
From the 1Blanquerna School of Health Sciences, Ramon Llull University, 2Iberoamerican Cochrane Centre, Institut d’Investigació Biomèdica Sant Pau (IIB Sant Pau), CIBERESP, Universitat Autònoma de Barcelona (UAB), Barcelona and 3Salut i Esport Rehabilitation Center, Santa Perpètua de Mogoda, Spain.
Objective: To determine whether the appearance of a radial extracorporeal shock wave device affects clinical outcomes in chronic plantar fasciitis.
Study design: Randomized controlled parallel assessor-blinded clinical trial.
Material and methods: A total of 135 patients were assigned to 3 groups: group I, standard radial extracorporeal shock wave device; group II, standard radial extracorporeal shock wave device modified to give a more sophisticated appearance; group III, standard radial extracorporeal shock wave device modified to give a more austere appearance. The radial extracorporeal shock waves emitted by the 3 devices were identical. Primary outcome was foot function, measured with the Foot Function Index. Secondary outcomes were pain at different times, measured with a visual analogue scale, and plantar fascia thickness, measured with ultrasound.
Results: All variables decreased significantly from baseline assessment, in all 3 groups and at all time-points: 1, 2, 4 and 14 months after the last session (p < 0.001). There were no significant differences between groups for any of the variables assessed.
Conclusion: Device appearance had no statistically significant influence on clinical outcomes in patients with chronic plantar fasciitis treated with radial extracorporeal shock wave therapy.
Key words: placebo effect; nocebo effect; plantar fasciitis; shock wave, therapeutic context.
Accepted Dec 18, 2018; Epub ahead of print Jan 22, 2019
J Rehabil Med 2019; 51: 00–00
Correspondence address: Antoni Morral, Blanquerna School of Health Sciences, Ramon Llull University, 08025 Barcelona, Spain. E-mail: antonimf@blanquerna.url.edu
The context and environment in which treatment is administered is highly relevant. Context variables are perceived and interpreted by patients and can generate positive or negative expectations. Such expectations may influence the therapeutic outcome. This study assessed whether a contextual element, such as the external appearance of a shock wave device, influenced clinical outcomes in patients with chronic plantar fasciitis. Three shock wave devices were compared: a standard device; a sophisticated device; and an austere device. The only difference between the devices was their external appearance. The shockwaves emitted by the 3 devices were identical. No differences were found between the 3 devices for any of the variables assessed. Health professionals and future research into the therapeutic encounter context should focus more on patient–therapist interactions than on the appearance of devices.
P
lantar fasciitis is the most common cause of inferior heel pain. Typical symptoms include pain with the first weight-bearing step in the morning. Diagnosis of plantar fasciitis can be made clinically (1). The incidence and prevalence of the condition are not fully known; however, it is estimated that, in the general population, 1 in 10 people will experience plantar fasciitis at least once in their life (2).
Although the suffix “-itis” implies an inflammatory condition, mounting evidence indicates that this foot disorder is associated with degenerative changes and should be appropriately classified as a “fasciosis” or “fasciopathy” (3).
The causes of plantar fasciitis are multifactorial. It responds well to multiple conservative therapies. The prognosis is favourable, with resolution of symptoms in approximately 80% of cases (4). However, there is no evidence-based consensus on the most effective treatment. Systematic reviews have shown radial extracorporeal shock waves (rESW) to be effective and safe for the treatment of chronic plantar fasciitis (5–7). The biological effects of rESW are tissue regeneration, angiogenesis and analgesia (8, 9), produced by a mechanotransduction mechanism by which cells recognize and respond to mechanical stimulation (10).
There are many variables, including the placebo effect, which can explain the clinical improvement experienced by patients when they receive a pharmacological treatment or physical treatment, such as rESW (11). The placebo and nocebo responses refer to changes in patients’ symptoms attributable to their participation in a therapeutic encounter and its rituals, symbols and interactions (12). However, other elements, such as patient–therapist relationship, psychosocial factors, and patients’ hopes, beliefs and fears, must also be considered (13, 14).
