
From the 1Discipline of Occupational Therapy, Faculty of Health Sciences, The University of Sydney, 2Graythwaite Rehabilitation Centre Ryde Hospital, 3Susan Wakil School of Nursing and Midwifery (Sydney Nursing School), The University of Sydney, 4The StrokeEd Collaboration, and 5Graduate School of Health, University of Technology Sydney, 6Discipline of Speech Pathology, Faculty of Health Sciences, The University of Sydney, Sydney, Australia
Background: Although stroke has a profound impact on sexuality there are limited evidence-based interventions to support rehabilitation professionals in this area. The aim of the current research was to prioritize content areas and approaches to sexual rehabilitation from the perspective of stroke survivors, their partners, stroke rehabilitation clinicians and researchers.
Methods: A 2-step online Delphi method was used to prioritize the content of, and approaches to, sexual rehabilitation with stroke survivors, their partners, stroke rehabilitation clinicians and researchers.
Results: Stroke survivors (n = 30), their partners (n = 18), clinicians and researchers in stroke rehabilitation (n = 45) completed at least 1 of 2 investigator-developed surveys. Participants prioritized 18 core content areas for inclusion in sexual rehabilitation following stroke with a high degree of consensus. Another 27 content areas were considered moderately important. There was strong consensus that sexual rehabilitation should be offered in the subacute and chronic phases of stroke recovery. Participants would prefer health professionals to deliver the intervention face-to-face.
Conclusion: This study presents opinions from stroke survivors, partners of stroke survivors, clinicians and researchers. The information about content, timing and mode of delivery will be used to develop and evaluate a comprehensive sexuality rehabilitation programme.
Key words: Delphi-technique; sexuality; sexual behaviours; stroke; rehabilitation.
Accepted Mar 12; Epub ahead of print Mar 21, 2019
J Rehabil Med 2019; 51: 352–360
Correspondence address: Margaret McGrath, Cumberland Campus C42, The University of Sydney, PO Box 170, Lidcombe, NSW 1825 Australia. E-mail: Margaret.mcgrath@sydney.edu.au
Although stroke often impacts on sexuality there are very limited programmes to provide sexual rehabilitation for stroke survivors or their partners. We asked stroke survivors, partners of stroke survivors, rehabilitation professionals and clinicians to identify what should be included in a sexual rehabilitation programme for stroke survivors, when this programme should be offered, what professionals should be involved in delivering the programme, and how they should provide the programme. The participants completed 2 online surveys and prioritized 18 core topics to be included in sexual rehabilitation following stroke. There was strong consensus among participants that sexual rehabilitation should be offered in person once the stroke survivor was medically stabilized and throughout rehabilitation. These results will be used to design an intervention to address sexuality after stroke.
Stroke has a profound impact on the ways in which sexuality is experienced and expressed by stroke survivors and their partners. A recent thematic synthesis found that, while sexuality is largely silenced by stroke, it nonetheless remains important to stroke survivors and their partners (1). International clinical guidelines for stroke rehabilitation propose that sexuality should be included as a core component of comprehensive rehabilitation (2–4). However, research consistently shows that health professionals rarely address sexuality during stroke rehabilitation (5–7). For stroke survivors and their partners, failure to address sexuality may result in increased anxiety and depression and poorer quality of life outcomes (8–11).
Sexual rehabilitation is effective for people undergoing cancer rehabilitation (12, 13), cardiac rehabilitation (14) and those living with spinal cord injury (15). However, evidence to support sexual rehabilitation following stroke is less well developed. Only 2 studies have reported interventions to address sexuality after stroke. In South Korea, Song and colleagues (16) developed a 32-page manual, which they used in conjunction with a pre-discharge, nurse-led information session addressing: (i) the impact of stroke on sexual function; (ii) fear of post-stroke sexual activity; (iii) strategies to reduce sexual dysfunction; and (iv) questions and concerns. A similar programme was delivered in Australia by Sansom and colleagues (17, 18) based on the intervention by Song and colleagues (16) and involving a 30-min consultation by a rehabilitation physician. While these programmes offer a starting point for professionals interested in sexual rehabilitation, both programmes placed a strong emphasis on sexual activity as the primary outcome of interest, rather than including broader dimensions of sexuality found to be important to stroke survivors (1). Furthermore, the efficacy of any sexuality intervention for stroke survivors and their partners remains largely unexplored. This lack of research into sexual rehabilitation hinders the ability of health professionals to provide evidence-based care and highlights the need to develop a more comprehensive sexual rehabilitation intervention for stroke survivors and their partners. The aim of the current research was to prioritize content areas and approaches to sexual rehabilitation from the perspective of stroke survivors, their partners, stroke rehabilitation clinicians and researchers.
