
From the 1Department of Respiratory Rehabilitation Center, Beijing Rehabilitation Hospital of Capital Medical University, Beijing, China, 2Department of Anaesthesiology and Intensive Care Medicine, University Medical Centre of Schleswig-Holstein Campus Kiel, Germany, 3Department of Biomedical Engineering, Fourth Military Medical University, Xi’an, China and 4Institute of Technical Medicine, Furtwangen University, Villingen-Schwenningen, Germany
#These authors contributed equally to this publication.
Objective: To investigate the effects of normocapnic hyperpnoea training on pulmonary function and patient-reported outcomes in chronic spinal cord injury.
Design: Single-centre randomized controlled trial.
Patients: Eighteen patients with spinal cord injury > 24 months post-injury and without regular respiratory muscle training prior to the study were included prospectively.
Methods: Patients were randomly assigned to either normocapnic hyperpnoea or control groups. The normocapnic hyperpnoea group patients performed training 15–20 min per day, 5 times a week for 4 weeks. The patients hyperventilated through partial re-breathing of ventilated air. The control group received no respiratory muscle training. Other rehabilitative programmes were performed identically in both groups. Lung function testing was performed in the sitting position prior to and after the study. Patient-reported outcomes were assessed using the Patient Health Questionnaire-9, St George’s Respiratory Questionnaire, Chronic Obstructive Pulmonary Disease Assessment Test and Borg scores.
Results: Significant differences were found in the improvement ratio between the normocapnic hyperpnoea and control groups for all investigated parameters, except total lung capacity and diffusing capacity of the lung for carbon monoxide.
Conclusion: Normocapnic hyperpnoea training may reduce the incidence of respiratory symptoms, improve pulmonary function and quality of life, and reduce depression in patients with chronic spinal cord injury, regardless of their neurological level of injury, even at more than 24 months after injury.
Key words: normocapnic hyperpnoea; chronic spinal cord injury; patient-reported outcomes; respiratory muscle training; lung function.
Accepted May 29, 2019; Epub ahead of print Jun 14, 2019
J Rehabil Med 2019; 51: 00–00
Correspondence address: Hongying Jiang, Department of Respiratory Rehabilitation Center, Beijing Rehabilitation Hospital of Capital Medical University, Xixiazhuang, Baduchu, Shijingshan, Beijing 100114, China. E-mail: 6jhy@163.com; and Zhanqi Zhao, Department of Biomedical Engineering, 169 Changle Xi Rd, Fourth Military Medical University, Xi’an, China. E-mail: zhanqi.zhao@hs-furtwangen.de
Respiratory muscle endurance training is beneficial for patients with chronic spinal cord injury. This study measured the effects of respiratory muscle endurance training on lung function and patient-reported outcomes. Eighteen patients with spinal cord injury who were > 24 months post-injury were randomly assigned to either a studied or a control group. The results showed that endurance training may reduce the incidence of respiratory symptoms, improve lung function and quality of life, and reduce depression in patients with chronic spinal cord injury, regardless of their neurological level of injury, even at more than 24 months after injury.
Significant impairment of lung function is frequent in patients with spinal cord injury (SCI). Respiratory complications are the leading cause of death in this population. Regular physical exercise helps to improve lung function (1). Current general rehabilitative programmes include passive range of movement, mattress exercise, sitting balance and upper limb functional training (2). Respiratory muscle training (RMT), on the other hand, focuses on training the inspiratory and/or expiratory muscles to improve muscle strength, muscle endurance and, at the same time, lung function (3). Early initiation of RMT after an SCI may have a positive effect on respiratory function and prevent respiratory complications (4). Patients may benefit from RMT even after several years of injury (5). The most widely used type of RMT facilitates flow resistive devices to add additional work on inspiration and/or expiration (3). Other types of RMT include pressure threshold, abdominal weights and glossopharyngeal breathing focussing on different breathing mechanisms. Only a few studies have evaluated the effects of RMT with normocapnic hyperpnoea (NH) in SCI (4, 6). NH may be an attractive training modality, since it trains inspiratory and expiratory muscles within a single programme. As shown by Van Houtte et al., respiratory muscles usually work at low resistance; therefore, challenging respiratory muscles by forced hyperpnoea might be a more “natural” way to train these muscles (4). Only limited data have been published on the effects of NH training in patients with chronic SCI with regard to their patient-reported outcome measures (PROMs), which is a very important aspect of patient-centred healthcare (7). Khazaeipour et al. reported a high prevalence of depression in patients with SCI (8). Postma et al. found that impaired respiratory function was associated with lower health-related quality of life (9). We hypothesize that improving lung function may also improve patients’ quality of life and reduce levels of depression.