The context and environment in which treatment is administered is highly relevant. Context variables are perceived and interpreted by patients and can generate positive or negative expectations (15). A placebo response occurs when a medical treatment and its context trigger specific expectations about a positive therapeutic outcome. Pre-existing optimistic expectations can amplify the positive effects of treatments (placebo effects), but negative expectations can also worsen treatment in the form of side-effects or a decrease in treatment-typical improvements (nocebo effects) (16).
Studies have shown that modifying the shape, colour or price of a placebo drug can produce different placebo responses (17, 18), yet there are few studies that explore and identify the contextual elements involved in placebo and nocebo effects; this is highly relevant, since the therapeutic effect of many treatments is inseparable from the context in which they are administered. However, there are other phenomena that can explain patients’ clinical improvement, such as the Hawthorne effect, natural fluctuations in diseases, and regression to the mean (19–21). The placebo effect can be overestimated if these are not taken into account (22).
This randomized controlled trial (RCT) aimed to assess whether a contextual element, such as the external appearance of the rESW device, would influence clinical outcomes in patients with chronic plantar fasciitis.
This randomized controlled parallel assessor-blinded clinical trial was conducted in a private rehabilitation and physiotherapy centre, “Salut i Esport”, in Santa Perpètua de Mogoda, Barcelona province, Spain. Patients were recruited from this centre and other private centres (n = 122) and from public centres (n = 13). A total of 135 patients were enrolled in the study during 2014–15.
Patients were referred to the lead investigator and considered for participation in the study according to the inclusion and exclusion criteria summarized in Table I. A total of 135 participants were recruited and 128 completed the study (Fig. 1).
After providing written informed consent, patients with chronic plantar fasciitis (more than 6 months’ duration) were randomly assigned to the following 3 groups:
Group I: standard device: therapy applied with a standard rESW device (n = 45).
Group II: sophisticated device: therapy applied with a modified standard rESW device designed to give a more attractive, high-tech appearance, with a larger external component (n = 45).
Group III: austere device: therapy applied with a modified standard rESW device designed to give a more austere, unattractive, low-tech appearance, with a smaller external component (n = 45).
Three Swiss Doloclast rESW devices (EMS Electro Medical Systems, Nyon, Switzerland), which comply with all of the European safety regulations for health equipment (Registration: EN-60601-1, Class I. Type BF IP40. 93/42 EEC) were used. Two of the 3 devices (corresponding to groups II and III), which were initially standard, were modified to change only the external part of the device without affecting the safety of the treatment or the technical performance of the equipment. The same therapeutic radial extracorporeal shock waves were used in all cases.
Table I. Inclusion and exclusion criteria for patients with chronic plantar fasciitis enrolled in the present study
Fig. 1. Flowchart of participants.
The study was approved by the Ethics and Research Commission of Blanquerna School of Health Science, Ramon Llull University (Barcelona, Spain). This study was carried out in accordance with the World Medical Association Declaration of Helsinki (23), according to good clinical practice, and registered with ClinicalTrials.gov (identifier NCT02608723).
All patients followed the same schedule of visits in an identical setting. During the first visit, patients were given an information document about the study, and the lead researcher explained the study aims with the wording: “the 3 devices are effective, all 3 are good, but we want to know which of them is best”. Information on plantar fascia and gastrocnemius muscle stretching exercises was also provided and explained. The patients then underwent a baseline evaluation: they were asked to complete the Foot Function Index (FFI) questionnaire, a visual analogue scale (VAS) was used to assess pain, and a foot ultrasound was performed. Each patient was then taken to another room containing all 3 devices, where they were to be treated. The area of the treatment room was 10 m2, it contained a stretcher, 2 chairs and the 3 devices, located next to each other (Figs 2 and 3). A second researcher explained the treatment procedure for 1 min and how the 3 rESW devices worked. He fired 32 shock waves (4 s) into the air using each device, so that the patient could hear and see the operation of the devices. The envelope assigning the device to that individual was then opened. The patient looked at the assigned device for 1 min, and was then asked to remove their shoes and lie on the stretcher in a prone position for the first session. All patients received 3 sessions, 1 per week. Patient interaction with the devices in the second and third session was the same as in the first session: the researcher explained the operation of the 3 devices for 1 min, then the patient observed the assigned device for 1 min. In each session 2,500 radial extracorporeal shock waves were applied at a frequency of 8 Hz. The applied energy was adjusted to the maximum discomfort the patient could tolerate, resulting in an individual air pressure of between 2.0 and 4.0 bar and, thus, a positive energy flux density of between 0.10 and 0.18 mJ/mm2. No local anaesthesia or analgesic drugs were given during the sessions. The patients were followed-up at 1, 2, 4 and 14 months after the last radial extracorporeal shock wave therapy (rESWT) session.