Recommendations outlined in the guidance on conducting and reporting DELPHI studies (CREDES) were followed (19). A modified Delphi methodology (20) was used to elicit and prioritize content for inclusion in post-stroke sexual rehabilitation, methods and timing of intervention delivery, and disciplines that should be involved. Delphi methods identify and use diverse groups of experts and a systematic approach to ascertain priorities, and achieve consensus on these priorities with relevant stakeholders (21, 22). Typically, Delphi methods are used where there is a knowledge gap. There is lack of consensus about the number of rounds of data collection needed for Delphi studies, but recognition that multiple rounds can result in respondent fatigue and increase attrition rates (20). We chose to complete a 2-round approach, balancing the need to retain key elements of the Delphi process without overburdening participants.
There is a dearth of evidence supporting provision of sexual rehabilitation services following stroke, particularly in relation to user-driven content. Contemporary implementation science increasingly recommends involving knowledge users (clinicians, managers, policymakers, patients/families and others) in the early design and development of interventions, for a faster and larger impact (23). Delphi methodology enabled stroke survivors, their partners, rehabilitation clinicians and researchers to contribute to the development of sexual rehabilitation interventions.
Four separate groups of stakeholders were targeted during recruitment: stroke survivors; their partners; rehabilitation clinicians; and researchers working in the fields of sexuality, disability and neuro-rehabilitation. Ethical approval for the study was granted by the research ethics committee at the University of Sydney (2017/079). All participants were provided with written information and study aims and invited to participate in 2 online surveys.
Stroke survivors and their partners. Participants were recruited through consumer organizations that represent stroke survivors in Australia, and through our own professional networks. Diverse representation was sought, including people living in rural and urban settings and with a variety of sexual orientations. Potential participants were eligible if they met the following criteria: (i) had received, or were a current or former partner of a stroke survivor who had received stroke rehabilitation services in Australia; (ii) were willing and able to participate in an online survey regarding sexuality and stroke (with or without communication support provided by a speech pathologist); and (iii) were able to communicate in English (with or without communication support provided by a speech pathologist).
Stroke survivors with self-reported communication difficulties (aphasia, apraxia, dysarthria, cognitive-communication disorder) were specifically targeted for inclusion in the study. Participants either indicated their interest by email or through referring family and clinicians. Participants with self-reported communication difficulties were offered an aphasia-friendly (24) participant information sheet, and either a phone call or in-person discussion about the study. Our aim in providing support was for people with self-reported communication difficulties to understand the consent process and written survey as much as possible. Where required, communication was facilitated with Principles of Supported Conversation for Adults with Aphasia (SCATM) (25) by an experienced speech pathologist (EP) with training in SCATM. To be eligible for inclusion, participants needed to accurately answer 4 yes/no questions about the study, based on information provided by the speech pathologist. If they consented, participants were then offered the opportunity to complete an unmodified online form (with or without support), or a face-to-face session with a speech pathologist using an aphasia-friendly version of the Delphi survey, accompanied by SCATM techniques. Based on the initial meeting, the speech pathologist rated participants’ communication activity limitation, using the Australian Therapy Outcome Measures (AusTOMs) Activity Limitation Scale (26) most pertinent to their reported communication difficulties (typically language).
Rehabilitation clinicians. Rehabilitation clinicians were contacted by email via rehabilitation networks. Clinicians were eligible to participate if they provided clinical care to stroke survivors. The importance of having respondents from as many rehabilitation disciplines as possible was highlighted. Additional emails were sent to discipline-specific networks to recruit participants from speech pathology, sexology and sexual counselling backgrounds.
Researchers. Three electronic databases (MEDLINE, CINAHL, PsycINFO) were searched to identify authors who had published peer-reviewed articles about sexual rehabilitation following acquired physical disability. We contacted theses authors by e-mail and invited participation in the study.
All surveys are available from the authors. Demographic data were collected to describe participants. In the first round information about age, gender, cultural background, sexual orientation, religious beliefs, stakeholder group, number of years post-stroke and professional background was sought.