The aim of the present study was to investigate the effects of NH training on quality of life, pulmonary function and the incidence of respiratory symptoms in patients with chronic SCI. Whether the improvements were related to the neurological level of injury was also examined.
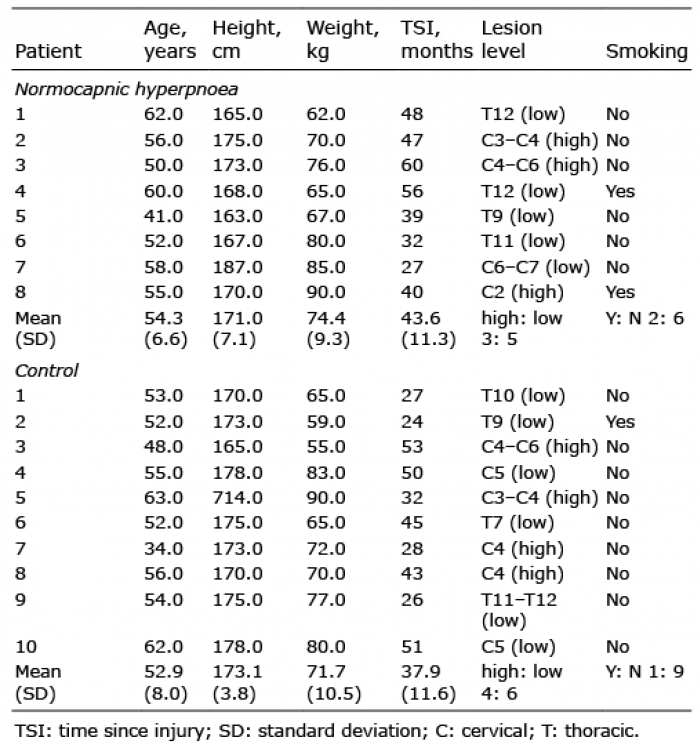
The study was approved by the ethics committee of Beijing Rehabilitation Hospital of Capital Medical University (Y20180012). In this single-centre preliminary randomized controlled trial, patient recruitment was performed in June 2018 with consecutive inpatients who met the inclusion criteria. Written informed consent was obtained from all patients prior to the study. Patients with SCI with a time post-injury > 24 months and without regular respiratory muscle training prior to study inclusion were included prospectively. Patients were randomly assigned to either NH training or control groups, using a computer-generated randomization table. Since limited data were published on the effects of NH training in patients with chronic SCI with regard to their level of depression, the sample size estimation was based on the difference in forced vital capacity (FVC) reported with a delta of 0.12 L (5). A priori power analysis determined that a sample size of 6 subjects in each group with SCI was required to obtain a statistical power of 0.80 (10). Considering possible drop out during the study, a total of 18 patients were randomized (see Table I for detailed demographics). For later data analysis, lesion level higher or equal to the fourth cervical vertebrae was considered “high” neurological level of injury. Other low cervical and thoracic SCI were referred to as “low” lesion level.
The patients in the NH group performed the RMT for 15–20 min per day, 5 times a week for 4 weeks with Spirotiger (Idiag AG, Volketswil, Switzerland). The patients hyperventilated through partial re-breathing of ventilated air (50% forced vital capacity (FVC)) and were supported by visual and acoustic feedback of breathing volume and frequency. The workload was adjusted during the training period to maintain a Borg CR-10 score (11) of 5–6/10. The control group received no RMT. Other rehabilitative programmes were performed identically in both groups (1~2 times/day, 5 days/week), such as passive range of movement (5 min/limb for all joints), mattress exercise (including trunk rolling, sit-ups, moving on bed, etc., 10 min), dynamic sitting balance (with increasing difficulty of catching ball, 5 min), or upper limb functional training (upper limb muscle power and endurance training, 20 min). The training was conducted by physiotherapists, who had a Bachelor’s degree and more than 5 years of clinical experience.
Lung function testing was performed in both groups in the sitting position prior to and after the study (MasterScreen, CareFusion, Höchberg, Germany). In addition, patients were asked to assess: the presence and severity of depressive symptoms, using the Patient Health Questionnaire-9 (PHQ-9) (12); impact on overall health, daily life, and perceived well-being, using the St George’s Respiratory Questionnaire (SGRQ) (13); the global impact on health status (due to cough, sputum, dyspnoea, chest tightness), using the Chronic Obstructive Pulmonary Disease Assessment Test (CAT) (14); and the level of perceived exertion and shortness of breath, using the Borg score.
The primary endpoint was the differences in PHQ-9 between NH and control groups. Exploratory endpoints included the lung function and PROMs differences between groups (NH and control) and between lesion levels (high and low).
