
From the University of Michigan Medical School, Department of Physical Medicine and Rehabilitation, Ann Arbor, MI, USA
Objective: To examine how factors associated with infection, organ failure, poor wound healing, or indices of chronic vascular disease are associated with unplanned transfers and functional gains in a population of dysvascular amputees during inpatient rehabilitation.
Design: Cross-sectional.
Setting: Inpatient rehabilitation unit at an academic medical centre.
Patients: A total of 118 patients with new, dysvascular, lower-extremity, amputation participating in inpatient rehabilitation.
Methods: Logistic regression and indices of change (minimal detectable change; MDC90), standardized response mean and effect size were used to examine the risks of unplanned transfer and functional change.
Main outcome measurements: Rate of unplanned transfers from rehabilitation, and Functional Independence Measure (FIM).
Results: Out of the total of 118 patients 19 had unplanned transfers due to medical complications. Age, creatinine, haemoglobin, white blood cell count, haemodialysis, wound vacuum device use, intravenous antibiotic use, or previous amputations were not independently associated with unplanned transfers, motor FIM change or efficiency. The MDC90 for motor FIM was 17.84, with 21.2% of patients exceeding this value; standardized response mean and effect size were large (1.03 and 1.39, respectively).
Conclusion: This study suggests that the presence of comorbidities in a population of dysvascular amputees participating in inpatient rehabilitation did not increase the risk of unplanned transfers or affect FIM gains.
Key words: amputation; inpatient rehabilitation; comorbidity, interrupted stay, healthcare quality; lower extremity amputee.
Accepted Mar 25, 2019: Epub ahead of print Apr 9, 2019
J Rehabil Med 2019; 51: 369–375
Correspondence address: Raymond Cheng, 3301 Matlock Road, Inpatient Rehabilitation Unit, 4th Floor, Arlington, TX 76015, USA. E-mail: rayscheng@gmail.com
Patients who undergo a lower extremity amputation due to poor blood flow often have multiple, long-term medical conditions that increase the risk of complications after surgery. They also tend to be in worse physical condition than the average person, even prior to amputation. After an amputation, people often participate in physical rehabilitation in a hospital to improve their strength, and to learn how to get around their homes and communities without a limb. We suspected that
chronic medical conditions related to poor blood flow and amputation would make it more difficult for
patients to participate in rehabilitation. This study of 118 patients who required lower extremity amputation due to poor blood flow found that, despite multiple medical comorbidities, these patients benefited from in-hospital rehabilitation after their surgeries as much as patients who were in rehabilitation for other reasons.
In the USA, patients are currently being admitted to inpatient rehabilitation more quickly following major surgery, and lengths of stay in acute care are decreasing. This is due to many factors, including increased scrutiny of inpatient rehabilitation facilities by payers and an increase in prospective payment structures for many surgical services that discharge patients to inpatient rehabilitation (1–3). As the medical complexity of patients admitted to inpatient rehabilitation increases, the incidence of unplanned transfers from inpatient rehabilitation units to acute medical services due to medical complications has also increased (4). Unplanned transfers negatively affect patients’ rehabilitation trajectories and increase healthcare costs, making appropriate selection and medical management of patients admitted to inpatient rehabilitation increasingly important (5). Screening patients to identify those at high risk of medical emergencies is essential to avoid unplanned transfers from inpatient rehabilitation.
Among common diagnoses seen in inpatient rehabilitation patients, dysvascular lower extremity amputee patients represent a population that is particularly vulnerable to medical complications due to the significant chronic comorbidities that often contributed to the amputation, such as diabetes. As a result, patients with lower extremity amputation are at particularly high risk of unplanned transfers from inpatient rehabilitation units compared with other diagnoses commonly admitted to inpatient rehabilitation (4, 6). Patients with dysvascular lower extremity amputation also have a higher rate of re-hospitalization, more so than other common inpatient rehabilitation diagnoses, such as spinal cord injury (SCI) (6), traumatic brain injury (TBI) (7), and stroke (8), which suggests that the comorbidities associated with dysvascular amputation are associated with increased medical complications. Unfortunately, dysvascular patients who undergo lower extremity amputation often rehabilitate at subacute rehabilitation facilities and skilled nursing facilities, where the level of medical supervision is significantly lower (9). Despite this, there is strong evidence that dysvascular amputees benefit greatly from inpatient rehabilitation in terms of functional gains and, potentially, survival (10, 11).
