activity monitor, the activPAL™ (AP; Physical Activity Technologies, Glasgow, UK), worn on the thigh. This device has been validated and shown to accurately differentiate between time spent sitting/lying, standing and stepping, even in sedentary populations (21). Research staff applied the activity monitors to participants and collected activity data for a 24-hour period once per week on a weekday, over the course of their acute hospital admission.
All participants were assessed on the ward by an unblinded assessor at the time of discharge from the acute hospital (regardless of whether they were discharged home or transferred to inpatient rehabilitation). Discharge assessments included the FIM; ICU-acquired weakness (via MRC sum score); Timed Up and Go Test (22) and 6-minutes walk test (23) for physical function; and the Depression Anxiety Stress Scale 21 (24) (DASS-21) for psychological status. Discharge destination and LOS were also collected.
Longer term outcomes were measured at 6 and 12 months. Assessments were conducted via phone by a blinded assessor, and included: the DASS-21; Lawton’s Instrumental Activities of Daily Living Scale (15); and 2 quality of life scales, the Short Form-12 (SF-12 v2) (25) and the Assessment of Quality of Life (AQoL-4D) (26) questionnaire. The principal study investigator (JW) provided staff training, a written assessment protocol, standard equipment and regular monitoring to ensure measurement accuracy and consistency between assessors.
Data analyses
The primary outcome for this trial was total hospital LOS (days), including days in the acute hospital admission, and any inpatient rehabilitation (where it was required). Secondary outcomes included: change between baseline and discharge FIM; ICU-acquired weakness, discharge Timed-Up and Go; discharge 6-minute walk; discharge DASS-21; and discharge destination. Analyses of follow-up data at 6 and 12 months were used to supplement those at the primary endpoint of hospital discharge. Process measures quantifying therapy delivery, intensity and physical activity were used to enable accurate description of the intervention that was delivered to each group.
Groups were compared at hospital discharge and at follow-up using Mann–Whitney U tests for non-normally distributed variables, and χ2 analyses for categorical variables. Analyses of outcome data were by intention-to-treat. Longitudinal changes in continuous data (e.g. FIM, DASS-21) were analysed using repeated measures analyses of variance (ANOVAs), with factors of time and group. Analyses were performed using SPSS v21 (IBM Corp., Armonk, NY, USA), and results were considered significant where p < 0.05.
Given that this was a feasibility pilot study, no formal power calculation was performed for this trial. Rather, the aim was to recruit all eligible participants over a 12-month period in order to generate the preliminary data required to perform formal power analyses for a subsequent larger trial. Power calculations were performed using our pilot data to model sample size requirements for a future randomized controlled trial of in-reach rehabilitation using LOS as a primary outcome. Calculations were performed in GPower (accessed via http: //www.gpower.hhu.de/), using a non-parametric 2-sample t-test model, with a power of 80% and a significance threshold of α < 0.05.
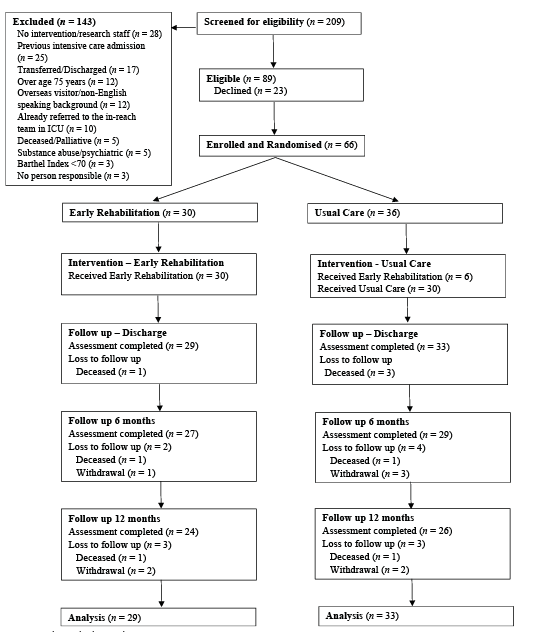
Flow of participants through the trial
Between May 2015 and August 2016, a total of 209 ICU survivors with a LOS of at least 5 days were screened (Fig. 1). Of the 89 patients who were eligible for the study, 66 (74.2%) consented to participate. Four patients subsequently died in acute care, and were not included in the analyses. Follow-up assessments were completed for all participants by October 2017.
Fig. 1. Flow of participants through the trial.
Baseline characteristics
The study cohort was comprised 43 males and 23 females, mean age 55 (standard deviation (SD) 13) years. Baseline comparisons between the intervention and control groups are presented in Table I. There were no significant between-group differences for any demographic or clinical variables at baseline. Prior to enrolment, the pooled cohort spent a mean of 9.7 (SD 5.0) days in ICU.
