
From the 1Department of Pediatrics, McMaster University, 2School of Rehabilitation Science, McMaster University, 3CanChild Centre for Childhood Disability Research, Department of Pediatrics, McMaster University, and 4Department of Kinesiology, McMaster University, Hamilton, ON, Canada
Objective: To examine longitudinal changes in traditional and non-traditional risk factors for cardiovascular disease in individuals with cerebral palsy and to investigate relationships between age, Gross Motor Function Classification System (GMFCS) and risk of cardiovascular disease.
Methods: Individuals with cerebral palsy (n = 28 of 53 eligible participants; GMFCS levels I–V; follow-up mean age 35.1 years (standard deviation (SD) 14.4) participated in a longitudinal cohort study with 4.0 years (SD 1.2) follow-up. Traditional risk factors included waist circumference and systolic blood pressure. Non-traditional risk factors included carotid artery intima media thickness and distensibility, carotid-femoral pulse wave velocity, and flow-mediated dilation.
Results: Absolute (0.31 mm (SD 0.13) vs 0.22 mm (SD 0.08) , p = 0.045, 95% confidence interval (95% CI) 0.040, 0.151) and relative flow-mediated dilation (9.9 % (SD 4.7) vs 7.5 % (SD 2.6), p = 0.049, 95% CI 0.464, 4.42) decreased, while carotid artery intima media thickness (0.52 mm (SD 0.17) vs 0.67 mm (SD 0.33), p = 0.041, 95% CI –0.242, –0.074) increased from baseline to follow-up. No other risk factor changed significantly. Age at baseline was a significant independent predictor of carotid artery intima media thickness change (R-squared = 0.261, p = 0.031).
Conclusion: Individuals with cerebral palsy experience significant changes in non-traditional risk factors for cardiovascular disease over 4 years, in the face of no changes in traditional risk factors. Compared with findings in the literature from the general population, these risk factors progress at a faster rate and at a younger age in individuals with cerebral palsy.
Key words: cerebral palsy; cardiovascular disease; risk factor, endothelial function; arterial stiffness.
Accepted May 10, 2019; Epub ahead of print May 23, 2019
J Rehabil Med 2019; 51: 525–531
Correspondence address: Patrick G. McPhee, CanChild Centre for Childhood Disability Research, IAHS 408, McMaster University, 1400 Main Street West, Hamilton, Ontario L8S 1C7, Canada. E-mail: mcpheepg@mcmaster.ca
Recent research has shown that individuals with cerebral palsy are at increased risk of developing cardiovascular disease compared with the general population. However, no studies have investigated the progression of risk of cardiovascular disease in individuals with cerebral palsy over time. This study measured risk factors for cardiovascular disease in 28 individuals with cerebral palsy over a 4-year time period. Some risk factors for cardiovascular disease appeared to progress at a faster rate and at a younger age in people with cerebral palsy compared with the general population. It is recommended that clinicians measure risk factors for cardiovascular disease in this population early on, in order to prevent the development of cardiovascular disease later in life.
Cerebral palsy (CP) is the most common childhood physical disability (1). However, very little is known about the effects of ageing on individuals with CP. It is hypothesized that individuals with CP experience an accelerated ageing process that might be linked to an increased prevalence of secondary conditions, such as reduced range of motion, muscular strength, aerobic endurance and increased fatigue (2, 3). Adults with CP have been reported as overweight and/or obese (4), sedentary (5), engaging in low levels of physical activity (6), and hypertensive (7), all of which contribute to an increased risk of developing cardiovascular disease (CVD) (8).
CVD remains the leading cause of death globally, meaning that more people die annually from diseases related to the cardiovascular system than any other cause (9). The World Health Organization (WHO) acknowledged that many CVDs can be prevented by modification of behavioural risk factors, such as unhealthy diet, obesity, and physical inactivity (9). We recently conducted a systematic review that examined the prevalence of CVD, risk factors for CVD, and CVD-related mortality among adults with CP (10). An important finding was that CVD-related deaths were elevated in individuals with CP compared with the general population. However, the development and progression of CVD in this population remains poorly understood. A key limitation was a lack of longitudinal studies, of both ambulatory and non-ambulatory adults with CP investigating overweight/obesity, hypertension, other CVD risk factors and CVD itself. Indeed, Peterson et al. recently examined age-related trends in cardiometabolic disease in adults with CP from a de-identified nationwide claims database, and reported that age was a strong predictor of type 2 diabetes, hypercholesterolaemia, hypertension, cardiac dysrhythmias, and atherosclerosis, such that mean disease-free survival rates were significantly less for middle-aged (40–< 60 years) and older (≥ 60 years) subjects compared with young adults (18–< 40 years) (11). Despite the fact that this was the first longitudinal cohort study to investigate cardiometabolic disease in adults with CP, other important risk factors, such as gross motor function and physical activity, were unavailable for analysis and may have influenced the disease-free survival trends.