Across all rehabilitation diagnoses, infection is the most common complication, and dysvascular patients are at risk of this due to poor blood flow and the presence of a wound (12). The presence of peripheral vascular disease, the most common cause of amputation (13), is associated with a higher risk of interruption to rehabilitation, with Meikle et al. finding that 18% of dysvascular amputees were discharged from inpatient rehabilitation due to wound healing issues (6) The study also found that time from amputation to starting inpatient rehabilitation was a significant risk factor for complications.
Medical comorbidities may also contribute to fewer functional gains during inpatient rehabilitation. For example, lower extremity amputees receiving haemodialysis make less functional gains and have longer lengths of stay than those without end-stage renal disease (ESRD) (14). Furthermore, patients who undergo amputation due to a sarcoma, and therefore may not have significant chronic comorbidities, perform better on inpatient rehabilitation units and have shorter lengths of stay than dysvascular amputees (12). Finally, cognitive impairment, which is commonly observed in patients with severe vascular disease, has been shown to have a negative impact on inpatient rehabilitation performance of dysvascular amputees (15).
Unfortunately, while the previously-mentioned studies evaluate dysvascular amputees within the framework of 1 or a few comorbidities, these patients often have multiple significant comorbidities and many have not been evaluated in this population. While prior research by Dillingham et al. has demonstrated the impact of medical and social factors on determining the post-acute care discharge destination following dysvascular lower limb amputations, there has been limited research into how specific medical comorbidities affect the rate of unplanned transfers from inpatient rehabilitation for this patient population (16). Furthermore, Sauter et al. found that patients who undergo dysvascular lower limb amputations have significantly improved functional outcomes from receiving rehabilitation at an inpatient rehabilitation facility compared with a skilled nursing facility, probably due to their high medical complexity and increased risk of medical complications, which necessitate closer medical monitoring (17).
The primary objective of this study was to examine whether certain indicators of medical comorbidities, available at the time of admission to inpatient rehabilitation, were associated with an increased risk of unplanned transfers from inpatient rehabilitation among patients with amputation due to vascular disease. Specifically, the study focused on factors associated with infection, poor wound healing, organ failure, and/or previous amputations that were commonly available at the time of admission to inpatient rehabilitation. No previous study has evaluated indicators of infection risk, such as the presence of wound vacuums, ESRD, or diagnoses that confound vascular disease, such as diabetes, as they relate to the risk of unplanned transfers from inpatient rehabilitation in dysvascular amputee patients. The secondary objective was to examine whether the aforementioned factors were associated with decreased functional gains during inpatient rehabilitation. A greater understanding of these risk factors can help identify patients at greater risk of severe medical complication, which could allow for the reduction in unplanned discharges by identifying specific comorbidities that might require more proactive management, or situations that may warrant a delay in admission to rehabilitation in order for medical stability to be firmly established prior to transfer.
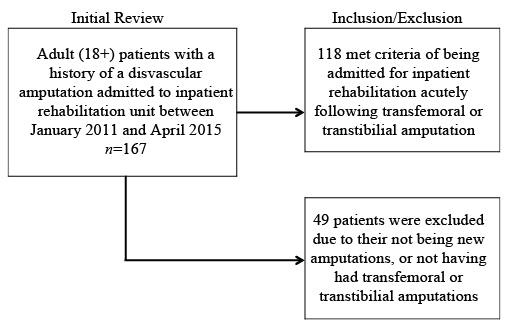
Using a cross-sectional, retrospective design, data were collected from electronic medical records of patients who received inpatient rehabilitation in an academic tertiary rehabilitation centre. Ethics approval for a waiver of informed consent was obtained before initiation of the study from the University of Michigan, Medical School Institutional Review Board. Data were collected from consecutive patients over the age of 18 years who were admitted to the acute inpatient rehabilitation unit from January 2011 to April 2015 following new transfemoral or transtibial amputation(s) due to sequelae of chronic vascular disease. Patients with previous amputations were included in the sample if they were undergoing a new, contralateral amputation. Patients were excluded from the sample if they had missing or incomplete data, were admitted for partial foot or toe amputations, or if their rehabilitation stay followed hospitalization for a reason other than amputation. In total, 49 patients were excluded, primarily because their admission to inpatient rehabilitation was not due to a new amputation. Only 3 patients were excluded due to having had foot or toe amputations, compared with above/below knee amputations (Fig. 1).
