
From the 1Department of Clinical Sciences, Danderyd Hospital, Karolinska Institutet, 2Department of Molecular Medicine and Surgery, Karolinska Institutet and Patient Area Endocrinology and Nephrology, Inflammation and Infection Theme, Karolinska University Hospital and 3Department of Clinical Neuroscience, Section for Neurosurgery, Karolinska Institutet, Stockholm, Sweden
Objective: To explore associations between pituitary dysfunction and clinical outcome at 12 months after traumatic brain injury and aneurysmal subarachnoid haemorrhage.
Methods: Prospective cohort study of 82 patients with traumatic brain injury and 45 with aneurysmal subarachnoid haemorrhage, included at one neurointensive care unit. Baseline data comprised age, sex, Glasgow Coma Scale (GCS) score, S100B and pupil light reactions. Hormone data were collected in the neurointensive care unit and after 3, 6 and 12 months. Outcome was assessed with Barrow Neurological Institute Screen for Higher Cerebral Functions (BNIS), Rancho Los Amigos Cognitive Scale-Revised (RLAS-R) and Glasgow Outcome Scale Extended (GOSE).
Results: The most frequent hormonal deviations were hypogonadotropic hypogonadism (38%) and hypercortisolism (52%). At 12 months, performance on BNIS was impaired in 54% and GOSE in 37%. Controlling for baseline variables, low levels of gonadal hormones were associated with lower GOSE score (b = –0.80, p = 0.033), high levels of prolactin with lower RLAS (b = –1.42, p = 0.034) and high levels of serum insulin-like growth factor I (S-IGF-I) with lower RLAS level (b = –1.78, p = 0.002) and lower GOSE score (b = –1.49, p = 0.006).
Conclusion: These data suggest that pituitary dysfunctions during the first year after traumatic brain injury and aneurysmal subarachnoid haemorrhage may have clinically relevant, independent effects on clinical outcome at 12 months.
Key words: traumatic brain injury; subarachnoid haemorrhage; outcome; pituitary dysfunction.
Accepted Jan 29, 2019; Epub ahead of print Feb 14, 2019
J Rehabil Med 2019; 51: 00–00
Correspondence address: Anna Tölli, Department of Clinical Sciences, Danderyd Hospital, Karolinska Institutet, 182 88 Stockholm, Sweden. E-mail: anna.tolli@ki.se
Traumatic brain injury and aneurysmal subarachnoid haemorrhage are leading causes of physical, cognitive and behavioural disabilities. Traumatic brain injury and aneurysmal subarachnoid haemorrhage may affect the hypothalamus and pituitary gland, which are of major importance for our hormone balance. The purpose of the study was to investigate the relationship between the pituitary dysfunction after traumatic brain injury and aneurysmal aneurysmal subarachnoid haemorrhage, and cognitive and global outcomes at 12 months after the injury. In total, we included 127 patients during neurointensive care. Follow-up was at a rehabilitation medicine department. The study showed negative associations between high level of growth hormone and prolactin and behavioural and cognitive function; and between low gonadotropins and high prolactin and global outcome. We conclude that some pituitary dysfunctions during the first year after traumatic brain injury and aneurysmal subarachnoid haemorrhage may have clinically relevant, independent effects on clinical outcome at 12 months.
Pituitary dysfunction (PiD) following traumatic brain injury (TBI) has been subject to several studies. A systematic review by Lauzier et al. in 2014 (1) concluded that approximately one-third of patients with TBI will develop at least 1 anterior pituitary disorder, and that older age, TBI severity and skull fractures are risk factors for PiD. They pointed out the need for further studies to clarify the clinical impact of PiD after TBI to guide systematic screening for PiD after TBI.
Corresponding studies of PiD following aneurysmal subarachnoid haemorrhage (aSAH) were reviewed by Robba et al. in 2016 (2). They concluded that approximately half of patients with aSAH exhibit PiD in the acute phase and one-quarter in the chronic phase, and that surgical treatment of the aneurysm and age had an impact on the prevalence of PiD after aSAH. As for TBI, the impact of PiD on clinical outcome after aSAH remains to be clarified.
Both TBI and aSAH may cause a wide range of disabilities (3, 4), as often assessed by global measures, such as the Glasgow Outcome Scale (GOS) (5) or the extended version (GOSE) (6). Cognitive impairments are common after both TBI (7, 8) and aSAH (4) and global measures may not be sensitive enough to capture these. While comprehensive neuropsychological testing is demanding, some studies have used screening methods, such as the Montreal Cognitive Assessment (9) or the Barrow Neurological Institute Screen for Higher Cerebral Functions (BNIS) (10), to describe cognitive disturbances after acquired brain injury. The BNIS has documented validity (11–13), is easily applicable in clinical routine and has been used in some studies of TBI (13, 14) as well as stroke (15, 16).