Fig. 2. The devices used in the present study: (1) sophisticated device; (2) austere device; (3) standard device.
Fig. 3. Close-up of the devices: (1) sophisticated device; (2) austere device; (3) standard device.
The primary outcome was foot function, measured using the FFI, a self-administered questionnaire that quantifies the impact of pathology on foot function in terms of pain, disability and activity restriction (24), and is one of the most-used assessment tools in clinical trials on plantar fasciitis treatments (25, 26). The index consists of 23 items that assess foot function on a continuous scale of 100 points, where a lower score indicates better function. This variable was assessed at baseline and at 4 follow-up sessions: at 1, 2, 4 and 14 months after the last rESWT session.
Secondary variables included: (i) pain assessment for “pain with the first weight-bearing step in the morning” and “pain during the day”, measured with a 10-point VAS at baseline and at 4 follow-ups: at 1, 2, 4 and 14 months after the last rESWT session; (ii) plantar fascia thickness of the affected foot, measured using ultrasound (Echo Blaster EXT-128) at baseline and at 2 time-points: 4 and 14 months after the last rESWT session. Complications, adverse effects during and after treatment were recorded. Information was also collected on discomfort during the application of rESWT (using a VAS scale).
Baseline patient data collected included age, sex, body mass index (BMI) (kg/m2), duration of symptoms (months), time spent standing per day (h), exercise level (1, no activity; 2, less than 5 h a week; 3, between 5 and 10 h a week; 4, more than 10 h a week), and level of education (1, no education; 2, compulsory education (primary and secondary school); 3, high-school studies or vocational training; and 4, university-level education).
Randomization was performed through a specific syntax for this study, in IBM-SPSS language (V22), in blocks and perfectly balanced by a statistician from the Ibero-American Cochrane Centre, Clinical Epidemiology and Public Health Service of the Hospital de la Santa Creu i Sant Pau. The randomization numbers were placed in sealed opaque envelopes, thus concealing allocation from both the patients and the therapist until treatment started. The envelopes were sequentially ordered from 1 to 135 and stored in a locked cabinet. Both the lead researcher (who assessed patients for eligibility) and the researcher responsible for delivering the treatment had no access to the content of the envelopes, ensuring the concealment of assignments. The patients and the therapist were not blinded to the treatment due to the nature of the study, as they knew which of the 3 devices was being applied, but the evaluator and data analyst were blinded.
Randomization was performed through a specific syntax for this study, in IBM-SPSS language (V22), in blocks and perfectly balanced by a statistician from the Ibero-American Cochrane Centre, Clinical Epidemiology and Public Health Service of the Hospital de la Santa Creu i Sant Pau. The randomization numbers were placed in sealed opaque envelopes, thus concealing allocation from both the patients and the therapist until treatment started. The envelopes were sequentially ordered from 1 to 135 and stored in a locked cabinet. Both the lead researcher (who assessed patients for eligibility) and the researcher responsible for delivering the treatment had no access to the content of the envelopes, ensuring the concealment of assignments. The patients and the therapist were not blinded to the treatment due to the nature of the study, as they knew which of the 3 devices was being applied, but the evaluator and data analyst were blinded.
Descriptive values are expressed as means and standard deviations (SD) for quantitative variables, and relative frequency for categorical variables.
As the main study analysis, a 2-way analysis of variance (ANOVA) was performed, with groups (3 levels: (groups I, II and III)) and time (5 levels (baseline and follow-ups) of repeated measures) as independent variables, and clinical variables (foot functionality, morning pain, pain during the day, and plantar fascia thickness) as dependent variables.
For secondary analysis with categorical variables a χ2 test was performed. Finally, in the case of quantitative variables, the inferential analysis was carried out with analysis of variance (ANOVA); the Kruskal–Wallis test was performed as a non-parametric test alternative to ANOVA (failure to meet assumptions or for ordinal variables).