Fig. 1. Inclusion and exclusion criteria.
The primary outcome of this study was the incidence of transfer from inpatient rehabilitation to an acute care medical service due to a medical complication. The secondary outcome was func-tional gains during the inpatient rehabilitation stay. Functional outcomes were measured using the Functional Independence Measure (FIM). Specifically, total gain in motor FIM (admission – discharge motor FIM score) and motor FIM efficiency (total motor FIM change divided by the number of days in inpatient rehabilitation) were evaluated.
The primary predictors of interest were the presence of infection at admission assessed by elevated white blood cell count and active treatment with intravenous (IV) antibiotics. Other factors associated with poor wound healing, such as diabetes or the need for negative pressure wound therapy (hereafter referred to as “wound vac”), were also expected to indicate an increased vulnerability to infections and possibly to be associated with increased incidence of unplanned transfers from inpatient rehabilitation. Markers of organ failure, represented by elevated creatinine levels at admission, anaemia, and pre-admission need for haemodialysis, were expected to correlate with increased incidence of transfer. History of previous amputation was also thought to be associated with higher rates of acute transfer, as it could reflect more severe systemic disease. In our evaluation of laboratory tests, the most recent results within 72 h prior to admission to the inpatient rehabilitation unit were evaluated; if there was no laboratory data available in that window of time, the first available laboratory values in the 48 h following admission were recorded. Finally, length of stay, gender, age at inpatient rehabilitation admission, number of days since amputation, and admission FIM scores (total and motor FIM) were controlled for in the analysis.
Binary logistic regression was used to test the impact of factors on the likelihood that patients would have an unplanned transfer from the inpatient rehabilitation unit. Hierarchical multiple regression was used to assess the ability of infection, poor wound healing, organ failure, and chronic vascular disease to predict gains in function during inpatient rehabilitation. Preliminary analyses were conducted to ensure no violation of the assumptions of normality, linearity, multicollinearity, and homoscedasticity. Linearity of the continuous variables with respect to the logit of the dependent variable (unplanned transfer) was assessed via the Box-Tidwell procedure (18). A Bonferroni correction was applied using all terms in the model resulting in statistical significance level of p < 0.00625. Based on this assessment, all continuous independent variables were found to be linearly related to the logit of the dependent variable. There were 4 cases of studentized residuals with values greater than 3.00 standard deviations (SD), which were kept in the analysis.
Because of interest in the potential functional benefits of a full course of inpatient rehabilitation, patients with unplanned transfers were excluded from the analysis of functional gains. In addition to examining the relationship of medical variables and functional gains, 3 indices of change for total and motor FIM scores (i.e. gain scores) were evaluated: minimal detect-able change (MDC); Cohen’s effect size; and the standardized response mean (SRM). The MDC is a statistical measure of change, defined as the minimum amount of change that exceeds measurement error. In other words, the smallest change that is due to “true” change and not variation in measurement (14). The intraclass coefficients (ICC) for total and motor FIM gain scores, within each group, were used to calculate the standard error of measurement (SEM) and MDC at the 90% confidence level (MDC90) using the following formula: 1.64*SEM*. The percentage of patients whose total and motor FIM gain scores exceeded the MDC90 using the χ2 test of homogeneity were also examined. Cohen’s effect size quantifies the size of the difference between baseline and follow up (i.e. admission and discharge) and estimates the magnitude of treatment effect; in this case, inpatient rehabilitation. Within-group effect size as admission to discharge difference divided by the admission score SD was also calculated. Similar to effect size, SRM attempts to quantify the effect of the treatment, or inpatient rehabilitation. It is preferred to paired t-test because it removes the dependence on sample sizes (19). The model contained 12 independent variables: white blood cell count (WBC, value), use of IV antibiotics (no/yes), creatinine (value), haemodialysis status at admission (no/yes), wound vac presence at admission (no/yes), history of diabetes treated with insulin and/or medication (no/yes), haemoglobin (value), history of a previous amputation (no/yes), length of stay on the rehabilitation unit (days), gender (male/female), time between amputation and admission to the acute inpatient rehabilitation unit (days), and motor FIM at admission (value). These variables were selected due to their correlation with chronic disease, risk of infection, and/or risk of poor wound healing. The same predictive model was used for all regression testing with the exception of length of stay for motor FIM efficiency, as this is used in the calculation of the outcome. Model variables were entered in a step-wise fashion, beginning with factors expected to have the most explanatory power, to observe the degree of change in the amount of variance in the outcome each step contributed. All analyses were conducted in IBM SPSS version 23, Armonk, NY, USA.