In 2 previous studies (17, 18) of PiD in a prospective cohort of patients with moderate and severe TBI or aSAH, we observed frequencies of PiDs within the same range, as reported in recent reviews (1, 2). Most PiDs were transient, with no need for replacement therapy, but a small subgroup (7%) needed such therapy. In this cohort of patients, who were recruited from the neurointensive care unit at one university hospital and who went through the same structured neurorehabilitation and follow-up programme, we also assessed cognitive and global function until one year after the event (19). Cognitive and global function improved significantly over time in both diagnostic groups and was not significantly different between groups at 12 months. Higher age was associated with lower BNIS T-scores after TBI, but not after aSAH, and lower initial GCS scores were associated with poorer cognitive outcome after TBI, but not after aSAH. Data from this cohort enable us to explore the potential impact of PiD on cognitive and global outcome after TBI and aSAH.
Thus, the aim of the present study was after TBI and aSAH to explore associations between PiD and cognitive and global outcome at 12 months post-injury, controlling for age, gender and acute injury variables.
The design of this prospective, observational study of patients with moderate or severe TBI and aSAH has been described previously (17, 18). Patients were included at the neurointensive care unit (NICU) at Karolinska University Hospital (KUH) from March 2009 to June 2012, and subsequently followed at the Department of Rehabilitation Medicine at Danderyd University Hospital, Stockholm, Sweden, at 3, 6 and 12 months post-event. Hormone testing was performed at Department of Endocrinology, KUH. Inclusion required a lowest Glasgow Coma Scale (GCS) score during the first day after the event of 3–13, age ≥ 18 years, living in the Stockholm region, and obtained informed consent. For patients who were unconscious or otherwise unable to give informed consent, the closest relative was asked.
The study was approved by the Regional Ethics Review Board in Stockholm (no: 2008/3:9 2008/1574-31/3).
Severity grading. Clinical severity measures included the GCS score (20, 21) (3–8 severe injury, 9–13 moderate injury), serum levels of S100B (highest level of S100B between 12–36 h after injury was categorized as normal if < 0.11, mild 0.11–0.25, moderate 0.26–0.50, and severe if ≥ 0.51μg/l), and pupil light reactions (categorized as normal or abnormal).
Endocrine function. Analyses of thyroid function; serum free thyroxine (S-fT4), serum thyroid-stimulating hormone (S-TSH), serum free triiodothyronine (S-fT3) and the synacthen test were performed 10 days post-event.
Analyses at 3, 6 and 12 months comprised thyroid function and S-cortisol. At 6 and 12 months analyses were performed for S-insulin-like growth factor I (IGF-I), S-prolactin, S-oestradiol in females, S-follicle-stimulating hormone (FSH) in females, S-luteinizing hormone (LH) in females, and S-testosterone in males.
Blood was sampled between 8 and 10 am. S-cortisol ≥400 nmol/l was set as normal. At 3, 6 and 12 months post-event a synacthen test was performed in patients with a morning S-cortisol < 400 nmol/l.
The synacthen test was performed by intravenous administration of 250 µg synacthen. Blood samples were taken before and 30 min after injection. A normal response to the synacthen test was defined as S-cortisol at 30 min > 550 nmol/l. Cortisol responses were arbitrarily categorized as < 550 nmol/l, between 550 and 1,000 nmol/l or > 1,000 nmol/l.
Hypothyroidism was defined as fT4 level below the normal reference range. The reference data for S-fT4 is shown in Table SI1.
An age-dependent reference range (geometrical mean±2 standard deviation (SD)) for IGF-I, independent of sex, was calculated based on the equation for the regression line in all patients: 10log [IGF-I (μg/l)]= 2.581–0.00693 × age (years), with SD = 0.120 (22). Decreased secretion of growth hormone (GH) was presumed if IGF-I <–2SD and high level if S-IGF-I >+2SD.
Gonadotrophin dysfunction in men was defined as S-testosterone below reference range, and in post-menopausal women was defined as S-FSH, and S-LH or S-oestradiol below the normal reference range, in pre-menopausal women in combination with amenorrhoea or oligomenorrhoea. The reference range of S-testosterone, S-oestradiol, S-FSH, S-LH are shown in Table SI1.
Patients were divided in groups of those who showed normal, low or high hormone levels at any time-points during the first year after the event. Patients with low and high hormones at different time-points during the study period were excluded from the calculations.
Analysis of all blood samples were performed at the Department of Clinical Chemistry in KUH using routine commercial kits.