Statistical analysis of the data was performed using the MATLAB 7.2 statistic toolbox (The MathWorks Inc., Natick, MA, USA). Due to the small sample size and a mix of ratio-scale and ordinal-scale variables, non-parametric statistical methods were applied. The values in each group are expressed as medians and interquartile ranges. The differences in lung function and PROMs changes between pre- and post-study within the same groups were compared using the Wilcoxon signed-rank test. Mann–Whitney U test was used to compare high and low lesion levels. A p-value < 0.05 was considered statistically significant. Bonferroni’s post-hoc test was used to modify p-values for multiple comparisons.
All training sections were conducted as planned and no adverse events were recorded. Patient demographics for NH and control groups are summarized in Table I. A summary of the determined pulmonary function parameters and the PROMs taken before the study and at the end of the 4-week study period are presented in Table II. FVC, forced expiratory volume in 1 s (FEV1), and maximal voluntary ventilation (MVV) were significantly higher in the NH group, but not in the control group at the end of the study period. All 4 PROMs revealed significant improvement in patients’ status in the post-study results for the NH group. Incidence of respiratory symptoms (e.g. sputum, shortness of breath, wheezing) were reduced compared with pre-study evaluation. There were significant differences in the improvement ratio between the NH and control groups for all investigated parameters, except total lung capacity (TLC) and diffusing capacity of the lung for carbon monoxide (DLCO). Significant differences in FVC and Borg score were found between high- and low-level lesions, both pre- and post-study (FVC in high vs low levels 53.6 ± 10.8 vs 68.6 ± 16.9 (pre, p < 0.05), 44.8 ± 17.8 vs 68.6 ± 21.3 (post, p <0.01); Borg score in high vs low levels 5.0 ± 0.8 vs 3.0 ± 1.8 (pre, p <0.01), 5.0 ± 2.0 vs 3.0 ± 1.0 (post, p <0.01)). However, the improvement ratio was not dependent on the lesion level.
Table I. Demographics of patients in the normocapnic hyperpnoea and control groups
Table II. Pre-study and post-study lung function and patient-reported outcome measures (PROM) results from the normocapnic hyperpnoea (NH) and control groups
This study found that a 4-week NH training reduced the incidence of respiratory symptoms, improved pulmonary function (except for DLCO) and quality of life, and reduced the level of depression in patients with chronic SCI, regardless of their neurological level of injury. These results indicate that it is not too late to start RMT with NH, even more than 24 months after injury.
In patients with recent SCI, no immediate or long-term improvements in lung function were found, even with the help of intermittent positive-pressure breathing therapy (15). Patients might be able to adapt to the situation and develop their own strategies for coping with the limitations. However, the limitations do not vanish and patients may subsequently develop depression (8). The current study revealed that improvement in lung function may be associated with a reduction in depression level, which coincides with the findings in the Postma’s study, in which they found that a decline in FVC may lead to negative changes in social functioning over years (9). Better lung function might have improved the patients’ well-being and quality of life, thus reduced their depression level. It may be helpful to develop new strategies for psychosocial recovery in patients with SCI, and this requires further investigation.
SGRQ and CAT are used widely for the assessment of patients with COPD. However, these 2 PROMs were not validated in patients with SCI, and some activities mentioned in these scales are not always relevant for such patients. Although significant differences were found between the NH and control groups in terms of these PROMs, these results should be interpreted with caution.
Previous studies have focused more on muscle strength compared with muscle endurance. In a retrospective study by Raab et al., inspiratory or combined inspiratory and expiratory muscle training was performed in a group setting with respiratory function measurements before and after the training period (16). They found that the training improved respiratory functions, but the relative improvements in combined respiratory muscle training were comparable with isolated inspiratory muscle training. As acknowledged by Raab et al., the study did not have a control group and the training groups were not randomized. In a randomized controlled trial by Roth et al., patients in the intervention group received expiratory muscle training (17). Only the value of maximum expiratory pressure was improved in the intervention group. Since the training focused only on expiration, we suspected that by also including inspiratory muscle training, improvement might also be observed in other lung function parameters. A study by Mueller et al. found that FEV1, PEF and maximal expiratory muscle pressure generating capacity increased only during inpatient rehabilitation, but not thereafter (18). However, this study failed to explore the effect of the rehabilitation programme, especially the influence of RMT during inpatient rehabilitation and thereafter. We reasoned that training of muscle endurance might be more suitable for patients with chronic SCI, given the slow progression of hypercapnic respiratory failure, while training of muscle strength might be more suitable for those with acute SCI. The improvement in MVV in the NH group also suggested better endurance compared with the control group (Table II). Two previous studies have shown the training effects of NH in SCI with a post-injury time between 2 and 8 months (4, 6). Mueller et al. found that inspiratory resistance training is more advantageous than NH regarding maximal inspiratory pressure, which was not surprising, since inspiratory resistance training focused on inspiratory muscle strength (6). To our knowledge, no study has examined the effect of NH on chronic SCI with a longer period after injury. Kim et al. considered training of both thoracic and abdominal muscles to be important for respiratory function (5). Their study included patients with SCI with a time post-injury > 3 years. The combined training showed a greater improvement compared with RMT focused on muscle strength alone. Although we did not include a group subjected to combined training, our results indicate that RMT with NH might have induced similar improvement as the combined training, given that the training period in our study was shorter (4 vs 8 weeks).