The sample was primarily male (82, 70.1%), Caucasian (84, 75.7%), with a mean age of 60.8 years (standard deviation (SD) 12.9). The patients had a mean of 10.9 days (SD 10.5) between amputation and admission to acute rehabilitation with a mean length of stay of 14.1 days (SD 7.1). Descriptives of study variables are given in Table I. In general, the sample reflected the medical complexity of the dysvascular amputee population. The mean creatinine value of the sample was above the upper limit of normal (SD 1.3 mg/dl), and the mean haemoglobin was below the lower limit of normal (SD 12.6 g/dl); 22% were being treated with IV antibiotics at the time of admission to the inpatient rehabilitation unit. Ten percent of the sample had incisions requiring wound vac, and 11% were on haemodialysis at the time of admission to the inpatient rehabilitation unit.
Table I. Descriptives of study variables
Of the 118 patients, 19 (16.1%) required an unplanned transfer from inpatient rehabilitation, with the most common causes for transfer being infection, hypoxia and renal failure (see Table II). The full model containing all predictors was not statistically significant, χ2 (13, n = 111) = 19.01, p = 0.12, indicating that the model was not able to distinguish between those who did and did not have an unplanned transfer from inpatient rehabilitation. The model explained between 15.7% (Cox and Snell R square) and 29.6% (Nagelkerke R-squared) of the variance in unplanned transfers and correctly classified 88.3% of cases. As shown in Table III, only gender made a unique and statistically significant contribution to the model.
Table II. Primary reasons for unplanned discharge from rehabilitation unit
Table III. Logistic regression predicting likelihood of unplanned transfer from inpatient rehabilitation
Controlling variables of days since amputation, age, admission motor FIM, and days in inpatient rehabilitation (for discharge motor FIM only) were entered in Step 1, explaining 0.9% of the variance in FIM efficiency, F (3, 93 = 0.29), p = 0.83. After entry of infection factors (WBC, presence of IV antibiotics) in Step 2, the total variance explained was only 6.7%, F (5, 91) = 1.31, p = 0.26). After entry of poor wound healing factors (creatinine, on haemodialysis, and on wound vac) in Step 3, the total variance explained gained only a nominal amount, with 7.0%, F (8, 88) = 0.82, p = 0.56. After entry of organ failure factors (diabetes, haemoglobin value) in Step 4, there was no gain in variance explanation with 7.0%, F (10, 86) = 0.65, p = 0.77. In the final model adding previous amputation, shown in Table III, only 7.2% of the variance was explained, F (11, 85) = 0.60, p = 0.82. Using the same model variables and steps (with the addition of days on inpatient rehabilitation in Step 1), results were similar for motor FIM gain with no predictor variable having a significant association with the outcome. In the final model, shown in Table IV, 14.3% of the variance was explained, F (11, 96)v1.08, p = 0.38.
Table IV. Hierarchical multiple regression (final model) predicting motor Functional Independence Measure (FIM) gain
At the time of discharge, 24 (21.2%) patients exceeded the MDC90 value of 17.84 for FIM motor gain. The MDC90 value indicates that there is a 90% confidence that change in motor FIM greater than 17.84 is not due to measurement error. The effect size was large (1.03), as was the SRM value (1.39), using Cohen’s criteria (19).
This is the first study to evaluate factors potentially associated with interruptions to rehabilitation. In this study, 16.2% of dysvascular patients participating in inpatient rehabilitation due to a lower extremity amputation required an unplanned transfer from the rehabilitation unit. This is consistent with the rate of unplanned transfers found in previous studies of amputee patients, which ranged from 6.6% to 22.8% (6, 20). Model testing indicated that renal function, use of IV antibiotics on admission, history of diabetes, history of previous contralateral amputation, presence of a wound vac, and age were not associated with an increased risk of an unplanned transfer from inpatient rehabilitation. Together, these factors explained a relatively modest amount of the variance, suggesting that other factors may better predict unplanned transfers. The only factor significantly associated with unplanned transfers was gender, with an increased incidence of unplanned transfers in women compared with men, which is also consistent with the findings of a previous study by Meikle et al. (6) Other factors, such as a shorter span of time between amputation and inpatient rehabilitation admission, and other markers of peripheral vascular disease were also not statistically significantly associated with the incidence of unplanned transfers in our study. Although older age also did not appear to increase the risk of transfer in our study, other studies have found evidence that older patients have a higher rate of transfer from acute rehabilitation to acute care across all rehabilitation diagnoses (12).