The Barrow Neurological Institute Screen for Higher Cerebral Functions (BNIS) (10) includes a pre-screen test (level of arousal 3 points, basic communication 3 points, and cooperation 3 points). The patients must achieve at least 2 points on each of the items to continue with assessment of higher cerebral functions: speech and language (15 points), orientation (3 points), attention/concentration (3 points), visual and visuospatial problem solving (8 points), memory (7 points), affect (4 points) and awareness of own performance (1 point), corresponding to a total score of maximally 50 p. A cut-off score of < 47 was set for identifying brain dysfunction for patients < 60 years, < 46 for patients 60–69 years and <44 for patients > 70 years (12, 13, 23). Total BNIS raw scores are converted to age-corrected standard T-points (< 1–71). Cut-off for cognitive dysfunction for T-points was set at < 40 (i.e. <–1 SD) (24).
Patients who failed pre-screen test were assigned a T-point of 0.
The Rancho Los Amigos Cognitive Scale-Revised (RLAS-R) (25) was used to categorize level of cognitive and behavioural function. RLAS-R scores from 1 to 10 represent 10 stages of recovery after brain injury, as reflected by the ability to follow commands, the presence of non-purposeful behaviour, cooperation, confusion, attention to environment, verbal ability, memory, orientation and higher cognitive ability. RLAS-R levels were dichotomized into ”inferior functioning” (RLAS-R 1–8) and ”superior functioning” (RLAS-R 9–10).
The Glasgow Outcome Scale Extended (GOSE) was used to assess global outcome and independence (5). The 8 categories extend from ”Dead” (score 1) to ”Upper Good Recovery” (score 8). GOSE scores were dichotomized into ”unfavourable outcome” (GOSE 1–4) and ”favourable outcome” (GOSE 5–8).
Statistical analysis was performed using IBM SPSS Statistics version 25 (IBM Corp., Armonk, New York, USA). Descriptive data comprise central measures (mean, median or percent) and measures of spread (SD, percentile, min–max). Non-parametric methods were used, as data were not normally distributed according to Shapiro–Wilk’s test of normality.
Mann–Whitney U test was used for group comparisons of GCS, peak S100B (12–36 h), and comparisons of results of BNIS, RLAS-R and GOSE between 2 subgroups of hormone dysfunction. Pearson χ2 test was used for group comparisons of sex, severity of injury, age groups, and anterior pituitary dysfunction. Fisher’s exact test was used for comparisons of pupil reaction to light stimulation at admission. Kruskal–Wallis test was used for multiple comparisons of results of BNIS, RLAS-R and GOSE between 3 subgroups of hormone dysfunction. Analysis of variance (ANOVA) was used for group comparisons of age and body mass index (BMI). Spearman’s correlation coefficient was used for analysis of bivariate correlation between hormone dysfunction and BNIS.
Multiple linear regression analyses were used to examine the relationship between BNIS or RLAS or GOSE and hormone dysfunctions, GCS, sex and age. In all cases, significance level was set at p < 0.05.
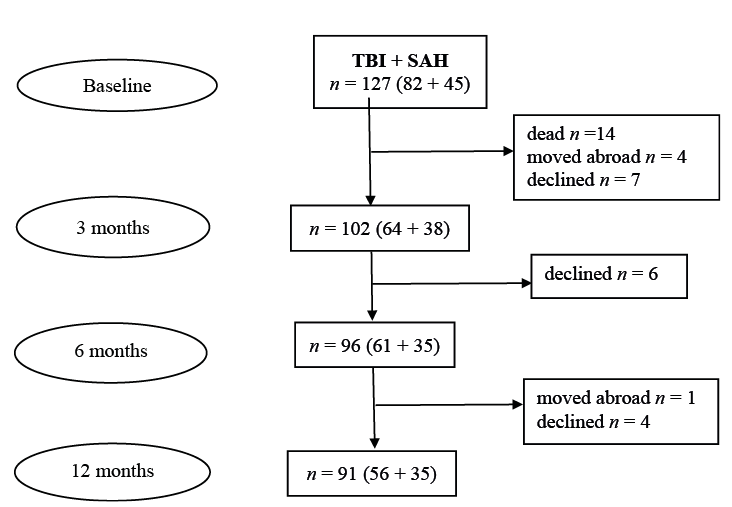
Out of 127 patients, 82 with TBI and 45 with SAH, data from 91 patients were available for analyses (Fig. 1). Drop-outs did not differ from retained study participants regarding sex (p = 0.121/p = 0.095), age (p = 0.094/p = 0.280) or GCS scores (p = 0.073/p = 0.205).
Fig. 1. Flow chart of study participants.
Data are displayed in Table I. Of the 91 patients, (49 men, 42 women, mean age 51.0±15.2 years), 66 had a severe and 25 patients had a moderate brain injury according to the admission GCS score. There was no significant difference between patients with TBI or with aSAH regarding GCS scores (p = 0.144), BMI (p = 0.893), while there was significant difference in age (p = 0.001) and sex (p < 0.001).