In addition to traditional risk factors for CVD (e.g. hypertension and increasing age), measures of arterial structure and function (12) have emerged as novel (i.e. non-traditional) independent risk factors for CVD. Specifically, physiological changes, such as reductions in elastin and increases in collagen formation, lead to a stiffer arterial wall and a widened pulse pressure, resulting in systolic hypertension. Measuring these non-traditional CVD risk factors could add prognostic value to the assessment and treatment of CVD in this population. We previously showed the feasibility of assessing non-traditional risk factors for CVD, including arterial stiffness and endothelial dysfunction through cross-sectional studies of adolescents (13) and adults with CP (8). A better understanding of change over time could assist clinicians to identify those individuals with CP who are most at risk of CVD, and may help institute and evaluate interventions to mitigate those risks. The objectives of this study were to examine longitudinal changes in both traditional and non-traditional risk factors for CVD in individuals with CP, and to investigate the associations between age and gross motor function with longitudinal changes in these risk factors.
This study was a component of the Stay-FIT program of research at CanChild, Centre for Childhood Disability Research. The purpose of the Stay-FIT programme of research is to promote physical activity and encourage an active lifestyle for individuals with CP across the lifespan. Adolescents and adults with CP (n = 53), who previously participated in cross-sectional studies (8, 13) within the Stay-FIT programme including cardiovascular health assessments, were invited to participate in this longitudinal study. All individuals with CP were eligible for the present study, regardless of intellectual ability and gross motor function. Participant or parent/caregiver written consent was obtained prior to study commencement. This study received local institutional review board approval (Hamilton Integrated Research Ethics Board Project #12-110).
All participants were invited to a research laboratory within a university setting to undergo a battery of cardiovascular health assessments. All participants arrived at the laboratory having abstained from food, caffeine and vigorous physical activity for at least 12 h prior to data collection. The visit began with measures of height and body mass, as reported previously (8). These were used to calculate body mass index (BMI; kg/m2). Waist circumference was measured to the nearest 0.5 cm at the end of a normal expiration 4 cm above the umbilicus with the participant in the supine position. Supine systolic, diastolic, and mean arterial blood pressures were measured using an automated blood pressure device (Dinamap PRO 100 series, Tampa, FL, USA). These assessments were performed by a clinical researcher with > 5 years’ experience collecting these measures in individuals with CP and spinal cord injury (first author (PM)). For the purpose of this study, waist circumference and systolic blood pressure (SBP) were included as traditional CVD risk factors. The Expanded and Revised version of the Gross Motor Function Classification System (GMFCS) (14) was used to determine level of gross motor function via self-report by participants.
Non-traditional risk factors and details pertaining to their data collection and analysis techniques are described below. All measures were performed with the participant in a supine position following 10 min of supine rest. A data acquisition system (Powerlab model ML795; ADInstruments, Colorado Springs, CO, USA) and software program (LabChart 8; ADInstruments, Colorado Springs, CO, USA) were used to acquire continuous heart rate and blood pressure during data collection. Heart rate was obtained using electrocardiography and blood pressure was obtained using finger photoplethysmography (Finometer MIDI, Finapres Medical Systems, Amsterdam, The Netherlands). The measurement protocols were identical at baseline and follow-up assessment time-points.
Carotid distensibility was acquired as an indicator of local carotid artery elasticity. This technique required a combination of brightness mode ultrasound with a 12 MHz probe (Vivid Q; GE Medical Systems, Horten, Norway) and applanation tonometry (model SPT-3-1; Millar Instruments, Houston, TX, USA). Simultaneous images and tonometer signals were acquired for 10 consecutive heart cycles. Distensibility was calculated as follows:
Distensibility (mmHg–1)=(π(dmax/2)2–π(dmin/2)2)/PP*π(dmin/2)2
where dmax was the mean maximum arterial lumen diameter, dmin was the mean minimum arterial lumen diameter, and PP is the mean pulse pressure of the carotid artery (difference between systolic and diastolic pressure) calculated from signals acquired using the applanation tonometer. A decrease in carotid distensibility is indicative of increased artery wall stiffness.
