
From the 1Department of Rehabilitation Medicine, Daegu Fatima Hospital, 2Department of Rehabilitation Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, South Korea
Objective: To investigate the association of metabolic syndrome with the development of knee osteoarthritis.
Design: Cross-sectional nationwide survey study.
Subjects: Data obtained from the 2010–2012 Korea National Health and Nutrition Examination Survey.
Methods: Subjects aged 50 years or older were included. Knee osteoarthritis (≥grade 2 Kellgren-Lawrence) and severe knee osteoarthritis (≥grade 3 Kellgren-Lawrence) were evaluated based on radiological findings. Medical information and demographic data were obtained from survey records. Multivariate regression analysis was performed to investigate the relationship between knee osteoarthritis and metabolic syndrome, and the number of metabolic syndrome components for dose-response relationship evaluation. Analyses were adjusted by age group (model 1) or by age group, education, smoking, alcohol consumption, and physical activity (model 2).
Results: A total of 8,491 subjects (3,684 men and 4,807 women) were included in the study. In women, metabolic syndrome increased the risk of knee osteoarthritis (odds ratio (OR) = 1.644, p < 0.001; and OR = 1.608, p < 0.001; respectively; for models 1 and 2) and severe knee osteoarthritis (OR = 1.593, p < 0.001; and OR = 1.559, p < 0.001; respectively; for models 1 and 2). However, in men, knee osteoarthritis and severe knee osteoarthritis were not associated with metabolic syndrome. As the number of metabolic syndrome components increased, knee osteoarthritis and severe knee osteoarthritis generally increased in women, but not in men.
Conclusion: Metabolic syndrome affects the development of knee osteoarthritis and severe knee osteoarthritis in women. In addition, dose-response relationships were observed between metabolic syndrome components and knee osteoarthritis in women, but not in men.
Key words: metabolic syndrome; osteoarthritis; abdominal obesity; hypertension; hyperglycaemia; hyperlipidaemia.
Accepted May 3, 2019; Epub ahead of print May 16, 2019
J Rehabil Med 2019; 00: 00–00
Correspondence address: Won Kim, Department of Rehabilitation Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, South Korea. E-mail: duocl79@gmail.com
Knee osteoarthritis is a common disorder in old age and is known to be associated with various medical conditions. Metabolic syndrome is a cluster of conditions including hypertension, dyslipidemia, abdominal obesity, and insulin resistance, with a rapidly increasing prevalence. The purpose of our study was to investigate the effect of metabolic syndrome on development of knee osteoarthritis. The result showed that metabolic syndrome affects the development of knee osteoarthritis and severe knee osteoarthritis in women. Additionally, the number of metabolic syndrome components showed additive effect on development of knee osteoarthritis. However, these relationships were not definite in men. Through our study, we were able to connect the impact of metabolic syndrome on knee osteoarthritis. Careful and thorough examination of knee osteoarthritis should be considered in patients complaining of knee pain in case of metabolic syndrome patient. Also, treatment of the components of metabolic syndrome should be emphasized, such case.
Knee osteoarthritis (OA) is a common musculoskeletal disorder in old age. It presents with joint pain and stiffness, and consequently reduces individual function and quality of life (1). Knee OA affects over 250 million people globally (2). It is expected that this number will increase rapidly in the future, as longer life expectancy leads to a growing elderly population (3). Mechanical stress has been considered the primary cause of the development of knee OA, and higher prevalence in old age and obesity suggest a relationship between mechanical stress and knee OA. Sex is another risk factor; women are at a higher risk than men (4). However, many researchers have recently suggested that other factors, such as genetic, neuroendocrine, and metabolic factors, may also play a role in the pathophysiological mechanism of knee OA (5).
Metabolic syndrome refers to a cluster of conditions, including hypertension, dyslipidaemia, abdominal obesity, and insulin resistance, with a rapidly increasing prevalence (6). In the presence of metabolic syndrome, general or local inflammatory reactions increase, and advanced glycation end-products accumulate or local ischaemia develops (7). These may contribute to the development of OA. Researchers have studied the association of the metabolic effects of diabetes and obesity with the development of OA. However, the results have been inconsistent. In addition, most studies only investigated the relationship between individual metabolic conditions and OA (8–11). The relationship between metabolic syndrome and development of OA has not been fully studied. Some studies have linked OA to metabolic syndrome, on the basis that OA is not only a mechanical disease, but also a metabolic disease (12, 13).