The sample size was calculated using GRANMO Software (Version 7.12, IMIM-Hospital del Mar, Barcelona, Spain), with the assumption that an ANOVA would be performed among the 3 groups and 5 time-points. Accepting a p-value below 0.05 and a statistical power (beta-1 risk) above 0.8 in a bilateral contrast, 45 patients were required in each group to detect a minimum difference of 15 points between 2 groups, assuming that there were 3 groups and a standard deviation (SD) of 20. A maximum rate of 15% loss to follow-up was estimated.
Calculations were performed using IBM-SPSS (Version 22, IBM, Armonk, NY, USA).
A total of 135 patients participated in the study; 45 in each group. Mean age was 49 years, and 48% of the patients were women. Mean duration of symptoms was 14 months. Table II shows the baseline patient data.
Table II. Baseline data
In this clinical trial there was no loss to follow-up after the first, second and fourth months after intervention, but there were 7 patients lost to follow-up after the 14th month due to lack of interest or time constraints; hence 128 patients completed the study and were analysed.
The data showed no significant interaction effect be-tween treatment group and time for the FFI variable (F (6.857, 428.554)= 0.064; p = 0.863). However, there was a significant time effect (F (3.428, 428.554)=209.31; p < 0.001); that is, a significant decrease from baseline in all 3 groups. No significant differences were found among groups (main effect) (F (2,125)=0.196; p = 0.611). (Fig. 4).
Fig. 4. Foot Function Index (FFI) over time, by device group. Time factor p < 0.001; device factor p=0.863; device-time interaction factor p = 0.611. **The whole analysis was adjusted, correcting for age and sex of the patients, by means of a co-variance analysis (ANCOVA). The adjustment showed no change in significance with respect to the initial result.
For the VAS variable there was no significant interaction effect between group and time (p = 0.910). There was a significant time effect (p < 0.001), with a significant decrease from baseline assessment in all 3 groups. No significant differences were found among groups (main effect) (p = 0.623) (Fig. 5).
Fig. 5. Visual analogue scale (VAS) assessment of pain with the first weight-bearing step in the morning, over time and by device group. Time factor p < 0.001; device factor p = 0.910; device–time interaction factor p = 0.623.
For the VAS variable there was no significant interaction effect between group and time (p = 0.853). There was a significant time effect (p < 0.001), with a significant decrease from baseline assessment in all 3 groups. No significant differences were found among groups (main effect) (p = 0.599) (Fig. 6).
Fig. 6. Visual analogue scale (VAS) assessment of pain during the day, over time and by device group. Time factor p < 0.001; device factor p = 0.853; device–time interaction factor p = 0.599.
There was no statistically significant interaction effect between group and time (p = 0.402) for plantar fascia thickness. There was a significant time effect (p < 0.001); i.e. a significant decrease from baseline assessment in all 3 groups. There were no significant differences between groups (main effect) (p = 0.800) (Fig. 7).
Fig. 7. Fascia thickness over time and by device group. Time factor p < 0.001; device factor p = 0.402; device–time interaction factor p = 0.800.
No serious side-effects or complications were observed in any group. Adverse effects were increased heel pain in 19 patients and headache in 9 patients. These effects appeared after application of rESWT and resolved completely in 4 days without requiring treatment. No other adverse events were observed and no significant differences were found among groups (p = 0.473). Regarding the discomfort perceived by patients during the application of rESWT, there were no significant differences between groups (p = 0.660).
Broadly, the placebo and nocebo effects consist of an improvement or worsening of symptoms that is attributable to the context of the patient-therapist relationship. Therapeutic context includes a multitude of signals inherent to any intervention, which are perceived and interpreted by patients and generate positive or negative expectations (12). Placebo and nocebo effects can be generated from expectations (27–29); therefore it is important to assess contextual factors that can generate expectations and their impact on clinical outcomes. This RCT was designed to evaluate the influence of the appearance of a physical agent; in this case a rESW device, on clinical outcomes in plantar fasciitis.