The same brightness mode ultrasound images that were collected for carotid distensibility were used to calculate carotid artery intima media thickness (cIMT). cIMT was measured as the distance (mm) from the lumen-intima to the media-adventitia interface at 100 sites along the arterial wall in the end diastolic frame for each of the 10 heart cycles and reported as a mean for each participant. An increase in cIMT is indicative of increased risk of CVD.
Carotid-femoral pulse wave velocity (cfPWV) is a regional measure and the gold standard assessment of arterial stiffness (15). cfPWV was determined from 20 continuous heart cycles and arterial pressure waveforms at the areas of greatest pulsation from the common carotid and superficial femoral arteries, and was calculated as follows:
cfPWV (m/s)=distance (m)/pulse transit time (s)
Distance was measured via the subtraction method as the distance from the sternal notch to the femoral site minus the distance from the sternal notch to the carotid site. An increase in cfPWV is indicative of increased arterial stiffness and subsequent risk for development of CVD.
Non-invasive assessment of endothelial function was measured using the flow mediated dilation (FMD) technique performed on the brachial artery. The FMD technique functions on the premise that increases in shear rate (a surrogate for shear stress in the absence of blood viscosity) cause vasodilation through an upregulation and/or production of nitric oxide, which causes a relaxation of the smooth muscle layer of the arterial wall, and a subsequent increase in arterial diameter. Ultrasound was used to acquire images of the brachial artery approximately 10 cm proximal to the antecubital fossa. Absolute and relative FMD values were calculated as reported previously (16). Reductions in absolute and/or relative FMD values over time are indicative of endothelial dysfunction and increased risk of CVD.
Statistical analyses were performed using STATA (version 13.1) statistical software package. Descriptive summary statistics for participants were calculated as means and SDs for continuous variables and as percentages for categorical data (i.e. sex and BMI categories).
To examine longitudinal changes in traditional and non-traditional risk factors for CVD in individuals with CP, repeated measures analysis of variance was performed. Dependent variables of interest included waist circumference, SBP, cIMT, carotid artery distensibility, cfPWV, and both absolute and relative FMD, while time-point (baseline and follow-up) was the independent variable. Difference in age (in months) between baseline and follow-up assessments was entered as a covariate to control for the differences in time between assessments for participants.
To investigate the relationships between age and gross motor function with longitudinal changes in traditional and non-traditional risk factors for CVD, multiple linear regressions were performed. Dependent variables consisted of waist circumference, SBP, cIMT, carotid artery distensibility, cfPWV, absolute and relative FMD. The regression models included both age at baseline (as a continuous variable) and GMFCS (dichotomous indicator variable; ambulatory (GMFCS I–II) vs non-ambulatory (GMFCS III–V)) as independent variables. A leverage vs residual squared plot was generated to determine data points of high influence (i.e. outliers) followed by calculating Cook’s distance to confirm data points of high influence, with those having a score ≥ 0.1 removed. Statistical significance was set at an alpha criterion (0.05). A sample size calculation was performed to determine the number of participants required to examine longitudinal changes in CVD risk factors in individuals with CP with 80% power. Our sample was derived using a one-tailed test and a medium effect size (0.5). Based on these parameters, the target sample size would be 27.