Table I Baseline data of patients with traumatic brain injury (TBI) and aneurysmal subarachnoid haemorrhage (aSAH)
PiDs were frequent and comprised all hormone axes, as shown in Tables II–IV. Most PiDs were singular. Multiple (2 or more) PiDs occurring at the same time in individual patients were observed in 7 (8%) in the acute stage, in 1 (1%) at 3 months, in 3 (3%) at 6 months and in 3 (3%) at 12 months’ follow-up. The results of comparisons of subgroups with normal, low or high hormone levels are shown in Tables II–IV.
Data are displayed in Table II. At 12 months’ follow-up, in total 16% (15/91) patients failed pre-screen of BNIS. Of those who performed the BNIS test, in total 35% (32/91) patients scored below cut-off for cognitive dysfunction (T-points < 40).
Table II. Relations between hormone function during the first year after traumatic brain injury (TBI) and aneurysmal subarachnoid haemorrhage (aSAH), and Barrow Neurological Institute Screen for Higher Cerebral Functions (BNIS) results at 12 months post-event
BNIS T-scores were significantly lower (p = 0.018) in the subgroup with high thyroid levels in comparison with those with normal thyroid levels. Patients with high thyroid levels were significantly (p = 0.016) older (mean 60.4 years (SD 9.5) than patients with normal thyroid levels (mean 50.6 years (SD 14.9). Comparisons of the other baseline variables showed no significant differences in any subgroup.
Multiple linear regression analysis demonstrated significant associations between BNIS T-score at 12 months after the event and age (b = –0.44, p = 0.027, CI: –0.83 ––0.05), GCS (b = 1.48, p = 0.036, CI: 0.10–2.87), but not with sex (b = 7.42, p = 0.170), or with high T4 (b = –12.46, p = 0.063), or with low T4 (b = –10.08, p = 0.095). Thyroid level, age, GCS and sex explained 20.4% of the variance in the BNIS T-scores (adjusted R2 = 0.204).
BNIS T-scores were significantly lower (p = 0.012) in the subgroup with high IGF-I levels in comparison with those with normal IGF-I levels. Patients with high IGF-I levels were significantly (p = 0.021) older (mean 60.8 years (SD 9.8) than patients with normal IGF-I levels (mean 50.6±14.8 years). Comparisons of the other baseline variables showed no significant differences in any subgroup.
Multiple linear regression analysis demonstrated significant relationships between BNIS T-score at 12 months after the event with age (b = –0.49, p = 0.011, CI: –0.88––0.12), and GCS (b = 1.42, p = 0.042, CI: 0.05–2.79), but not with sex (b = 5.39, p = 0.311), or with high IGF-I (b = –10.33, p = 0.142), or with low IGF-I (b = –0.91, p = 0.907). IGF-I level, age, GCS and sex explained 17.1% of the variance in the BNIS T-scores (adjusted R2 = 0.171).
BNIS T-scores were significantly lower (p = 0.027) in the subgroup with low prolactin levels in comparison with those with normal prolactin levels. Comparisons of the other baseline variables showed no significant differences in any subgroup.
Multiple linear regression analysis demonstrated significant relationships between BNIS T-score at 12 months after the event with age (b = –0.513, p = 0.005, CI: –0.87––0.16), GCS (b = 1.35, p = 0.043, CI: 0.05–2.65) and low prolactin (b = –31.02, p = 0.016, CI: –56.15––5.89), but not with sex (b = 5.81, p = 0.274) or with high prolactin (b = –13.83, p = 0.083). Prolactin level, age, GCS and sex explained 23.6% of the variance in the BNIS T-scores (adjusted R2 = 0.236).
BNIS T-scores did not differ between subgroups with different cortisol levels (p = 0.468) and gonadotrophin levels (p = 0.267).
Multiple linear regression analysis demonstrated no significant relationship between BNIS T-score at 12 months after the event and low (b = –3.00, p = 0.572) or high hormones levels (b = 3.53, p = 0.492).
Data are displayed in Table III.
At 12 months, 51% (46/91) patients had ”inferior cognitive functioning” and 49% (45/91) had ”superior cognitive functioning”.
Table III. Relations between hormone function during the first year after traumatic brain injury (TBI) and aneurysmal subarachnoid haemorrhage (aSAH), and Rancho Los Amigos Cognitive Scale-Revised (RLAS-R) results at 12 months post-event
RLAS-R scores were significantly lower (p = 0.026) in the subgroup with high thyroid levels in comparison with those with normal thyroid levels. Patients with high thyroid levels were significantly (p = 0.011) older (mean 59.9 years (SD 9.3) than patients with normal thyroid levels (mean 50.0 years (SD 14.7). Comparisons of the other baseline variables showed no significant differences in any subgroup.