It was found that, in the treatment of chronic plantar fasciitis with rESW, the appearance of the device did not significantly affect the clinical results. None of the 5 clinical variables analysed (foot function, pain with the first weight-bearing step in the morning, pain during the day, plantar fascia thickness, and adverse effects) showed statistically significant differences between the 3 groups: patients had similar results regardless of the treatment device (standard, sophisticated, or austere device). Furthermore, all patients improved significantly over time in relation to the baseline assessment. The improvement was observed equally in all 3 groups and at all assessment time-points: 1, 2, 4 and 14 months after the last rESWT session, with no statistically significant differences among groups over time. That is, the clinical outcomes were independent of the device used. Although the appearance of the device neither improved nor worsened treatment outcomes, as shown in this study, small differences were observed between the austere group and the other groups. The austere group obtained, in most evaluations, the worst clinical outcomes.
Despite an extensive neuroscience base that supports the placebo effect, there is a lack of clinical research that explores, in a healthcare setting, the context and placebo responses that accompany the overall therapeutic intervention. Most existing knowledge about the placebo effect has come from studies in basic science and clinical trials that are far removed from usual clinical practice. However, it has been found that placebo responses are greater under these conditions than in clinical trials conducted in real healthcare settings (21).
Few clinical trials have analysed treatment context factors, such as the appearance of a physical agent and its possible influence on patient recovery, making it difficult to compare the results of the current study with those obtained in similar studies. In a study conducted by Dawes et al. (30), 2 identical hearing aids were compared: 1 described as “new” and the other as “conventional”. Approximately 75% of the participants preferred the new device and reported that the hearing quality it provided was superior to the conventional one (30). Another clinical trial, with real patients, investigated the influence of different verbal information combined with a real analgesic drug (31) and reported similar results to the present study, showing no differences in pain reduction. Furthermore, in a crossover clinical trial, it was shown that the same person may respond differently to different types of placebo (placebo tablet or sham acupuncture). The response to placebo is a complex phenomenon that has many variables and goes beyond patient characteristics. This could explain the difficulty of detecting a pattern for people “responding to placebo” (32, 33).
The magnitude of the placebo effect depends on numerous design factors. A 2015 meta-analysis found that the type of active drug (opioid or non-steroidal anti-inflammatory drug (NSAID)), the scheduled follow-up visits (number of planned face-to-face visits), and randomization ratio (probability of receiving a placebo treatment, 1:4 or 1:1) were predictive of the magnitude of the placebo response, thereby supporting the expectancy hypothesis. Exploratory models showed that baseline pain intensity, age, washout length, and discontinuation due to adverse events accounted for approximately 10% of placebo response variability, and patients’ perception of treatment allocation and expectations toward treatment efficacy was strongly predictive of RCT outcomes (34). Nevertheless, most of the placebo effect is due to individual factors that are not yet well identified; hence, there is a growing interest in determining the individual factors that can predict the placebo response (35).
Patient expectations have been identified as one of the major components contributing to placebo responses. Patients requiring therapeutic interventions are exposed to stimuli in the clinical setting that trigger specific expectations about treatment and outcomes. These stimuli include the nature of the treatment itself, such as surgery, drugs, injections or therapeutic devices. They also include the characteristics of the clinician and the relationship formed with the patient, as well as the clinician’s confidence in the therapy and explanation of the treatment. The wider treatment context, such as the reputation of the facility and status of the clinic, may also affect treatment outcome expectations. These factors all operate psychologically and can enhance or diminish treatment efficacy (36).
The design of the current RCT allowed us to isolate and analyse the external appearance of the device as a contextual element of the placebo and nocebo responses. The strict inclusion and exclusion criteria allowed appropriate selection of patients with chronic plantar fasciitis, excluding patients with heel pain caused by other pathologies. The main clinical outcome, foot functionality, was assessed through the FFI, which has been proven as a validated and reliable instrument, and is one of the most-used tools in clinical trials on the effectiveness of plantar fasciitis treatment interventions (25, 26); the quality of this evidence has been rated as high (grade A recommendation by the American Physical Therapy Association) (37). A strong statistical power was reported; thus we can reasonably dismiss a type II error (or beta type error). In contrast to other studies, this study was carried out in a real healthcare setting, with patients rather than healthy volunteers. Other similar studies have used small samples and short follow-up periods (18, 36, 38), and were therefore less reflective of real clinical practice.
