
From the 1Research Department, Rehabilitation Clinic “RehaClinic”, Bad Zurzach, and 2Institute of Psychology, University of Bern, Bern, Switzerland
Objective: To quantify and compare the course of health-related quality of life of immigrant native Italian-speaking and German-speaking patients before and after an interdisciplinary pain programme.
Design: Prospective cohort study with 1–12 month follow-up.
Subjects: Fibromyalgia, generalized widespread pain, and chronic non-specific back pain patients (Italian-speaking n = 96, German-speaking n = 199).
Methods: Score changes measured with the Short Form 36 (SF-36) were compared with multivariate analysis using standardized mean differences (SMD), adjusted for sex, education and the baseline score.
Results: At baseline, health of the Italian-speaking patients was worse than for the German-speaking patients. Adjusted SMDs showed significantly better improvements in the German group compared with the Italian group: SF-36 Physical functioning SMD = 0.54 (at discharge) and 0.49 (at 12 months), General health SMD = 0.71 and 0.44, Vitality SMD = 0.43 and 0.48 in one sample. In the other sample, the corresponding SMDs were 0.06 (discharge), 0.50 (3 months) and 0.47 (6 months) for Bodily pain.
Conclusion: State of health was better and health improvements were greater in German-speaking patients compared with Italian-speaking patients. Patients with a migration background may have special needs in therapeutic management, and addressing these might enhance the positive outcome in the short- and mid-term.
Key words: rehabilitation; interdisciplinary pain management programme; fibromyalgia; back pain; language; socio-cultural
factors.
Accepted Dec 7, 2018; Epub ahead of print Jan 22, 2019
J Rehabil Med 2019; 51: 00–00
Correspondence address: Thomas Benz, Research Department, Rehabilitation Clinic “RehaClinic”, Quellenstrasse 34, CH-5330 Bad Zurzach, Switzerland. E-mail: t.benz@rehaclinic.ch
This study examined the health of patients with
chronic pain who participated in a specific rehabilitation programme for chronic pain. Patients’ health was measured before participating in the programme, at the end of the programme, and after the programme. German-speaking patients were compared with Italian-speaking patients. Both groups participated in the same pain management programme with the same therapies, held either in German or in Italian. Italian-speaking and German-speaking patients improved immediately after the programme, but Italian-speaking patient reported lower improvements. The measurements after the programme showed that German-speaking patients could maintain the improvements, whereas the Italian-speak-ing patients lost the positive effects of the programme over time. In conclusion, Italian-speaking patients may have special needs in pain management and the level of acculturation may influence the results.
Chronic pain occurs in countries with different ethnic, racial, and cultural backgrounds, and has an adult prevalence of 19% in Europe (1). “Ethnic and racial differences” have been described for response to experimental pain, as well as for the perception, experience and treatment of pain (2, 3). Reasons proposed for ethnic differences in the prevalence of widespread pain include psychosocial or cultural differences, genetic predisposition, and the influence of physical or social environment (4, 5).
Interdisciplinary biopsychosocial rehabilitation for chronic low back and fibromyalgia reduces pain intensity, symptom impact, disability and improves functional capacity and work status (6–9). Based on a biopsychosocial treatment approach for chronic pain, interdisciplinary pain management programmes (IPMP) consider that pain, disability, and participation are not only the consequence of a biomedical cause (10, 11). Biological, psychological and social factors influence the development, course and maintenance of chronic pain (12, 13). These dimensions, as well as their interactions, are therefore, recommended to be an integral part of the treatment of low back pain and fibromyalgia (14, 15).
Social factors can be defined as “external facts and circumstances that influence and control an individual’s behaviour or attitudes related to pain”, e.g. language (16). Language difficulties may lead to misunderstandings relating to treatment intentions and decisions, advice given after therapy, the healthcare and insurance system, as well as educational treatment, and may not be sufficiently taken into account by the therapists. Social factors were shown to influence functional limitation and disability in low back pain, with social disadvantage being one of the important factors (16).
In Switzerland, the population with foreign citizenship has grown continuously since 1983 and had reached 24.6% of the total population by 2015. This is one of the highest percentages of foreign residents in Europe. In Switzerland, 84.7% of the foreign permanent resident population are of European origin, and the largest group of foreigners are Italian at 15.2% (17). Reactions to health-illness process are different in each culture and are influenced by the patient and by interpretations and attitudes that lead to a certain way of living with the disorder (18). More intercultural competence, awareness and culturally sensitive attitudes are required in medical treatment in order to meet the needs of these different groups better, e.g. by standardized IPMPs held in specific languages.