Table I. Comparison of baseline characteristics
Dose of therapy and activity levels
The mean number of days from ICU discharge to commencement of the in-reach rehabilitation team was 2.0 (SD 1.4) days. The in-reach team was involved in patient care for a mean of 11.3 (SD 8.7) days. Participants receiving in-reach rehabilitation stayed a mean of 17.8 (SD = 14.9) days on an acute ward. One patient in the intervention group did not receive the in-reach rehabilitation intervention, as they were transferred back to the referring rural hospital within 2 days of recruitment, before the intervention could be commenced. Six out of the 33 patients in the control group received early rehabilitation from the in-reach team, as their primary care teams made a referral as part of usual care and standard hospital practice.
The therapy dosage received in both groups and activPAL data are described in Table II. The intervention group received a median of 8.2 (IQR 6.0–11.8) occasions of service from physiotherapy and occupational therapy per week. This was significantly higher (p = 0.001) than the usual care group, who received 4.9 (IQR 2.6–7.0) occasions of service per week. The activPAL data demonstrated low levels of physical activity across both groups, whereby participants achieved approximately 500 steps in a 24-hour period, with no significant between-group differences.
Table II. Comparison of therapy dose provided and participant activity levels
Length of stay
Intention-to-treat analyses were conducted for LOS and are presented in Table III. No significant between-group differences were observed for LOS measures, except for rehabilitation LOS. The rehabilitation LOS was, however, based on low numbers (as only 9 patients in the intervention group and 10 in the control group went to inpatient rehabilitation). Median values for total LOS appeared to differ between groups, (31 days [IQR 20–56] for the early rehabilitation group vs 41 days [IQR 17–54] for the control group), but this was not significant in the present pilot.
Table III. Comparison of length of stay
Secondary outcomes
Analyses of secondary outcomes are shown in Tables IV and V. Participants in both groups demonstrated improved function (measured by the FIM score) from ICU discharge to acute care discharge, but there were no differences in the magnitude or rate of improvement between the groups. Participants’ ability to attend to domestic activities of daily living (as measured by the Lawton’s Scale) improved from baseline to 6-month follow-up, and remained stable until 12 months. Both participant groups demonstrated lower quality-of-life scores and higher scores on the DASS compared with population norms (25, 27) at follow-up. As for the primary outcomes, no significant between-group differences were observed for any secondary measures.
Table IV. Comparison of secondary outcomes
Table V. Comparison of other secondary outcomes
Sample size determination
Using LOS as the primary outcome and the observed variability in our pilot data, a future adequately powered trial (with 80% power) would require 943 participants in each group to detect a 10% relative reduction in total LOS; or 604 participants in each group to detect a 10% relative reduction in acute LOS.
This pilot randomized controlled trial demonstrated that it is feasible to provide an intensive coordinated multidisciplinary rehabilitation programme using an in-reach team for ICU survivors on the acute ward. To our knowledge, this is the first trial to explore the delivery of a multidisciplinary rehabilitation intervention in this patient population, combining medical, nursing, physiotherapy and occupational therapy expertise.
Significant improvements in physical function over the course of admission were observed for patients receiving both in-reach rehabilitation, and usual care. There was a non-significant difference in total LOS between the intervention and control groups (median difference 10 days), but given this pilot was not powered to detect significant differences in LOS, the reported p-values should be interpreted with caution.
Since the time of conception of this pilot study, there have been 3 other trials of early rehabilitation programmes in this patient population, each exploring a different intervention, but focused mainly on physiotherapy. Gruther and colleagues (28) showed, in a randomized controlled trial (n = 53), that an early rehabilitation programme using additional physiotherapy on the acute ward for intensive care survivors led to earlier discharge from hospital. This study found a median 7-day reduction in hospital LOS, although long-term follow-up outcomes were not assessed. Their cohort had a much longer LOS in ICU (mean = 20 days) compared with our cohort (mean = 10 days). They also used a number of criteria to select patients who were more likely to benefit from an early rehabilitation programme. Gruther et al.’s trial (28) was able to deliver a mean of 114 ± 58 min/day of therapy in the intervention group compared with 21 ± 46 min/day of therapy in the standard-care group, representing a 543% increase in therapy dose. Our study achieved less than a 2-fold increase in combined physiotherapy and occupational therapy compared with standard care, which probably contributed to our divergent results.
The study by Walsh et al. (29), conducted at 2 hospitals in Scotland, was more similar in methodology and outcomes to the present study. Their participant cohort closely resembled that of the present study (median time in ICU 11 days), as did the intervention timing and intensity, starting 2 days post ICU-discharge and offering a similar increase in therapy intensity with an allied health assistant seeing patients once daily. Walsh et al. (29) reported that using an allied health assistant to deliver a 2- to 3-fold increase in therapy in the intervention group did not confer a benefit for LOS in their randomized controlled trial. This is congruent with our findings, and suggests that a greater increase in therapy intensity (over and above a 2–3-fold increase) may be needed to achieve significant benefits.