Therefore, the aim of the current study was to investigate the association of metabolic syndrome with the development of knee OA, based on a nationwide survey. In addition, the study attempted to identify the relationship between the number of metabolic syndrome components and development of knee OA
The data used in this study were obtained from the fifth Korea National Health and Nutrition Examination Survey (KNHANES). This was conducted from 2010 to 2012 by the Korea Centers for Disease Control and Prevention. The KNHANES is a nationwide, representative survey. Participants were selected using a multi-stage clustered and stratified random-sampling method. The sampling method considered the residential area, sex, and age group based on the National Census Data. The fifth KNHANES was conducted in 25,534 subjects (11,616 men, 13,918 women), and 10,152 subjects were 50 years of age or older. From this pool of subjects, those who had complete data on components of metabolic syndrome, plain knee radiographs, height, body weight, level of physical activity (PA), smoking, alcohol consumption, and educational status were selected. All subjects provided informed consent. This study was approved by the institutional review board (IRB) of our hospital (IRB No. 2016-1354).
Metabolic syndrome was diagnosed using the criteria of the National Cholesterol Education Program Adult Treatment Panel III (14). Subjects with 3 or more of the following criteria were considered as having metabolic syndrome: high blood pressure (≥ 130/85 mmHg) or use of antihypertensive medication; fasting glucose ≥ 100 mg/dl or undergoing treatment for diabetes; abdominal obesity (waist circumference ≥ 90 cm in men and ≥ 80 cm in women); and fasting triglyceride ≥ 150 mg/dl or high-density lipoprotein cholesterol (HDL-C) < 40 mg/dl in men and < 50 mg/dl in women (15).
The cut-off values applied for the criterion of abdominal obesity in Korean adults were proposed by The Korean Society for the Study of Obesity (16). The criterion for hyperglycaemia was adopted from the American Diabetes Association guidelines (17).
Knee OA was assessed using radiographs. Plain anterior-posterior and lateral radiographs of the knee were taken routinely on a representative sample of KNHANES participants using DigiRAD-PG (Sitec Medical Co., Seoul, South Korea). Knee radiographs were taken according to a standard protocol, with the film centred 1 cm below the patellar apex for both the anterior-posterior and lateral views. Two radiologists performed the evaluation individually, using the Kellgren-Lawrence (KL) grading system. Participants with KL grade 2 or greater were defined as having knee OA, and participants with KL grade 3 or greater were defined as having severe knee OA (18). If the radiologists assigned different KL grades in the same case, another radiologist provided an opinion to achieve consensus. The weighted kappa coefficient for inter-rater reliability was 0.6522, indicating moderate reliability.
In the initial survey, body weight, height, and waist circumference were measured using standard protocols. Body mass index (BMI) was calculated (kg/m2). Obesity was defined as BMI ≥ 25 kg/m2, in accordance with the criteria of the Asia-Pacific region.
For the assessment of other possible contributing factors, age, education, alcohol consumption, smoking, obesity, and range of PA were included in the analysis. Participants were divided into 4 age groups: 50–59, 60–69, 70–79 and ≥ 80 years. The level of education was classified as elementary school graduate or below, middle-school graduate, high-school graduate, or college graduate or above. Smoking status was categorized as current smoker or non- or ex-smoker. Alcohol consumption was divided into those drinking twice a week or more and those drinking less than twice a week. The Korean version of the International Physical Activity Questionnaire-Short Form, which includes questions regarding the frequency, duration, and intensity of recent PA, was used to assess the participants (19). PA was defined as follows: vigorous PA, vigorous activity of at least 20 min on 3 days or more in a week; moderate PA, moderate-intensity activity of at least 30 min on 5 days or more in a week; walking, more than 30 min of walking on 5 days or more in a week; strength and flexibility exercises, strength and flexibility exercises on 2 days or more in a week.