One limitation was the wording of the study. It was decided not to use the words “placebo effect” with the participants and this was not included in the informed consent form, because it could have confused the participants and made them mistakenly believe that there was a group without treatment. Another limitation of this study was the presence of the 3 devices in the same room, since in a real healthcare setting only a single device would be available. This could increase patients’ expectations and thus generate placebo or nocebo responses. This aspect might have been relevant for the external validity of the study, if differences had been found between the groups.
The current study may have some practical consequences. The results could encourage the industry to manufacture rESW devices with a more austere design, which would allow lower production costs. Therefore, equipment and treatment sessions would be cheaper, potentially increasing the number of patients who could access this therapy.
Creative experimental efforts are needed to rigorously assess the clinical significance of placebo and nocebo effects and investigate the individual elements that may contribute to a therapeutic benefit. Future research should place more emphasis on patient–therapist interactions rather than the diagnostic and therapeutic tools used. The placebo effect must be isolated from other phenomena present in clinical trials, such as the Hawthorne effect, natural fluctuations in diseases, and regression to the mean (20–22). These phenomena can cause confusion and lead to clinical improvements being wrongly attributed to a placebo effect.
In patients with chronic plantar fasciitis treated with rESW therapy, the appearance of the device did not influence clinical outcomes: function, pain with the first weight-bearing step in the morning, pain during the day, fascia thickness, and adverse effects. As device appearance did not affect treatment outcomes, it should not currently be considered as one of the contextual elements that generate placebo and nocebo responses. Further research is needed to identify the contextual variables, including patient-therapist interactions, which influence such responses.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize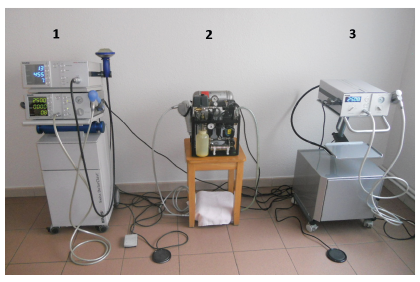 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize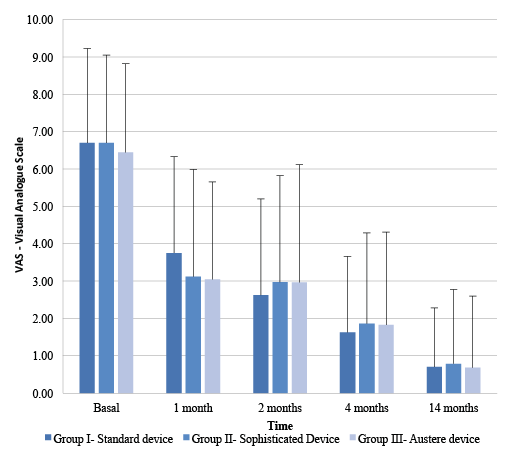 Click to show fullsize
Click to show fullsize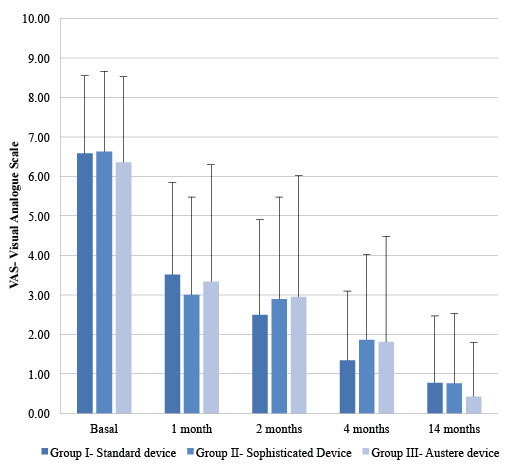 Click to show fullsize
Click to show fullsize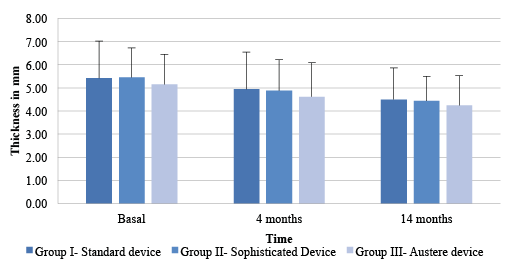 Click to show fullsize
Click to show fullsize