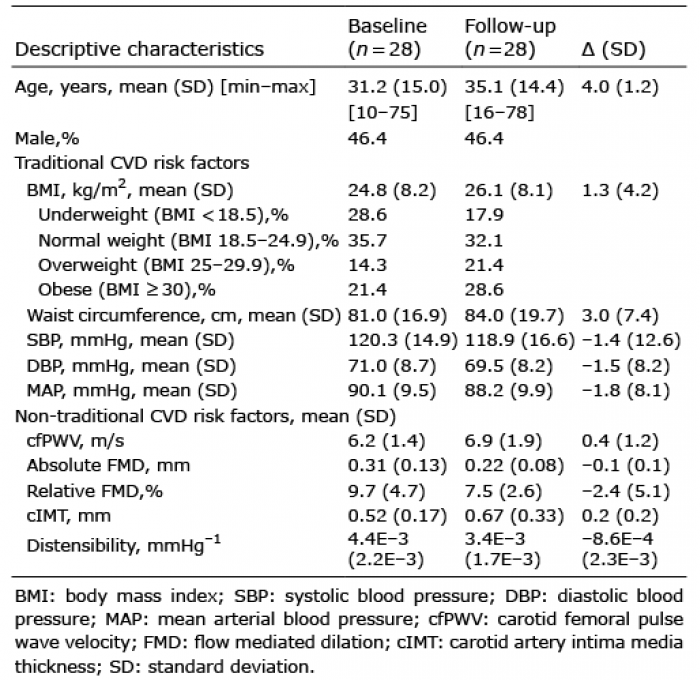
Descriptive characteristics of the study participants are presented in Table I. Twenty-eight of the 53 eligible participants agreed to participate in the follow-up assessments. The remaining 25 participants did not participate for various reasons, some of which included: no longer living in Southwestern Ontario, not willing to participate in follow-up research, or the contact information that was on file was no longer accurate. In addition, the time period between baseline and follow-up assessment could have been up to 7 years for some participants, based on the time period of the adolescent study (13); this probably contributed to the reasons for non-participation in the follow-up assessment, as other life demands could have taken over. It was possible that individuals who participated in the follow-up component of this study might be a selection of more healthy participants compared with those who did not participate; however, 2 sample t-tests performed for age, and traditional and non-traditional risk factors for CVD at baseline between participants who participated in the follow-up and those who did not revealed no significant between-sample differences for all variables (i.e. p > 0.05). Our goal was to include all 53 individuals for follow-up assessments; however, our sample size calculation confirmed that an n of 28 was reasonable to investigate the longitudinal effects in this study design.
Table I. Descriptive characteristics and measures of risk factors for cardiovascular disease (CVD) in individuals with cerebral palsy (CP) at baseline and follow-up
GMFCS distribution was as follows: I = 6; II = 7; III = 5; IV = 7; V = 3. The mean time interval between baseline and follow-up assessments was 4.0±1.2 years. Changes in CVD risk factors between baseline and follow-up are shown in Table I. Between baseline and follow-up assessments at the group level, 64% of participants had an increase in waist circumference, absolute and relative FMD decreased in 85% of participants, 93% of participants experienced an increase in cIMT, carotid distensibility decreased in 59% of participants, and cfPWV increased in 70% of participants. Three participants at follow-up had cfPWV values that were above the clinical value (i.e. 10 m/s) deemed at risk for future cardiovascular events, whereas only one participant was at risk at baseline. With difference in age in months included as a covariate, repeated measures analysis of variance revealed statistically significant differences in mean absolute FMD (0.31 (SD 0.13) vs 0.22 (SD 0.08) mm, p = 0.045 95% CI 0.040, 0.151), relative FMD (9.9 (SD 4.7) vs 7.5 (SD 2.6) %, p = 0.049, 95% CI 0.464, 4.42), and cIMT (0.52 (SD 0.17) vs 0.67 (SD 0.33) mm, p = 0.041, 95% CI –0.242, –0.074) between baseline and follow-up assessments, respectively.
As a result of the varying time intervals between the 2 sets of assessments between participants, changes in traditional and non-traditional risk factors were divided by time for each participant and reported as rates of change for the regression analyses. Multiple linear regression analysis for rate of change in cIMT revealed an R-squared of 0.294, p = 0.015, with age at baseline being a significant predictor of change in cIMT. From Cooks distance calculation, participant 19 (age = 58 years; GMFCS III; change in cIMT = 1.07 mm) was identified as an outlier with a residual of 0.14. The regression was performed without this data point, resulting in an R-squared of 0.261, p = 0.031 and again with age at baseline being a significant predictor of change in cIMT (Table II). Age at baseline and/or GMFCS grouping were not significant predictors of rates of change for waist circumference, SBP, carotid artery distensibility, cfPWV, and both absolute and relative FMD (Table II).