Round 1. The first round sought participants’ views on the desired content of a post-stroke sexual rehabilitation programme, timing of the programme, preferred method of programme delivery and involvement of specific disciplines in the programme.
Participants were initially presented with a short statement describing potential content areas (n = 47) grouped into 6 categories: (i) general issues relating to sexuality and disability (n = 4); (ii) communication issues (n = 7); (iii) stroke-related cognitive and behavioural changes impacting on sexuality (n = 5); (iv) stroke-related psychological changes impacting on sexuality (n = 8); (v) stroke-related changes in physical function impacting upon sexuality (n = 9); and (vi) changes in sexual function (n =14). Potential content was generated from 3 sources. First, we completed a systematic review and meta-synthesis of qualitative research regarding experiences of stroke survivors and their partners in relation to post-stroke sexuality (1). Secondly, a content review of existing sexual rehabilitation programmes for adults following acquired disability was completed. Thirdly, we examined the curricula of published interventions, which addressed sexuality after stroke (16–18). A list of potential content was then organized into the 6 broad categories listed above and presented to participants in the first Delphi survey.
For the first Delphi survey, participants were initially asked to rate the value of each content area in relation to sexual rehabilitation programmes, using a 5-point-Likert scale. Secondly, participants were asked to identify and rank the 10 content areas they deemed to be most important for inclusion in a sexual rehabilitation programme, from 1 (highest) to 10 (lowest) in importance. Next, participants were asked to propose additional content not covered in the survey, responding to an open-ended question. The same process was completed for timing of a sexual rehabilitation programme, method of programme delivery and involvement of specific disciplines.
For participants with self-reported communication difficulties, the aphasia-friendly version was modified using aphasia-friendly principles (24) with pictographic support, simplified language, bolding and larger font. Pictographic supports for sexuality were used with permission from the Aphasia Institute Canada (27). Three participants required the modified version, with the remainder (n = 5) completing the online survey with support from the speech pathologist as required. The online survey was formatted so that participants could return and complete it later; some people with mild self-reported communication difficulties reported that this was helpful, as they could complete the survey more slowly with breaks.
Round 2. In round 2, participants were presented with content areas from round 1, along with a summary of responses obtained from round 1. Participants were asked to rate the importance of each content area, preferred methods of delivery, timing of delivery and discipline using the same 5-point Likert scale. Finally, participants were asked to reflect on results from round 1 and provide feedback on aggregated responses via a series of open-ended questions.
Analysis was conducted for the overall sample. Descriptive statistics were used to calculate responses about content area, timing, methods and disciplines that the overall group deemed most important. For each content area, the mean importance score, the 25th and 75th percentile and interquartile range were calculated. To determine the degree of consensus around the importance score, a score was calculated for each content area by dividing the interquartile range by 2. Following guidelines proposed by Burnette and colleagues (28), a consensus score of < 1 indicated high consensus, a score of 1 indicated moderate consensus, and a score > 1 indicated low consensus.
Two approaches were used to identify the content areas, timing, methods and disciplines deemed of highest importance by respondents. Firstly, we considered the mean priority score given to each content area. Scores ≤ 2.4 were categorized as low priority, scores ≥ 2.41 and scores ≤ 2.8 as intermediate priority, and scores ≥ 2.81 categorized as high priority. Secondly, the percentage of respondents who included a content area in their top 10 priorities was calculated. After reviewing the spread of scores, categories were assigned as follows: > 25% = high priority, 15–25% = intermediate priority, and < 15% = low priority.
Finally, the 2 priority ratings (mean priority score and percentage of respondents including the content area in their top 10 priorities) were synthesized into 1 priority code with 3 tiers. Tier 1 content, timing, delivery methods and disciplines were rated as either: (i) high by both rating schemes; or (ii) high by one rating scheme and intermediate by the second rating scheme. Tier 2 content were rated as either: (i) intermediate by both rating schemes or (ii) high by one rating scheme and low by the second rating scheme. Tier 3 content areas were rated as either: (i) low by both rating schemes or (ii) low by one rating scheme and intermediate by the second rating scheme. For example, the statement “Resuming sexual activity after stroke”’ had a mean priority score of 3.51 (high priority), with 57.4% of respondents identifying the statement as a top 10 priority area (> 25%, high priority), thus was included as a tier 1 content area. On the other hand, the statement “What is sexuality?” had a mean priority score of 3.57 (high priority) with 9.6% of respondents identifying the content area as a top 10 priority area (low priority), and thus was included as a tier 2 statement. A summary matrix was compiled to display the content, timing, delivery methods and disciplines according to consensus and priority. See supplemental Tables SI1, SII1, SIII1 and SIV1 for full information.