Univariate and multivariate logistic regression analyses were performed to identify associations between metabolic syndrome and knee OA or severe knee OA. To accommodate the effect of covariates, Model 1 was adjusted for age group, which has the most definite effect on development of OA. Model 2 was adjusted for additional environmental factors; age group, education, smoking, alcohol consumption, and PA. In addition, the relationship between the number of metabolic syndrome components and development of knee OA, and the effect of each component, adjusted by 5 metabolic components, on the development of knee OA were analysed, in the same manner. The results were presented as means with 95% confidence intervals (95% CI). The odds ratios (OR) were calculated with the corresponding p-values < 0.05. Sampling weights were applied to each participant’s data to represent the Korean population without biased estimates. All statistical analyses were applied using SAS, version 9.4 (SAS Institute, Cary, NC, USA).
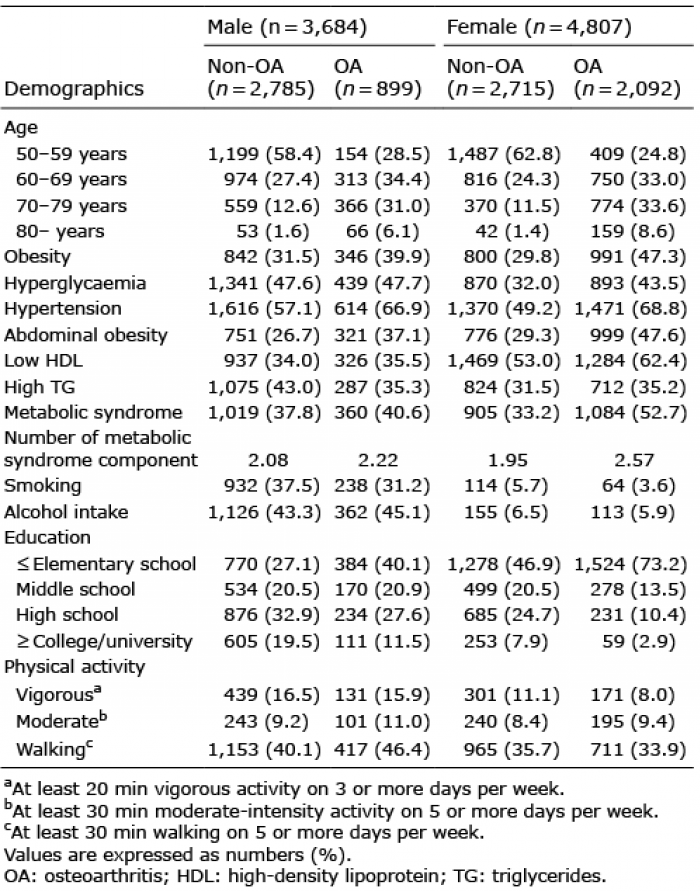
A total of 8,491 subjects (3,684 men and 4,807 women) were included, and 1,661 subjects were excluded among the subjects who were 50 years of age or older. The overall prevalence of knee OA was 35.2% (n = 2,991). Among subjects with knee OA, 59.8% (n = 1,790) had severe knee OA. Clinical characteristics according to the presence or absence of knee OA are shown in Table I. The prevalence of knee OA was 24.4% (n = 899) in men and 43.5% (n = 2,092) in women. The prevalence of severe knee OA among subjects with knee OA were 42.7% (n = 384) in men and 67.2% (n = 1,406) in women. Compared with subjects who did not have knee OA (men, 37.8%, women, 33.2%), more subjects with knee OA were diagnosed with metabolic syndrome, especially in women (men, 40.6%, women, 52.7%). The mean number of metabolic syndrome components was also higher in women with knee OA.
Table I. Demographics of the participants
In the univariate analysis, metabolic syndrome increased the risk of developing knee OA (OR = 2.24, 95% CI = 1.94–2.58, p-value< 0.001) and severe knee OA (OR = 2.22, 95% CI = 1.90–2.60, p-value< 0.001) in women (Table II). After adjusting for age group (model 1), metabolic syndrome increased the risk of developing knee OA (OR = 1.64, 95% CI = 1.41–1.91, p-value < 0.001) and severe knee OA (OR = 1.59, 95% CI = 1.36–1.87, p-value < 0.001) in women. After adjusting for all other environmental factors (model 2), metabolic syndrome also increased the risk of developing knee OA (OR = 1.61, 95% CI = 1.38–1.87, p-value < 0.001) and severe knee OA (OR = 1.56, 95% CI = 1.33–1.84, p-value < 0.001) in women. However, these associations were not observed in the univariate and multivariate analyses in men.