Table II. Multiple linear regression analyses
The objective of this study was to examine the longitudinal changes in traditional and non-traditional risk factors for CVD in a cohort of individuals with CP, in order to better understand the development of CVD in this population. An important finding was that, while risk factors for CVD increased in at least 50% of participants with CP relative to baseline over approximately a 4-year time period, some non-traditional indices seemed to have higher sensitivity for detecting significant changes over time. Specifically, after controlling for the varying time intervals between baseline and follow-up assessments among participants, significant changes were apparent only for the non-traditional risk factors absolute FMD, relative FMD, and cIMT. Importantly, this informs us that non-traditional measures may detect changes in CVD risk in individuals with CP when not revealed by tracking traditional risk factors, which is consistent with the pathophysiology of the cardiovascular system in general; functional impairment of the arterial wall may occur at an early stage of the atherosclerotic process, before clinical symptoms of CVD are present (17).
Concerning traditional risk factors for CVD, obesity and hypertension have shown a strong association with the non-traditional risk factors arterial stiffness and endothelial dysfunction. In fact, some non-traditional risk factors are considered negative prognostic factors of hypertension (18, 19). The increases in waist circumference and significant changes in FMD and cIMT within this cohort of individuals with CP underscore the importance of monitoring and managing CVD risk in this population to prevent the development of hypertension.
As this was the first longitudinal cohort study to investigate changes in non-traditional CVD risk variables in individuals with CP, it was important to understand these findings in the context of the general population. A longitudinal study completed in older adults (mean age 60 ± 9 years) found that cfPWV increased from 9.6 to 10.4 m/s in a 4–6-year time-period (20). Comparably, we found a modest increase in cfPWV from 6.2 to 6.9 m/s in a similar time period (i.e. 4 years), but in a much younger cohort of individuals with CP (mean age 31.2 ± 15.0 years at baseline). In addition, there is well-established literature demonstrating that advancing age is the strongest predictor of increases in cfPWV (18, 21), and we previously found age to be significantly associated with cfPWV in a cross-sectional analysis of 42 adults with CP (8). However, our current multiple regression analysis did not reveal age to be associated with rate of change in cfPWV in the present study, which, in addition to younger age at baseline, might be explained by a combination of the small magnitude of observed changes in cfPWV and the small sample size. Similarly, cIMT increases with age due to changes to the structural components of the arterial wall, particularly thickening of both the intima and media layers; in the general population, cIMT increases by approximately 3-fold between the ages of 20 and 90 years (22). The 1st Screening for Heart Attack Prevention and Education (SHAPE) Program identified an individual to be at high risk for subclinical atherosclerosis when a cIMT ≥ 1 mm is present (23). Considering the information in the SHAPE guideline, 2 individuals in the present study were at high risk for subclinical atherosclerosis from cIMT alone. A study in a cohort of 70-year-old Swedish adults found that cIMT significantly increased from 0.88 to 0.95 mm over a 5-year period (24). The present study found a larger relative increase in cIMT compared with the Swedish cohort. Also, age was a strong significant predictor of cIMT change in our study, which is consistent with what is known in the general population and further supports our findings from cross-sectional work (8). In addition to age, another important variable to consider when examining CVD risk is hormonal development. Specifically, literature has shown that estrogen might have a cardioprotective effect on the cardiovascular system (25); however, this topic remains controversial (26). While this was the first longitudinal study that examined cardiovascular health in individuals with CP and demonstrated change over time, we recommend investigating the effect of age and sex, in particular metabolic and hormonal effects on cardiovascular health, in future studies.
Few studies have examined longitudinal changes in brachial artery FMD from adolescence to adulthood. A study in children and adolescents with type 1 diabetes mellitus observed a significant decrease in FMD in approximately a 3-year follow-up period (27); whereas no significant change in FMD was observed after a 5-year follow-up study in older adults (24). The latter study observed a significant inverse relationship between change in FMD and change in LDL-cholesterol (24), whereas the former study observed an inverse relationship between glycaemic control and FMD (27). It is plausible that metabolic markers could be associated with change in FMD in individuals with CP; however, we did not measure these in the current study. At the very least, we know that age and gross motor function were not significantly associated with change in FMD in the present cohort. Given the recent work by Peterson et al. (28) and Ryan et al. (29) pointing towards adolescents and adults with CP having an elevated risk of cardiometabolic disease, it is important for future work to include cardiometabolic markers to advance our understanding of the regulation of endothelial function in this population. Indeed, we did observe a (non-significant) increase in waist circumference; however, our modest sample size limited our ability to include waist circumference as an independent predictor in linear regression analysis. Finally, a significant decrease (1.1E–3 mmHg–1) in carotid artery distensibility between baseline and follow-up assessment was observed in our cohort. In a large cohort of men and women free of CVD (45–84 years old), carotid artery distensibility decreased by 0.41E–3 mmHg–1 over a mean period of 9.4 years, and SBP was associated with accelerated stiffening (30). A larger decrease in distensibility that was not associated with age or gross motor function was observed. Taken together, our findings provide initial support for the argument that individuals with CP experience accelerated ageing for disease progression, specifically non-traditional CVD risk factors, in comparison with the general population. In light of recent research that identified young adults with CP at increased risk of CVD compared with age-matched controls from the general population (31), early detection of the development of CVD, particularly by assessing non-traditional risk factors for CVD, can lead to more effective strategies for the prevention of CVD in this population.