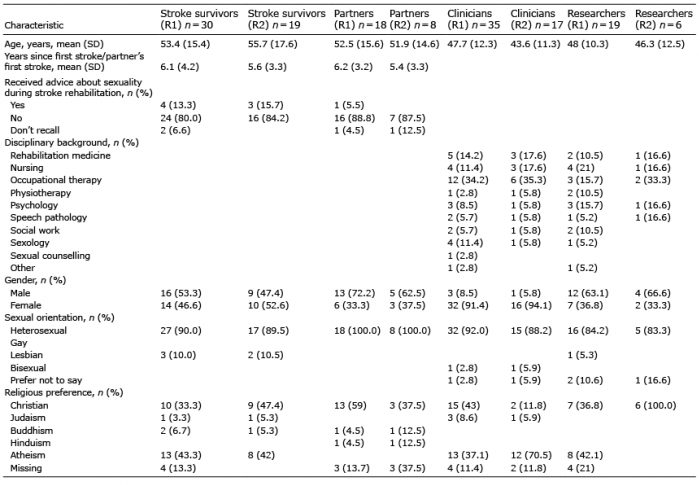
The final sample size and characteristics are presented in Table I. Of the 102 participants who completed the first survey, 49% (n = 50) completed the second survey. For participants with self-reported communication difficulties (n = 8), 1 person (male) had a mild activity limitation on the AusTOMS (26) cognitive-communication scale, 3 people (2 females and 1 male) had mild receptive and expressive language limitation on the AusTOMS language scale (26), and all elected to complete the online survey. One participant (female) had a moderate expressive language limitation, a mild receptive language limitation, and completed the online survey. Another participant (male) had moderate expressive and receptive language limitations and chose to complete the aphasia-friendly survey. Finally, 2 male participants had moderate/severe language and speech limitations (apraxia) and completed the aphasia-friendly version with supported communication. Due to time constraints associated with data collection the 3 participants who completed the aphasia-friendly version of the survey were unable to participate in the second round of data collection.
Table I. Participants’ characteristics
During round 1, participants were presented with 47 potential content areas for inclusion in sexual rehabilitation following stroke. No further content was identified through open-ended questions in rounds 1 or 2. Table SI1 shows the final 47 content areas, with consensus scores and both priority scores. Table II presents the final 47 questions in a matrix categorized by consensus and priority tier. None of the original 47 content areas were excluded by participants. Eighteen content areas were identified as being of high priority with a high level of consensus. A further 27 content areas were identified as having intermediate priority, again with a high level of consensus. One content area “What is sexuality?” was given a low priority with moderate level of consensus, while the content area “Why is it important to talk about sexuality?” was given an intermediate priority with high consensus. Analysis of responses between rounds 1 and 2 indicated no changes in priority or consensus relating to content areas.
Analysis of responses to open-ended questions indicated that stroke survivors and partners were conscious of the individual nature of sexuality and the stroke recovery experience, and thus, were reluctant to exclude content areas based on their own personal experience:
‘I feel these would be relevant to all stroke survivors and the partners. Additional information should be chosen on an individual basis depending on the personal situation’ and
‘I have no physical problems and my partner’s very supportive therefore I have many neutral answers. I could expect that there are many others have real problems.’
Clinicians and researchers had similar concerns, noting that discriminating between content areas was often difficult, with practice typically led by the needs of individual stroke survivors and their partner.
‘All are extremely relevant, and each has a specific function regarding one’s sexuality and disability and their approach with this as an individual and as a couple.’
Clinicians and researchers tended to rank content related to psychological, cognitive and behavioural changes after stroke higher because in their experience, professionals were more able to respond to sexual problems caused by stroke-related physical impairments:
‘I have focused more on the social and psychological aspects for suggested topics as, in my experience, doctors and allied health are already reasonably comfortable in discussing changes to physical functioning related to sexuality following stroke.’
Similarly, some respondents suggested that focusing on communication about sexuality following stroke could be a useful starting point as this would support stroke survivors and their partners to identify other areas of concern:
‘Topics that encourage the discussion and therefore problem solving around this topic is the starting point to further explore this area. If the patient’s and partners feel it is ok to talk about this subject then it allows open discussion.’