In a trial by Denehy et al. (30), the investigators aimed to provide 2 additional sessions of physiotherapy per day, but were unable to show an effect over usual care on LOS, physical function and quality of life. In this Australian trial, the dose of therapy provided was not measured, and limited information was available regarding what therapy was delivered to the intervention group compared with the usual care group. An insufficient dose of therapy may again be a possible explanation for the negative results of this trial.
The current study has shown that it is feasible to provide a higher level of rehabilitation in the acute care setting compared with standard ward practice, and to achieve patient participation even among patients who remain medically unwell. However, process measures revealed that the dose of therapy actually delivered as part of our experimental intervention was less than intended. A median of 8.2 therapy sessions per week in the intervention group, compared with 4.9 therapy sessions for the control group, meant that the 2-fold increase target was not achieved with our staffing levels. Therapy dosage was also demonstrated to be a problem in a similar, but adequately powered, early rehabilitation trial in multi-trauma patients (31). These results, together with those of similar trials (28–30), emphasize that therapy dose is an important consideration that needs to be further characterized in the early/acute rehabilitation setting. They also highlight the importance of monitoring intervention fidelity and evaluating the real-world dose of therapy delivered in rehabilitation trials, in order to draw valid and meaningful conclusions about the dose of therapy required to improve outcomes (32).
Rehabilitation standards can vary between hospitals. Our hospital provides physiotherapy up to 7 days per week as standard care. Many published rehabilitation trials have been conducted in different “usual care” settings, often with lower levels of usual care rehabilitation (33) (e.g. a median of 2.6 physiotherapy sessions per week was reported as standard care in a hospital in Scotland (34)). Furthermore, in the present study 52% of patients in both arms were discharged home to their usual place of residence upon leaving hospital. This compares with 24% of usual-care patients and 43% of intervention patients in the study by Schweickert et al. (3). These differences in usual care practice, including the provision of relatively intensive usual care rehabilitation services at our study site, may have contributed in part to the lack of significant between-group differences observed.
Patient selection is another important consideration for future rehabilitation trials that was not explicitly addressed in the present study. Gruther et al. (28) utilized a rehabilitation physician (physiatrist) to clinically assess patients in order to identify those most likely to benefit from their intervention and subsequently report the only positive findings published to date. Thus, developing a screening process to enable identification of those patients most likely to benefit from a targeted early rehabilitation programme is worthy of further investigation. This may improve patient selection to maximize the benefit from resource- and time-intensive rehabilitation interventions.
The use of an activity monitor highlighted an overall lack of physical activity on hospital wards. This is consistent with other research using activity monitors, which have found similarly low levels of activity in hospitalized patients (35–37). Evidence is emerging to suggest that hospitalized physical activity has effects on readmission rates (38) and mortality (39). This finding has important implications for both clinical practice and researchers to explore innovative strategies to increase physical activity during the acute hospital stay.
Experience gained from conducting this trial and another similar early rehabilitation trial in multi-trauma (31) calls into question the use of LOS as the primary outcome measure for assessing the efficiency and effectiveness of early rehabilitation. LOS can be significantly influenced by medical complications, which may be unrelated to mobility, functional independence, as well as numerous non-clinical factors (40). Our forecasted sample size calculations using LOS as a primary outcome measure indicate that very large numbers of participants would be required in future trials, which would make them costly and logistically complex. Alternative outcome measures may need to be considered, such as the time taken for participants to achieve functional milestones or discharge readiness from a functional perspective.
Strengths of this study include its high follow-up rate, comprehensive measurement protocol, including the collection of long-term longitudinal follow-up data, and the use of a consecutive cohort of patients. The findings of this pilot study can be used to inform the design of larger definitive trials in this area. We have learnt from this pilot study that it is important to collect data directly quantifying therapy dose; have a method of selecting patients most likely to benefit from early rehabilitation; and use a randomization scheme that stratifies for age, diagnostic categories and functional disability to avoid the influence of cofactors on the LOS. In-reach teams may need to reconsider their model of care and staffing ratios so that adequate levels of therapy intensity can be provided. It may be pertinent for trials to mandate a minimum level of intensity in order for an intervention to be classified as an early rehabilitation intervention.