The analysis of our results also found that none of the factors examined were significantly associated with functional outcomes in terms of FIM efficiency in this limited sample. No definitive conclusions can be drawn from these results due to the limited scope and sample size of this study; however, our findings would be consistent with the idea that comorbidities associated with dysvascular amputations do not increase the risk of unplanned transfers from inpatient rehabilitation, nor do they limit functional gains during rehabilitation. This may be influenced by the increased level of medical supervision during inpatient rehabilitation, which allows for the prevention of many major medical complications, and is consistent with previous research showing the overall benefits of inpatient rehabilitation over subacute rehabilitation in this population (17, 21). Finally, only approximately one-fifth of patients exceeded a FIM motor gain of 17.84, or the threshold of change not due to measurement error. This suggested modest actual gains in motor function for the sample.
This study has several limitations that should be considered when interpreting the results. First, the sample was drawn from a single inpatient rehabilitation facility in a single health system and therefore the generalizability of these results is limited. Studies of amputee patients in different health systems and across different demographics are needed to show whether these outcomes are consistent for the amputee population at large, though the non-novel aspects of our results are consistent with previous studies (e.g. female gender as a risk factor for unplanned transfer).
Furthermore, our sample did exclude certain dysvascular amputee patients, which should be taken into account when interpreting the results. We did not include patients who initially went home after amputation or patients who were admitted months after amputation for the purpose of prosthetic training, because we felt they represented patients who were significantly more medically stable and less prone to complications than those admitted to inpatient rehabilitation immediately following amputation. Also, a small proportion of patients were transferred and re-admitted to inpatient rehabilitation several times. In these cases, only the patient’s first rehabilitation admission was analysed, as the goal of this study was to identify factors that could predict a patient’s likelihood of a major medical complication necessitating acute transfer, before the patient is identified as being at high risk of decompensation.
In addition, this study examined each risk factor for unplanned transfer or FIM gains independently and does not does not account for the aggregate effect of multiple comorbidities. Thus, the results do not account for the possibility that multiple comorbidities may have an additive effect, greater than the sum of each individual comorbidity. Another limitation is that the data for our regression models analysing motor FIM and FIM efficiency are limited to patients who completed rehabilitation, and did not include patients who developed medical complications necessitating transfer to an acute medical service. Furthermore, it is notable that clinical change indices suggested that only 20% of the sample exceeded motor FIM gains that were unlikely due to measurement error, although effect sizes were quite large. One explanation is that much of the benefit of inpatient rehabilitation for post-amputation patients is from complication avoidance and patient education, and that FIM, as a gross measure of function, may not fully capture the medical benefits of inpatient rehabilitation for patients with amputations. For example, many lower extremity amputees are discharged at a wheelchair level, which significantly lowers their motor FIM score potential. However, FIM has been used as the primary outcome measure in other research and is the current standard for evaluating inpatient rehabilitation performance of lower extremity amputees (14). For future studies, measures such as self-reported perception of functional independence, such as the SF-36 or Katz ADL disability tools, may be considered as additional ways to measure any benefits achieved in this patient population (16, 17).
Taken together, these results suggest that patients undergoing lower extremity amputation due to vascular disease benefit from inpatient rehabilitation despite the multiple comorbidities that are commonly associated with this population. This study supports the notion that dysvascular amputee patients should be considered for inpatient rehabilitation despite having high levels of medical complexity. This is especially true given the increased risk of harm or decompensation that may result from a lower level of care. Further research is needed to determine how comorbidities in dysvascular patients may affect the extent of functional gains in inpatient rehabilitation, and larger sample sizes would be needed to judge the reproducibility and generalizability of our findings across a wider range of patients.
Funding to partially support this study was received from the University of Michigan Health System-Ann Arbor Center for Independent Living Advanced Rehabilitation Research Training Program, US Department of Education, National Institute of Disability and Rehabilitation Research (H133P090008).