Table II. Odds ratio for development of knee osteoarthritis (OA)and severe knee OA in metabolic syndrome patients
In women, the risk of knee OA and severe knee OA increased as the number of metabolic syndrome components increased (Table III). In the univariate analysis of risk of knee OA, the highest OR was observed in subjects with 4 metabolic syndrome components (OR = 4.85, 95% CI = 3.54–6.65, p-value < 0.001). The same results were observed in model 1 (OR = 2.63, 95% CI = 1.89–3.66, p-value < 0.001) and model 2 (OR = 2.45, 95% = CI 1.75–3.43, p-value < 0.001). However, in the univariate analysis of risk factors of severe knee OA, the highest OR was observed in subjects with 5 metabolic syndrome components (OR = 5.47, 95% CI = 3.54–8.44, p-value < 0.001). In model 1, the highest OR was observed in subjects with 5 metabolic syndrome components (OR = 2.81, 95% CI = 1.77–4.46, p-value < 0.001). However, in model 2, the highest OR was observed in subjects with 4 metabolic syndrome components (OR = 2.51, 95% CI = 1.67–3.78, p-value < 0.001).
Table III. Odds ratio for development of knee osteoarthritis (OA) and severe knee osteoarthritis in accordance with number of metabolic syndrome components
In men, however, the risk of knee OA only increased in subjects with 5 metabolic syndrome components, compared with subjects with no metabolic syndrome components (OR = 1.80, 95% CI = 1.06–3.08, p-value = 0.031 and OR = 1.82, 95% CI = 1.05–3.17, p-value = 0.033, respectively, for models 1 and 2).
In women, hypertension was associated with an increased risk of knee OA (OR = 2.28, 95% CI = 1.96–2.65, p-value < 0.001; OR = 1.96, 95% CI = 1.68–2.29, p-value < 0.001; and OR = 1.25, 95% CI = 1.06–1.47, p-value = 0.009, respectively, in the univariate analysis with models 1 and 2) and severe knee OA (OR = 2.54, 95% CI = 2.15–3.00, p-value < 0.001; OR = 2.18, 95% CI = 1.84–2.59, p-value < 0.001; and OR = 1.36, 95% CI = 1.14–1.62, p-value < 0.001; respectively; for univariate analysis in models 1 and 2) (Table IV). Abdominal obesity showed the same results for risk of knee OA (OR = 2.19, 95% CI = 1.88–2.55, p-value < 0.001; OR = 1.85, 95% CI = 1.58–2.17, p-value < 0.001; and OR = 1.89, 95% CI = 1.60–2.23, p-value < 0.001; respectively; for univariate analysis in models 1 and 2) and severe knee OA (OR = 2.29, 95% CI = 7.96–2.68, p-value < 0.001; OR = 1.92, 95% CI = 1.64–2.26, p-value < 0.001; and OR = 2.00, 95% CI = 1.68–2.38, p-value < 0.001; respectively; in univariate analysis with models 1 and 2).
Table IV. Odds ratio for development of knee osteoarthritis (OA) and severe knee osteoarthritis in accordance with each metabolic syndrome component
In men, hypertension was associated with an increased risk of knee OA in the univariate analysis (OR = 1.52, 95% CI = 1.25–1.86, p-value < 0.001), model 1 (OR = 1.51, 95% CI = 1.23–1.86, p-value < 0.001), and model 2 (OR = 1.33, 95% CI = 1.07–1.66, p-value = 0.012). Hypertension was also associated with an increased risk of severe knee OA in model 1 (OR = 1.40, 95% CI = 1.03–1.90, p-value = 0.033). Abdominal obesity was associated with an increased risk of knee OA in the univariate analysis (OR = 1.62, 95% CI = 1.32–1.98, p-value< 0.001), model 1 (OR = 1.63, 95% CI = 1.31–2.02, p-value < 0.001), and model 2 (OR = 1.59, 95% CI = 1.27–2.00, p-value = 0.012). It was also associated with an increased risk of severe knee OA in models 1 (OR = 1.62, 95% CI = 1.22–2.15, p-value < 0.001) and 2 (OR = 1.56, 95% CI = 1.17–2.08, p-value = 0.003).