Limitations of this study include its small sample size, pilot nature and intervention infidelity. Because of the considerable variability in LOS, our prospective power calculations have shown that large numbers of patients would be required to replicate a powered trial using the same methodology. “Contamination” was a significant problem in the present study, which led to 6 patients allocated to the control arm receiving early in-reach rehabilitation. It was considered unethical not to provide additional rehabilitation services to patients. Their acute teams were blinded to the randomization in the study, and, therefore, if their acute team made a referral for in-reach rehabilitation based on clinical need, then that referral was considered part of usual treatment. These events, however, confound the interpretation of our results. Future studies may need to be conducted in hospital sites that do not offer in-reach rehabilitation as part of standard clinical care. Alternatively, a cluster randomized trial design may be used to circumvent this issue in future trials, but this may not reduce total sample size, given that cluster trials appear to be more efficient only where contamination exceeds 30% (41).
In conclusion, this study found that it is feasible to deliver a coordinated, multidisciplinary rehabilitation programme, using an in-reach rehabilitation team, to critical care survivors soon after discharge from the ICU. Significantly more sessions of physiotherapy and occupational therapy were delivered via the intervention, compared with usual care. Median values for total LOS were 31 [20–56] days for the intervention group and 41 [17–54] days for those receiving usual care. Although this did not represent a significant reduction in this pilot study, a larger definitive trial, which can deliver more than a 2-fold increase in therapy dose compared with usual care, may be worth exploring. Intervention dose, fidelity, outcome measurement and patient selection should be key considerations in the design of future trials.


 Click to show fullsize
Click to show fullsize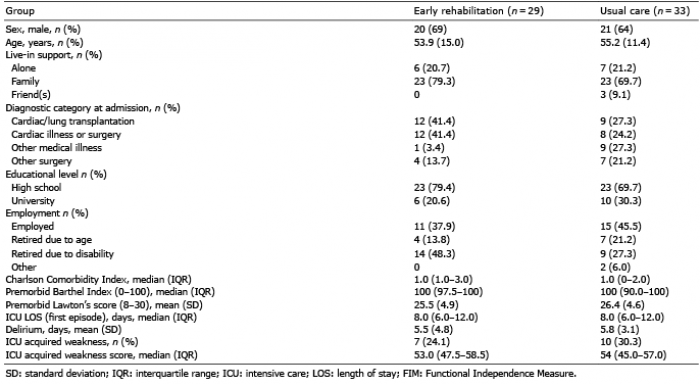 Click to show fullsize
Click to show fullsize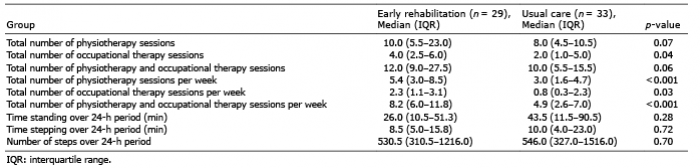 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize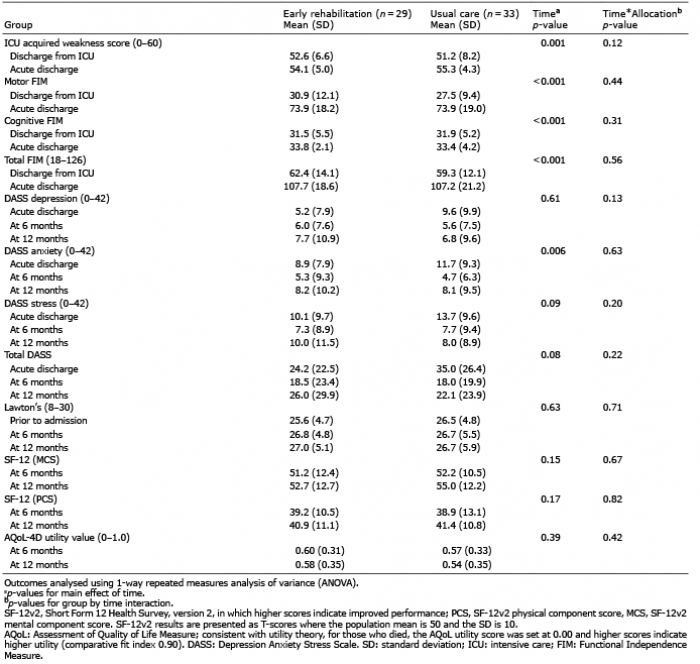 Click to show fullsize
Click to show fullsize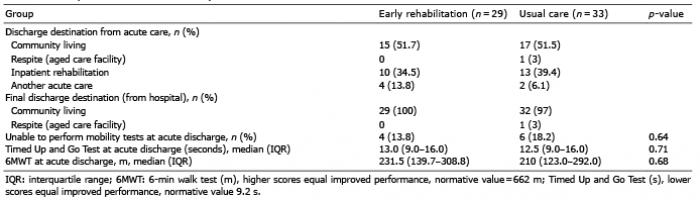 Click to show fullsize
Click to show fullsize