Table II. Matrix of consensus and priority scores for topics to be included in post-stroke sexual rehabilitation programme
Participants did not exclude any of the timings suggested during round 1, nor did they identify any additional times when sexual rehabilitation would be most preferable. Table SII1 shows the 6 potential timings with consensus score and both priority scores. Table III shows the potential options in a matrix, categorized by consensus and priority tier. Analysis of open-ended responses indicated that a single time-point was not considered optimal for the delivery of sexual rehabilitation following stroke. This finding was attributed to the idiosyncratic nature of stroke recovery and the likelihood that sexuality would have different meanings and different levels of relevance for individual stroke survivors.
‘It affects different people at different points in time. It would need to be when they are mentally ready to approach that topic, when they have sorted out the ‘back to normal’ out of the hospital situation. Personally, I believe six months post would be the right initial timing, but could be shorter at three months.’
Nonetheless, participants indicated high levels of consensus in prioritising delivery of services between 3 months to 1 year after stroke, reflected by comments such as:
‘I was ready to receive education re [sic] sex around the 2 to 3-month mark. Before that, I was more focused on other changes (i.e. communication, movement)’, and
‘I think the topic should be broached before hospital discharge so that people have an opportunity to consider and ask about sexuality while they still have the input of an MDT, and again after discharge, when people have had time to consider their priorities. For people with long-term stroke impairments, it would be important to revisit the topic of sexuality again, after about a year, when priorities may have changed and people have had time to try different approaches and identify what is/is not working for them.’
Although participants did not identify any time during the stroke recovery journey when sexual rehabilitation was not relevant, all 4 stakeholder groups noted that stroke survivors during the acute phase of recovery are often overwhelmed with information. The acute phase may therefore not be the best time to address sexuality.
‘In the first few weeks post-stroke clients are provided with too much information and many become very overwhelmed. Perhaps information given (very brief) at this early stage would be useful; however, it should be followed up at a later date.’
Table III. Matrix of consensus and priority scores for timing of sexual rehabilitation following stroke
Participants did not exclude any of the potential methods of service delivery offered in round 1. Table SIII1 shows the 9 potential methods of delivering sexual rehabilitation, with consensus and priority scores. Table IV shows the final 9 options in a matrix, categorized by consensus and priority. Analysis of responses to open-ended questions suggested that individual face-to-face consultation was preferred, due to the personal and potentially sensitive nature of the content.
‘This topic is deeply personal and the people are very vulnerable. Often it is too overwhelming and personal to discuss in groups although this may be effective later; therefore, one-to-one is a much more person-centred, sensitive and culturally appropriate approach.’
Furthermore, while participants valued the use of peer-to-peer counselling, they had concerns regarding the skills and training needed to ensure safe effective counselling.
‘Peer counselling could be useful however it could be a disaster depending on the ‘peer’.’
Table IV. Matrix of consensus and priority scores for modes of delivery of sexual rehabilitation following stroke
Participants did not exclude any professional group from providing sexual rehabilitation following stroke. Table SIV1 shows the 11 potential professionals presented in round 1, with their consensus and priority scores. Table V shows the final 11 options in a matrix, categorized by consensus and priority. Rehabilitation physicians, nurses with specialist knowledge in stroke and sexuality, psychologists, sexologist/sex educators/counsellors, nurses working in stroke services (acute care or rehabilitation), physiotherapists and occupational therapists were all prioritized as the preferred professionals to address sexuality, with a high level of consensus. There was a moderate level of consensus for prioritising social workers and speech pathologists.
Analysis of responses to open-ended questions indicated that stroke survivors and their partners did not have a strong preference for any specific profession to provide sexual rehabilitation. Instead, they suggested that factors, such as the age, gender and comfort of a professional when discussing sexuality should be considered:
‘Difficult to talk to female professionals about this and most of the male professionals are older than me. Need someone who is young and male.’
Participants with self-reported communication difficulties commented on the value of having a speech pathologist available to support discussions with partners and other health professionals:
‘I need people to help me (in having conversations)’ and ‘Our experience is that the medical fraternity are woefully ignorant of aphasia, its effects and its treatment, and do not take the time or care to understand the patient’s needs.’