No studies have investigated the differences in changes as a result of the same IPMP with the same therapy components held in 2 different languages, administered by the same therapists. The objective of this study was to describe and to examine state (at baseline) and short-term (at discharge) as well as mid-term (at 3-, 6-, and 12-month follow-up) changes in biopsychosocial health and quality of life in Italian-speaking patients (ISP) with fibromyalgia, generalized widespread pain and chronic non-specific back pain before and after a standardized 4-week IPMP in the Italian language. Furthermore, the study aimed to compare the results of the ISP with the results of German-speaking patients (GSP) at follow-ups.
Patients included in this study were recruited at the pain centre of the rehabilitation clinic “RehaClinic” in Bad Zurzach, Switzerland. All patients with chronic non-specific back pain, fibromyalgia according to the American College of Rheumatology (ACR) definition (19), or generalized widespread pain (pain in all 4 body quadrants not fulfilling the ACR criteria of 1990 (19)) who attended the “Zurzach Interdisciplinary Pain Program” (ZISP) were invited to participate. Further inclusion criteria were age ≥ 18 years and chronic pain for ≥ 3 months. Exclusion criteria were severe somatic or mental illness/condition that prevented participation in the IPMP, insufficient language skills (reading and writing) to complete the assessment tool, and refusal to participate in the study or the IPMP.
Prior to inclusion in the IPMP and based on the admission report, potential participants were contacted by telephone by the programme leader (RB) or his assistant (both of whom are bilingual in German and Italian) to complete inclusion and exclusion criteria and to assess oral language skills (listening and speaking). Allocation to the groups was based on oral language skills and not on migration background. For example, all patients participating in the German-speaking programme had excellent oral German language skills, which were an inclusion criteria. Patients with insufficient oral German or Italian language skills (exclusion criteria) were admitted to a different, individual IPMP in our clinic.
Each group underwent a specific Italian- or German-speaking IPMP. This means that all information and instructions were given either in German or Italian. Both language-specific programmes consisted of the same therapy components, the same therapeutic content, and the same number of therapies. All
therapies in the programme were provided by the same therapists for the German, as well as for the Italian, group.
Written informed consent was obtained from all participants. The study protocol was approved by the Local Ethics Commission (Health Department in Aarau, Switzerland, EK AG 2008/026).
The ZISP is a 4-week, standardized, comprehensive, inpatient IPMP in groups. The IPMP focused on chronic musculoskeletal pain disorders and consisted of active physiotherapy, and aerobic endurance training, Qigong/tai chi exercises, individual psychotherapy including cognitive behavioural therapy, participation in a pain coping group, relaxation therapy, humour therapy, horticultural therapy (since April 2006), information and education about the pathophysiology of pain mechanisms and management of chronic disabling pain, nursing care, and regular medical consultations, including drug therapy. Details of the IPMP are provided elsewhere (6, 7).
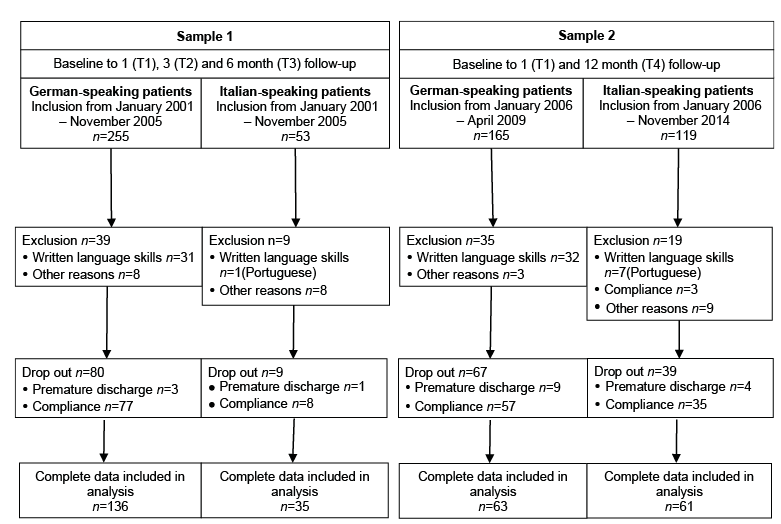
In this prospective cohort study, 2 different samples are described and analysed. Sample 1 was collected between 2001 and 2005 with follow-up measurements at 3 and 6 months (Fig. 1), sample 2 between 2006 and 2014 with follow-up measurements at 12 months. In 2006, the follow-up measurements at 3 and 6 months were replaced by one follow-up measurement at 1 year after entry to the programme. This decision was based on the findings for the GSP analysed in sample 1. In this study, only mid-term results were calculated (3 and 6 month follow-up) (6). In the following, long-term results came into our focus of interest, especially because these could not otherwise be found in the literature at that time. A further reason for the restart with the “revised” sample strategy (sample 2) of the IPMP was that a new, improved version (version 2) of the Medical Outcomes Study Short Form 36 Health Survey (SF-36) was available and included in the measurements (20).