In men, hypertriglyceridemia was associated with a reduced risk of knee OA in the univariate analysis (OR = 0.72, 95% CI = 0.60–0.88, p-value < 0.001) and in model 1 (OR = 0.64, 95% CI = 0.52–0.78, p-value < 0.001). It also was associated with a reduced risk of severe knee OA in model 1 (OR = 0.59, 95% CI = 0.44–0.79, p-value < 0.001). However, the associations were not significant with knee OA (OR = 0.82, 95% CI = 0.66–1.01, p-value = 0.059) and severe knee OA (OR = 0.79, 95% CI = 0.58–1.06, p-value = 0.117) in model 2.
This study utilized data from a nationwide survey to assess the relationship between objectively defined metabolic syndrome and knee OA. Additional analyses were performed to appraise the dose-response relationship of the number of metabolic syndrome components and the effect of individual metabolic syndrome components on knee OA. In women, metabolic syndrome was associated with the development of knee OA and severe knee OA. Furthermore, the number of metabolic syndrome components was associated with the development of OA. However, this relationship was not established in men.
The prevalence of knee OA and severe knee OA was higher in women with metabolic syndrome than in men. This was consistent with previous studies that reported an association between metabolic syndrome components and development of knee OA. In a study by Engström et al. based on a Western population, the result showed that after adjusting for age, sex, smoking, physical activity, and C-reactive protein, the presence of metabolic syndrome was associated with a significantly increased risk of knee OA (20). A study using nationwide data reported that metabolic syndrome and the development of knee OA showed no association after adjusting for confounding factors, such as age and sociographic factors of exercise, alcohol intake and smoking (15). This, however, may be due to the fact that diagnosis of knee OA was performed in a self-reporting manner. The current study used radiological findings to diagnose knee OA more accurately. In the presence of metabolic syndrome, mechanical effects of high body weight may influence the development of knee OA (21). Recently, however, the emphasis has been on the metabolic effects of metabolic syndrome. Yusuf et al. reported that overweight is associated with increased risk of OA in non-weight-bearing joints of the hand (22). A meta-analysis showed that type 2 diabetes increased the risk of OA, after adjustment for body weight (9). The results of the current study in a nationwide representative population also support the relationship between metabolic syndrome and OA in women.
To determine the dose-response relationship of metabolic effects, we analysed the association between the number of metabolic syndrome components and development of knee OA or severe knee OA. In women, the risk of knee OA and severe knee OA tended to increase as the number of metabolic syndrome components increased. In a study by Yoshimura et al. that showed similar results, 3 or more metabolic syndrome components in men, and 2 or more metabolic syndrome components in women were associated with increased risk of knee OA (23). However, the fact that the study result was similar in both men and women was in contrast with the results of our study, which showed no significant relationship in men. The difference between the 2 studies might be because of the different study populations and diagnostic criteria for knee OA.
The current study performed additional analyses on the group with more severe knee OA. The reason was that, in severe cases, knee OA is more symptomatic and often requires special attention and more aggressive treatment than less severe cases. The aim was to elucidate the different impact that MS might have on more severe cases of knee OA. In addition, unlike the study by Yoshimura et al., we stratified the number of metabolic syndrome components from 0 to 5, which helped to identify more detailed dose-response relationships with metabolic syndrome components. Contrary to our expectation, the risk of knee OA was highest in patients with 4 metabolic syndrome components, rather than with 5 components. Various factors, such as general medical condition, individual lifestyle or activity, may have influenced this finding. Further study is needed to determine the exact mechanism. However, in the aforementioned studies, including our study, the different effect size of each component was not considered. This was a limitation of these dose response analyses.
In men, a significant relationship between metabolic syndrome and knee OA was not definite. The presence of metabolic syndrome was not associated with the development of knee OA and severe knee OA. In addition, in a dose-response analysis, the risk of knee OA only increased in men with 5 metabolic syndrome components. As knee OA is more common in women, who are more vulnerable to other risk factors for knee OA, it can be assumed that women are more vulnerable to metabolic risk factors for the development of knee OA (4, 24). However, further basic research regarding metabolic markers is needed to confirm the mechanism of the different responses in men and women.