Table V. Matrix of consensus and priority scores for preferred professionals to provide sexual rehabilitation following stroke
This study used a modified Delphi technique to determine whether agreement could be reached on the essential components of sexual rehabilitation following stroke. Specifically, we sought to identify what content should be addressed, at what point in the stroke recovery journey, and which professional group should deliver interventions, using what
method. There was a high level of consensus that all 18 core content areas should be included in post-stroke sexual rehabilitation. Participants also identified a clear preference for sexual rehabilitation services to commence during the sub-acute phases of stroke recovery and to be available across the chronic stages of stroke recovery. Participants prioritized individual face-to-face services, as well as services delivered online by professionals, reading material or peer-to-peer counseling. Rehabilitation physicians, nurses with specialist knowledge in stroke and sexuality, psychologists, sexologists/sex educators/counsellors, nurses and physiotherapists were all prioritized as the preferred professionals to address sexuality, with a high level of consensus. There was a moderate level of consensus for prioritising occupational therapists, social workers and speech pathologists. The inclusion of consumer perspectives when designing healthcare interventions is widely accepted and likely to increase the quality, relevance and acceptability of interventions (29, 30). A strength of our research is the inclusion of people with self-reported communication difficulties as part of the consumer panel, a group that are typically excluded from sexuality (1) and stroke rehabilitation research (31).
Previous studies outlining interventions to address sexuality following stroke have focused primarily on sexual activity (16–18). However, the 18 items prioritized by our panel as core content for inclusion in post-stroke sexual rehabilitation curricula reflect a much broader understanding of sexuality. The additional 27 content areas that achieved a high level of consensus, but a lower level of priority, potentially point to the need for a stepped care (32) approach to sexual rehabilitation. Using a stepped care model, the majority of stroke survivors and their partners could be offered a core programme during the first stage (Step 1) of a sexual rehabilitation curriculum. In the second stage (Step 2), those who need additional support could select other content areas based on individual need and preference. This stepped care approach would need evaluation, but potentially offers a method of addressing sexuality within existing stroke rehabilitation services.
Participants in this study did not exclude sexuality from any stage of the stroke rehabilitation continuum. However, there was high level of consensus for the subacute and chronic stages of stroke recovery as key points when intervention should be offered. It is perhaps not surprising that participants did not believe sexual rehabilitation should be prioritized during the earliest stages of stroke recovery, given that, for many, the acute phase is focused on achieving medical stability and preparing for rehabilitation. This finding also reflects previous research, where most stroke survivors want counselling about sexuality between 3 and 12 months post-stroke (5). However, there was a high level of consensus that access to sexual rehabilitation services should be available throughout the continuum. Clinicians and researchers therefore need to be mindful of the individual nature of stroke recovery and recognize that individuals will require support to adjust to post-stroke sexuality at different times in their recovery journey.
Previous research indicates that stroke survivors, their partners and health professionals struggle to openly discuss sexuality (1). However, despite this struggle, participants in our study prioritized face-to-face delivery by health professionals over other modes. Given the high levels of discomfort reported by stroke professionals regarding sexuality (11), this finding suggests an urgent need for education and training to support professionals as they assume this new role. Further work is also needed to explore how stroke survivors and their partners might be supported to take on roles as peer counsellors, including their training and education needs.
Participants prioritised rehabiltiation physcians, nurses with specialist knowledge in stroke and sexuality, psychologists, physiotherapists and sexologists/sex educators/ counsellors as the preferred service providers. Previous research has also identified physicians and nurses as key providers of sexual rehabilitation counselling (5), but limited attention has been given to the roles of allied health professionals in addressing sexuality after stroke. Our study suggests a need to adopt a multidisciplinary approach to sexual rehabilitation. Although sexologists may not be routinely available for referrals by stroke rehabilitation teams, our findings suggest that there is a need to develop onward referral pathways for stroke survivors and their partners when needs cannot be met by traditional stroke rehabilitation professionals. Furthermore, stroke survivors with communication difficulties need access to speech pathologists who can support communication about sexuality.
While the Delphi methodology allowed consensus to be reached on the content and delivery of sexual rehabilitation following stroke, there are some study limitations. First, although we attempted to recruit a diverse panel of experts, our panels were largely composed of people who identified as heterosexual, and who, for the most part, came from white Australian backgrounds. If their backgrounds had been more diverse, different aspects of sexuality may have been prioritized. Secondly, while we successfully recruited stroke survivors with self-reported communication difficulties, the nature of the survey meant that in-depth description and assessment of communication was not conducted. Thus, we may not have provided a comprehensive description of all aspects of their communication presentation. Readers should note this limitation when considering how representative our participants are of people with communication impairment following stroke.