Several limitations were identified in the present study. The patients were not blinded to their group assignment, which is critical with respect to subjective evaluations with the questionnaires. Psychological influences on PROMs were not clear. In addition, the CAT and SGRQ were not validated in patients with SCI. Furthermore, no data from previous studies could be used to assess the sample size for comparing the effects on lesion levels. Hence, the number of patients for each lesion level was not considered in the randomization process. It may be more reasonable to divide the lesion levels into high, low cervical and thoracic. However, due to the limited number of patients, the comparison may not be adequate. Comparison with other RMT or combined training could be beneficial, but this was beyond the objective of this study. Further comparison with other RMT should be considered in future studies. Last, but not least, the sample size was small in this randomized study and the current findings need to be confirmed in a larger one. Nevertheless, the differences in lung function and quality of life between groups can be used for sample size estimation in future larger randomization studies.
We suggest that patients with chronic SCI could consider receiving RMT with NH, even a long period after injury. NH training may reduce the incidence of respiratory symptoms, improve pulmonary function and quality of life, and reduce depression in patients with chronic SCI, regardless of their neurological level of injury, even at more than 24 months after injury.
This work was financially supported by the project Beijing Rehabilitation Hospital of Capital Medical University (No. 2018–16).
Zhanqi Zhao receives a consulting fee from Dräger Medical. Inéz Frerichs reports funding by the European Union’s 7th Framework Program for Research and Technological Development (WELCOME, Grant Number 611223), the European Union’s Framework Program for Research and Innovation Horizon2020 (CRADL, Grant Number 668259) and reimbursement of speaking fees, congress and travel costs by Dräger Medical. The other authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize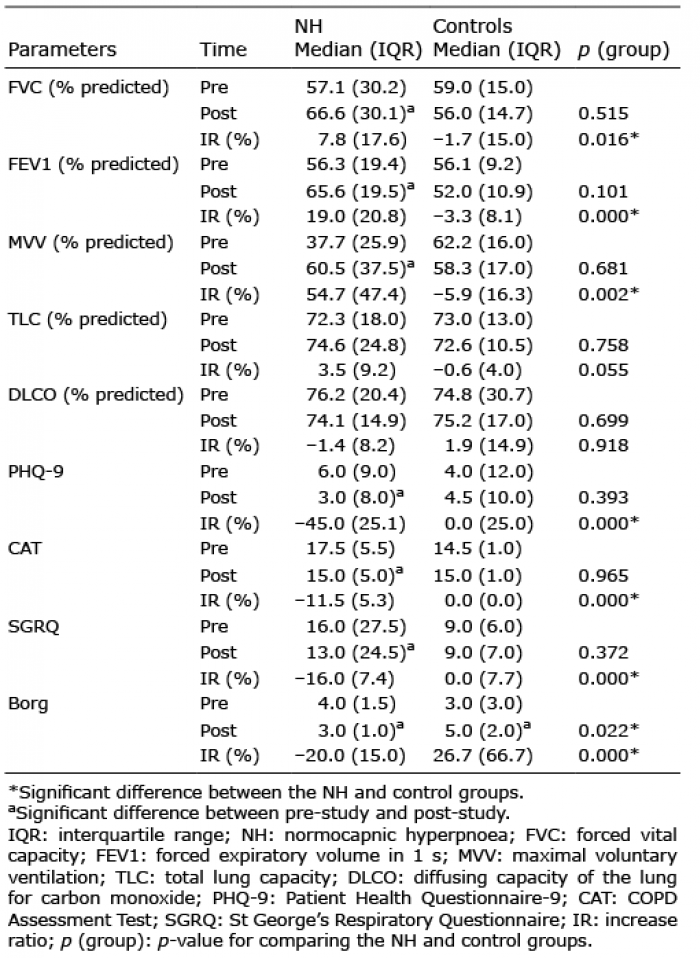 Click to show fullsize
Click to show fullsize