In a component analysis, abdominal obesity and hypertension was generally associated with increased the risk of knee OA and severe knee OA in both sexes. Obesity is a well-known risk factor for OA (8, 25). Abdominal obesity might affect knee OA development by the combined metabolic effects of adipose tissue and mechanical stress of body weight. In our study, hypertension, in addition to abdominal obesity, was significantly associated with an increased risk of knee OA. The association was valid even after adjusting for abdominal obesity. Moreover, this relationship was also present in men. Zhang et al. reported that multiple genes or the proinflammatory cytokine interleukin-6 plays an important role in the association between hypertension and knee OA (26). Yoshimura et al. also clarified that hypertension was significantly associated with the occurrence of knee OA and vice versa (23, 27). Other metabolic syndrome components, apart from abdominal obesity and hypertension, showed a significant association with the development of knee OA in several analysis models. However, after adjusting for all compounding factors in model 2, the effects were insignificant. Nevertheless, caution is needed in determining the individual effect of each component based solely on the results of the current study, because every metabolic component interacts with, and usually coexists with, other components. Considering the dose-response relationship for metabolic syndrome components, each factor has an effect on the development of knee OA with some interactions and accumulative effects.
The present study has several strengths. First, not only did it investigate the association between the presence of metabolic syndrome and development of knee OA, but it also evaluated the dose-response relationship by considering the number of metabolic syndrome components. Moreover, this study assessed the individual effect of each metabolic syndrome component. These analyses revealed that some components may be more associated with the development of knee OA than other components. Secondly, the current study evaluated knee OA in an objective manner, using radiographic images. In addition, it divided the disease into knee OA and severe knee OA, based on the KL grading system. Therefore, it was possible to make a more detailed analysis. Thirdly, participants were divided and analysed by sex, and substantial differences were confirmed between the 2 groups. Fourthly, the current study was based on a nationwide representative large-sample survey. Thus it was possible to reduce selection bias and the results are applicable to the general population.
The current study also has some limitations. First, it was a cross-sectional study, and thus could not establish a causal relationship between metabolic syndrome and knee OA. Secondly, various risk factors that may affect the development of knee OA were adjusted for, but there could be more factors affecting the development of OA that need to be adjusted. Thirdly, there were many fewer men with OA than women with OA, which will have reduced the statistical power to investigate associations in men.
Overall, the results of this study showed that the presence of metabolic syndrome was associated with increased risk of knee OA and severe knee OA in women. The risk of knee OA in women increased as the number of metabolic syndrome components increased. However, these findings were not definite in men. Hypertension and abdominal obesity were significantly associated with the development of knee OA and severe knee OA in women. In men, abdominal obesity and hypertension significantly increased the risk of knee OA, but only abdominal obesity increased the risk of severe knee OA. Further studies are needed to determine the exact mechanism by which metabolic syndrome affects the development of knee OA.
This study was supported by a grant (2017–661) from the Asan Institute for Life Sciences, Asan Medical Center, Seoul, South Korea.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
The authors have no conflicts of interests to declare.