Finally, although there were high levels of consensus among panel members regarding inclusion of content, timing and mode of service delivery, panel members failed to exclude any of the original content areas presented in the first round of data collection. This lack of discrimination may reflect their limited exposure to, and experience with, sexual rehabilitation. The majority of stroke survivors and their partners in our study did not receive any information or advice from health professionals regarding sexuality. Therefore, it could be argued that the knowledge of these experts was limited, and responses represent their best judgement on what content might be helpful. Despite this limitation, we believe that the inclusion of open-ended questions throughout the survey allowed panellists to comment and express their views, resulting in greater ecological validity of results.
In conclusion, there is a need for informed, evidence-based interventions to address sexuality after stroke. This study presents the opinions of stroke survivors, their partners, clinicians and researchers. Inclusion of stroke survivors with self-reported communication impairments offers new insights into their needs. The range of content include by participants represents a broad understanding of sexuality. There was a high level of consensus on content areas that were important to respondents. In a subsequent pilot randomized controlled trial, the intervention will be evaluated with regard to feasibility of implementation, acceptability of the developed intervention, retention of stroke survivors and their partners, and compliance.
This research was supported by the Stroke Foundation Australia through a Small Project Research Grant (SPG1713).


 Click to show fullsize
Click to show fullsize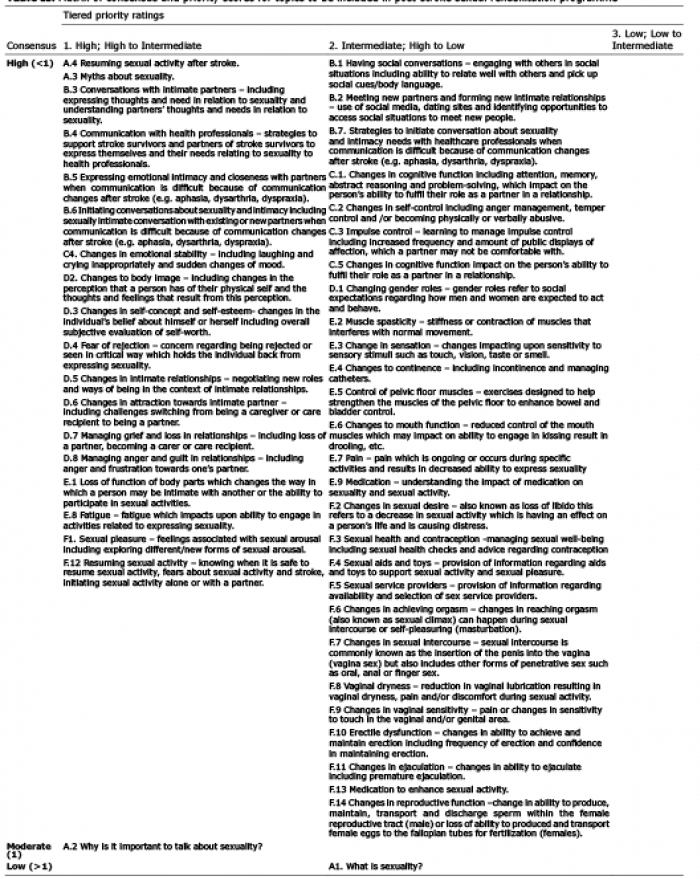 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize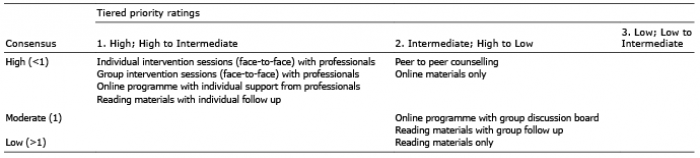 Click to show fullsize
Click to show fullsize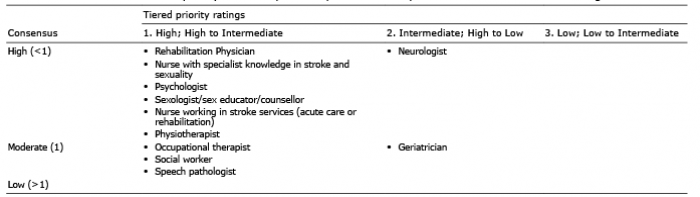 Click to show fullsize
Click to show fullsize