Multiple linear regression analysis demonstrated significant relationship between RLAS-R score at 12 months after the event with GCS (b = 0.14, p = 0.020, CI: 0.02–0.26), but not with age (b = –0.03, p = 0.113), or with sex (b = 0.87, p = 0.058), or with high T4 (b = –0.84, p = 0.133) or with low T4 (b = –0.17, p = 0.738). Thyroid level, age, GCS and sex explained 16.6% of the variance of the RLAS-R scores (adjusted R2 = 0.166).
RLAS-R scores were significantly lower (p = 0.006) in the subgroup with high IGF-I levels in comparison with those with normal IGF-I levels. Patients with high IGF-I levels were significantly (p = 0.019) older (mean 60.1 years (SD 9.7) than patients with normal IGF-I levels (mean 50.2 years (SD14.8). Comparisons of the other baseline variables showed no significant differences in any subgroup.
Multiple linear regression analysis demonstrated significant relationships between RLAS-R score at 12 months after the event with GCS (b = 0.13, p = 0.019, CI: 0.02–0.24), and high IGF-I (b = –1.78, p = 0.002, CI: –2.87––0.70), but not with age (b = –0.03, p = 0.074), or with sex (b = 0.62, p = 0.144), or with low IGF-I (b = 0.29, p = 0.639). IGF-I level, age, GCS and sex explained 24.3% of the variance on the RLAS-R scores (adjusted R2 = 0.243).
RLAS-R scores were significantly lower (p = 0.025) in the subgroup with high prolactin levels in comparison with those with normal prolactin levels. Comparisons of the other baseline variables showed no significant differences in any subgroup.
Multiple linear regression analysis demonstrated significant relationships between RLAS-R score at 12 months after the event with age (b = –0.04, p = 0.013, CI: –0.07––0.01), GCS (b = 0.12, p = 0.037, CI: 0.01–0.23) and high prolactin (b = –1.42, p = 0.034, CI: –2.73––0.11), but not with sex (b = 0.54, p = 0.236), or with low prolactin (b = –1.20, p = 0.285). Prolactin level, age, GCS and sex explained 18.2% of the variance of the RLAS-R scores (adjusted R2 = 0.182).
RLAS scores did not differ between subgroups with different cortisol levels (p = 0.674) and gonadal levels (p = 0.182).
Multiple linear regression analysis demonstrated no significant relationships between RLAS-R score at 12 months after the event and low (b = –0.18, p = 0.678) or high hormone levels (b = –0.12, p = 0.783).
Data are displayed in Table IV. At 12 months, 37% (34/91) of patients had a bad outcome and 63% (57/91) had a good outcome.
Table IV. Relations between hormone function during the first year after traumatic brain injury (TBI) and aneurysmal subarachnoid haemorrhage (aSAH), and Glasgow Outcome Scale Extended (GOSE) results at 12 months post-event
GOSE scores were significantly lower (p = 0.011) in the subgroup with high thyroid levels in comparison with those with normal thyroid levels. Patients with high thyroid levels were significantly (p = 0.011) older (mean 59.9 years (SD 9.3) than patients with normal thyroid levels (mean 50.0 years (SD 14.7). Comparisons of the other baseline variables showed no significant differences in any subgroup.
Multiple linear regression analysis demonstrated a significant relationship between GOSE score at 12 months after the event with age (b = –0.04, p = 0.004, CI: –0.07––0.01), but not with sex (b = 0.30, p = 0.420), or with GCS (b=0.08, p = 0.086), or with high T4 (b = –0.90, p = 0.051), or with low T4 (b = –0.16, p = 0.696). Thyroid level, age, GCS and sex explain 21.2% of the variance in the GOSE scores (adjusted R2 = 0.212).
GOSE scores were significantly lower (p = 0.011) in the subgroups with low gonadotrophin levels in comparison with those with normal levels. Patients with low gonadotrophin levels were significantly (p = 0.013) older (mean 57.4 years (SD 12.2) than patients with normal gonadotrophin levels (mean 49.6 years (SD 14.6). Comparisons of the other baseline variables showed no significant differences in any subgroup.
Multiple linear regression analysis demonstrated significant relationships between GOSE score at 12 months after the event with age (b = –0.046, p = 0.001, CI: –0.07––0.02), GCS (b = 0.11, p = 0.025, CI: 0.01–0.21) and low gonadotrophins (b = –0.80, p = 0.033, CI: –1.54––0.07), but not with sex (b = 0.16, p = 0.675). Gonadotrophin level, age, GCS and sex explained 24.5% of the variance on the GOSE scores (adjusted R2 = 0.245).
GOSE scores were significantly lower (p = 0.022) in the subgroup with high prolactin levels in comparison with those with normal prolactin levels. Comparisons of the other baseline variables showed no significant differences in any subgroup.