 Click to show fullsize
Click to show fullsize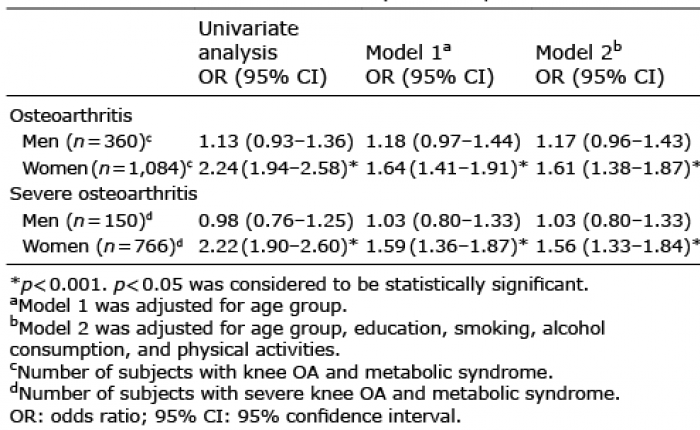 Click to show fullsize
Click to show fullsize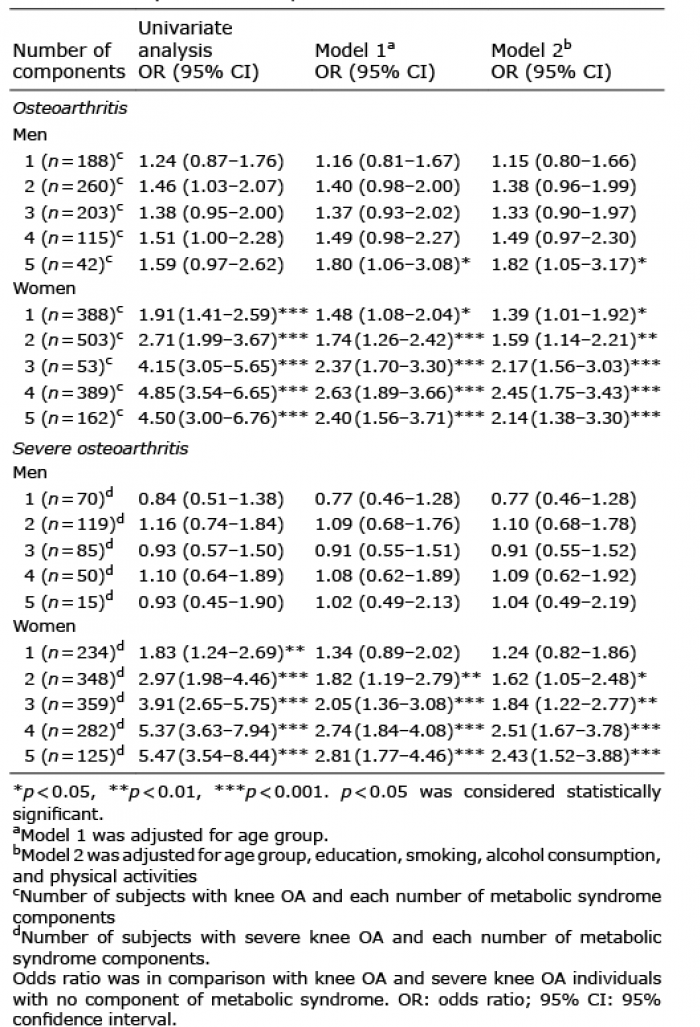 Click to show fullsize
Click to show fullsize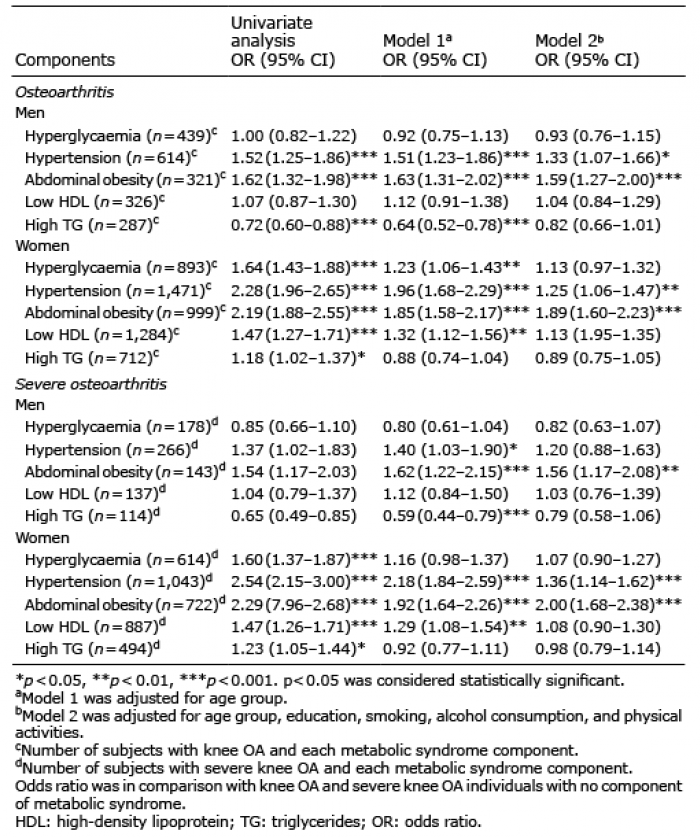 Click to show fullsize
Click to show fullsize