There are important limitations to address in this cohort study. The main limitation was the small sample size. While the sample size of 28 individuals did allow us to examine longitudinal changes in CVD risk factors in the total group, we were unable to determine whether other factors (e.g. waist circumference and sex hormones) were associated with the observed changes in CVD risk variables. Secondly, the large age range would have been best examined in age groups with a statistically representative sample size. However, the large age range provided support for us to investigate the effects of age on traditional and non-traditional risk factors for CVD. Thirdly, we did not include a direct comparator group, as this was not the primary objective of the study. Instead, we referenced studies that have investigated changes in non-traditional risk factors for CVD in the general population to characterize the relevance of our findings. However, a matched cohort group of typically developing adolescents and adults undergoing the same assessments of CVD risk using the same techniques would provide subsequent support for altered risk patterns in this population. Another limitation was that we did not collect medication lists from each participant. However, none of the participants reported a medical history of CVD. Finally, we adopted BMI cut-points from the adult population in this study, despite 4 participants at baseline and one participant at follow-up being under 18 years of age.
This was the first study to provide longitudinal evaluation of traditional and non-traditional risk factors for CVD in individuals with CP. Changes in risk factors for CVD were observed in the majority of individuals with CP at a relatively young age over a relatively short period of time (i.e. 4 years). Key implications from this study include evidence for the importance of clinical screening for CVD risk, particularly measuring cIMT and brachial artery FMD, to assess changes over time in individuals with CP in adolescence and adulthood. The findings will be used to inform future studies to further understand and improve cardiovascular health in individuals ageing with CP, ideally in a larger sample size with an opportunity to include other health variables that might explain risk of CVD in this population (e.g. sex hormones, nutrition status, physical activity, medications, etc.). This is particularly important, as persons with CP represent a population that is living longer, yet changes to their clinical health remain to be determined.
Dr Jan Willem Gorter holds the Scotiabank Chair in Child Health Research.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize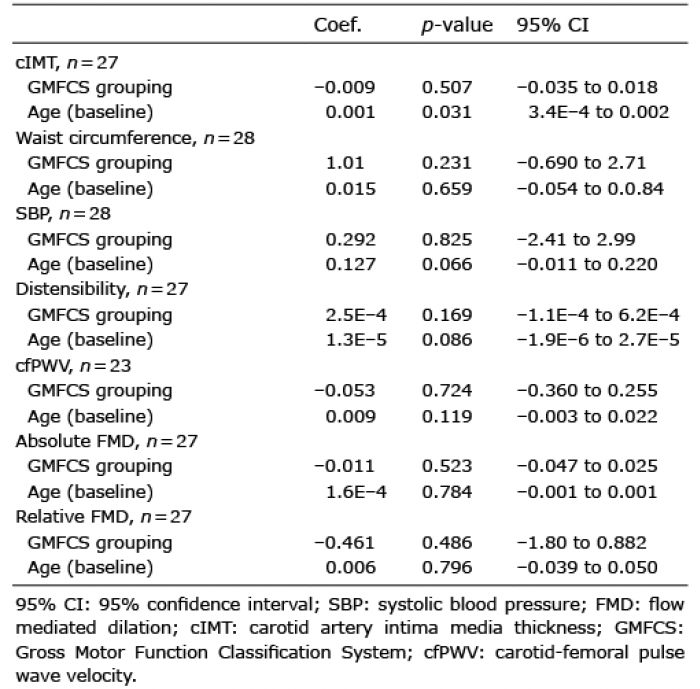 Click to show fullsize
Click to show fullsize