Multiple linear regression analysis demonstrated significant relationship between GOSE score at 12 months after the event with age (b = –0.05, p < 0.001, CI: –0.08––0.03) and high prolactin (b = –1.49, p = 0.006, CI: –2.55––0.43), but not with sex (b = 0.03, p = 0.926), GCS (b = 0.07, p = 0.132) or low prolactin (b = –0.84, p = 0.354). Prolactin level, age, GCS and sex explain 25.5% of the variance on the GOSE scores (adjusted R2=0.255).
GOSE scores did not differ significantly between subgroups of patients with different cortisol levels (p = 0.305) and IGF-I levels (p = 0.158).
Multiple linear regression analysis demonstrated no significant relationship between GOSE score at 12 months after the event and low (b =–0.44, p = 0.213) or high hormone levels (b =0.42, p = 0.215).
The main finding of this study of patients with TBI or aSAH, is that low levels of gonadal hormones and high levels of somatotrophic hormones (IGF-I) and prolactin, occurring at any of the 4 test-points during the first year after the event, were independently associated with poorer clinical outcome at 12 months. The magnitude of some of the observed effects of PiDs seem clinically relevant, with, for example, regression coefficients indicating that presence of hypogonadism during the first year after the event will lower the GOSE score at 12 months by 1 point. Taken together, the identified independent variables explained 16–25% (R2) of the variation in outcome variables. Thus, there are, other factors explaining a large part of the variation in outcome.
It is notable that signs of pituitary hypofunction or hyperfunction were frequent during the first year after the event, and most of these were transient, as reported previously (18). The most common hypofunction in the current study group was for gonadal hormones, observed in 38%, and most common hyperfunction for high cortisol levels in 52% (Table II). As recently reported (19), although both cognitive and global function improves significantly until 12 months after both TBI and aSAH, impairments remain at 12 months. In the current study group, cognitive impairment according to BNIS was present in 54% of cases and impaired global outcome according to GOSE in 37%. Higher age and lower GCS score had an independent effect on cognitive and global outcome, while no association was observed with sex or the other injury severity variables, which agrees with the results of previous studies (26–29).
This study investigated whether signs of pituitary dysfunction (hypo- or hyper-function) at any time-point were associated with outcome. In our study we observed both hypo- and hyper-function of the thyroid, adrenal and somatotrophic axes (17, 18). It can be speculated why both hypo- and hyper-function of the pituitary occurs, but it might be related to different reactions to stress and changes in body weight. Most previous studies observed pituitary hypofunction in one or multiple axes (1, 2), but only a few studies reported hyperfunction of the adrenal axis (30), thyroid axis (31) and somatotrophic axis (30).
Low gonadotrophins had a significant negative association with GOSE, but not with BNIS or RLAS-R. This finding is in agreement with the results of several previous studies reporting on the impact of multiple hormone dysfunctions, including the gonadotrophic axis, such as studies of patients with aSAH (32–34) and patients with both TBI and aSAH (35), all reporting worse outcome, as measured by GOS. One previous study by Marina et al. (30) also used GOSE and observed a negative impact of low gonadotrophins in patients with TBI. Thus, even though study samples and design differ and previous studies assessed outcome with GOS, the findings regarding an association between gonadal hormone insufficiencies and worse global outcome are concordant. One previous study on TBI by Bondanelli et al. (29) reported a negative impact specifically of gonadotrophin disturbances on cognitive/behavioural function, with outcome measured with Disability Rating Scale (DRS) and with RLAS. These findings are also in agreement with ours regarding global outcome, while we observed no association with cognitive function according to RLAS-R or BNIS. This discrepancy may have several causes, including that our study also used data from patients with aSAH.
No signs of an impact of either abnormal thyroid or cortisol level were found. BNIS, RLSA-R and GOSE were lower in the subgroup with high thyroid levels at group comparison, but when multivariate analysis was made, no independent association was seen. Thus, although frequent, neither high nor low T4 or cortisol levels were associated with worse cognitive or global outcome at 12 months. This finding is in contrast to studies demonstrating that hypothyroidism and hyperthyroidism, as well as low or high glucocorticoid levels (36) may have a negative impact on cognitive function (37), but in line with a study by Schneider et al. (35) of TBI and aSAH, who found no impact of corticotropic dysfunction on GOS. The discrepancies observed in the studies might be caused by differences in study cohorts, differences in methods of hormonal analyses, as well as interpretation of these and the degree of hormonal abnormality.
Regarding the somatotrophic axis, high IGF-I had a significant negative association with RLAS-R, but no association with BNIS. The cause of increased levels of IGF-I as well as of other hormones, as frequently observed in our study, but not often reported in other studies is not clear. Factors at play may include somatic stress reactions as well as complex interactions between the pituitary hormones, as suggested previously (31). Notably, we observed no association between low IGF-I levels and GOSE, which agrees with findings by Schneider et al. (35) in the study of TBI and aSAH, who observed no impact of somatotrophic dysfunction on GOS.