 Click to show fullsize
Click to show fullsize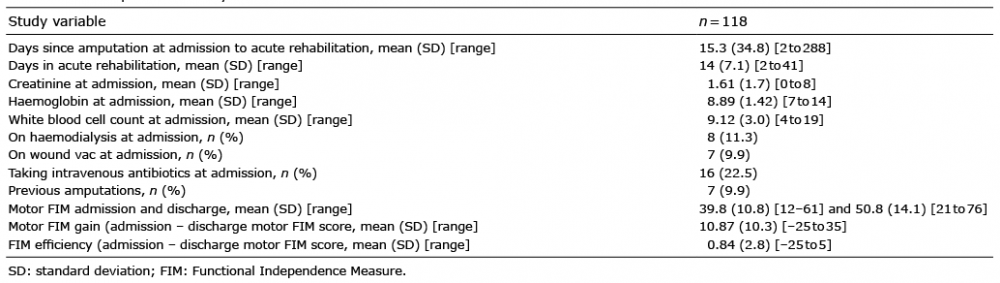 Click to show fullsize
Click to show fullsize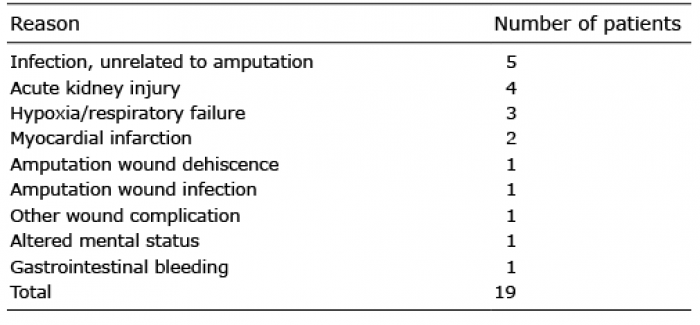 Click to show fullsize
Click to show fullsize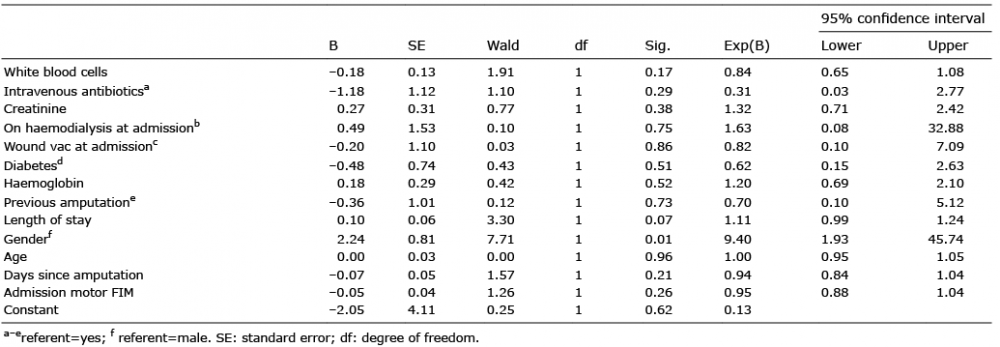 Click to show fullsize
Click to show fullsize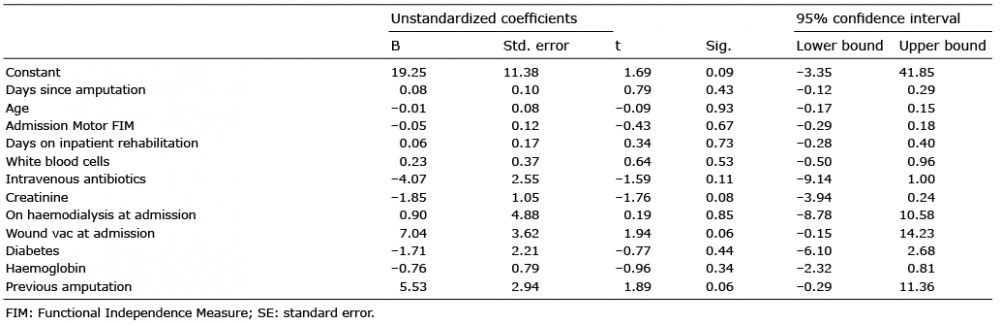 Click to show fullsize
Click to show fullsize