However, it should be pointed out that an IGF-I level within normal reference range does not exclude GH deficiency, since 30% of patients with GH deficiency have IGF-I levels within the normal reference range (38). Thus, there is a risk for underestimation of growth hormone deficiency in our study.
Prolactin levels were low in too few patients to allow any conclusion. High prolactin levels were more frequent and were associated with lower performance according to RLAS-R and GOSE. This is in agreement with a study by Marina et al. (30), who reported lower GOSE in patients with TBI and elevated stress hormones (prolactin, IGF-I and cortisol).
The analyses of associations between multiple low hormone /values and outcome were hampered by the low frequency of multiple hormone deviations in individual patients at any of the 4 test-points. Thus, our finding of no significant associations between multiple low or high hormones and outcome measured with BNIS, RLAS-R or GOSE at 12 months after the event must be interpreted with caution. Even though our results are in line with a study of patients by Bavisetty et al. (39), who found no association between pituitary dysfunction (somatotrophic, gonadotrophic, thyreotrophic, corticotrophic, posterior pituitary axes) and GOSE after TBI, it is reasonable to assume that multiple pituitary dysfunction would have more impact on clinical outcome than isolated pituitary dysfunction, as also indicated in some previous studies.
Our data suggest that global measures, such as GOSE, may be more sensitive to an impact of pituitary dysfunction than specific cognitive measure, such as BNIS. One may speculate that this reflects that not only cognitive function, but also other, e.g. emotional, motor or musculoskeletal functions, are also disturbed by pituitary dysfunction and impact on the global outcome according to GOSE. We believe that further studies are warranted to elucidate this, to increase our understanding of the clinical impact of pituitary dysfunction, and to learn whether there is any reason to intervene in terms of substitution therapy outside established treatment criteria in order to enhance recovery after TBI or aSAH.
To the best of our knowledge, this is the first study to explore the potential effects of pituitary dysfunction on clinical outcome after TBI or aSAH by use of systematic measurements of hormone levels at 4 time-points during the first year after the event and by cognitive assessment with BNIS and global measures, while most previous studies used only global measures, most often GOS or GOSE. Study participants were all managed at the same NICU and with the same, structured follow-up, which should reduce confounding regarding acute and later interventions, but also limits generalizability. Similarly, all clinical assessments were performed by the same person (AT), which should strengthen the reliability of assessment data, but also bears a risk for systemic bias of scoring. However, we consider this risk low, as most assessments are highly standardized.
Due to sample size and small subgroups of patients, power issues must be considered. Thus, there is a risk that some associations were not detected due to type II errors. Although adherence was fairly good for this kind of longitudinal study, the presence of drops-outs and missing data carries a risk of underestimation of pituitary dysfunction in our study. IGF-I level was used as an estimate of GH secretion, which might also underestimate growth hormone deficiency (38) as discussed above. It should also be pointed out that reference values applied in this, as well as in previous, studies may overestimate the true frequency of PiDs in brain-injured populations, as recently discussed by Klose & Feldt-Rasmussen (40). Finally, we did not consider other factors that may impact on hormone levels, as well as outcome, such as comorbidities, pharmacological drug treatment, etc.
This study demonstrates that pituitary dysfunction during the first year after TBI and aSAH may have clinically relevant effects on clinical outcome at 12 months after the event, and lends further support to the need for screening of pituitary dysfunction after TBI and aSAH. The findings also point to the need for further studies to improve clinical management of these patients and may be useful for the design of larger prediction studies.
This study was supported by a grant provided by grants from Stockholm County Council (ALF-grants), Lars Hedlund (Karolinska Institutet Dnr 2-1582/2016), NovoNordisk, and partly by a grant from Pfizer, Sweden. The authors thank Johan Bring, Statisticon, for most valuable statistical advice.
The authors have no conflicts of interest to declare


 Click to show fullsize
Click to show fullsize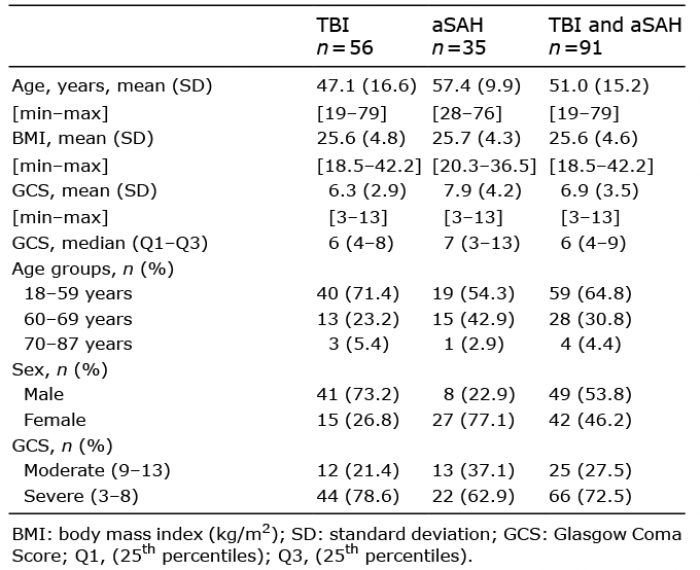 Click to show fullsize
Click to show fullsize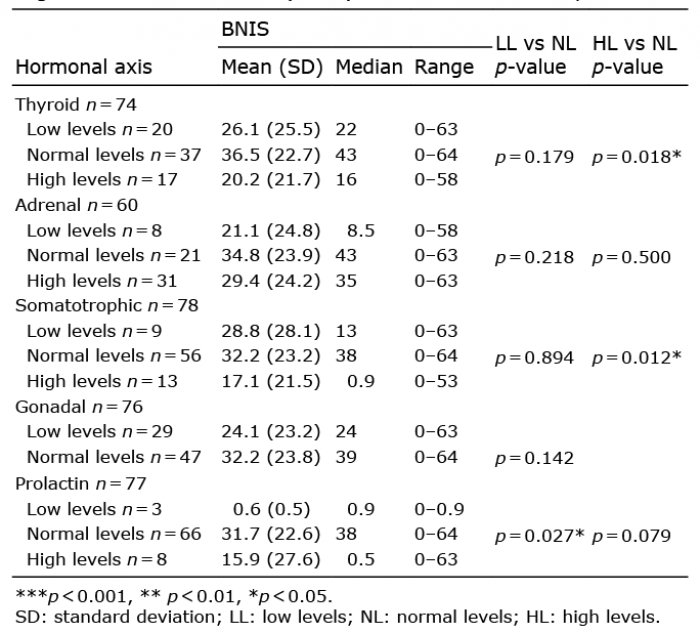 Click to show fullsize
Click to show fullsize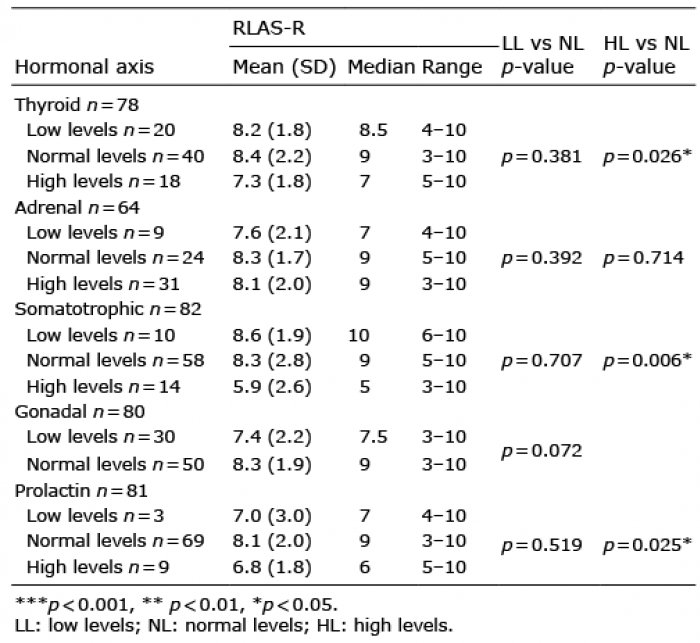 Click to show fullsize
Click to show fullsize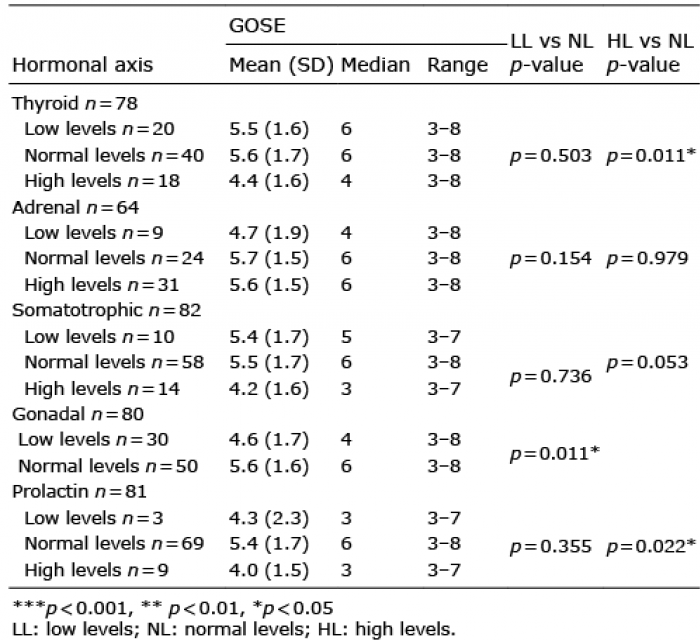 Click to show fullsize
Click to show fullsize