For these reasons, the size of sample 1 was limited. The analysis based on sample 1 revealed relatively high effect sizes for many health scales (6). Thus, data sampling for sample 2 was considered sufficient after having reached n ≥ 60 for both the German- and the Italian-speaking group. Doubling the sample size up to n = 120 for each group would narrow the width of the 95% confidence interval of the effect sizes by 0.02. This gain was considered to be too small in face of the burden of doubling the sampling effort.
The difference in number of included patients in sample 1 and the difference in duration of inclusion of the patients in sample 2 were due to the naturalistic study design and the maximal capacity of 6 patients per treatment group in the ZISP. Only one group of patients was treated at a time. Twice a year, the programme was held in Italian for the ISP. This means that 2 groups with ISP and 10 groups with GSP were treated per year. This resulted in an unbalanced number of patients included in sample 1 with the same observation duration (Fig. 1). In order to obtain almost equal numbers of patients, different observation periods were chosen in sample 2.
Fig. 1. Flow chart of study participants.
Sociodemographic and potentially confounding parameters, such as age, sex, occupation, living conditions, sports, and formal education, were recorded at admission to the clinic on a standardized form used previously in many studies (6). Comorbidities were retrieved from the medical history.
The SF-36 comprehensively measures the dimensions of quality of life, physical, mental and psychosocial health (21). This instrument contains 36 items in 8 health domains: bodily pain, physical functioning, role physical, general health, vitality, social functioning, role emotional, and mental health. It is a commonly used measurement for the self-assessment of health-related quality of life in chronic pain diseases, such as fibromyalgia (22). It has already been used to assess the efficacy of interventions in rheumatology, physiotherapy, drug treatment, tai chi and many others (22). The validated German version was used for the GSP (23). In sample 1, version 1 (21) was used and in sample 2, version 2 (20). For the ISP, the validated Italian version was used (24).
Patients from sample 1 were assessed at baseline (T=0), discharge (T1; short-term), i.e. 4 weeks after entry, 3 months after entry (T2; mid-term), and 6 months after entry (T3; mid-term). Patients from sample 2 were assessed at baseline (T=0), discharge (T1; short-term), i.e. 4 weeks after entry, and 12 months after entry (T4; mid-term).
SF-36 scores were transformed into scales ranging from 0 (“maximal symptoms or limitation”) to 100 (“no symptoms or limitation”) to ease comparison of the descriptive data (25). The specific “missing rules” of the instrument had to be fulfilled for determination of the scales. This means that at least 50% of the items had to be completed for each of the SF-36 scales (25).
Sociodemographic and disease-relevant frequency data were compared by the χ2 test and continuous data by the non-parametric Wilcoxon test. Changes on the SF-36 scales between baseline and follow-up were quantified by multivariate standardized mean differences (SMD) (26). For each SF-36 score, stepwise multivariate linear regression was used to model the individual score changes (baseline to follow-up) as dependent variables. The same independent variables were used for all scales in both samples: group allocation (1=GSP, 0=ISP), baseline score, and sex and education (27). The last 3 variables are well-known as potential confounders for the score changes between baseline and follow-up. The number of confounders is limited by the number of patients in the smallest group/10 (28). The coefficient/slope of the group allocation variable was then equal to the adjusted score difference and was used to calculate the multivariate SMDs (26).
The SMD equals the difference of the mean score changes (baseline to follow-up) between the 2 groups (GSP and ISP) divided by the pooled standard deviation of the score changes (baseline to follow-up) of the 2 compared groups (26). The pooled variance equals the mean of the 2 score change variances, which is weighted by the number of patients. Intervals for 95% confidence (95% CI) for the SMD and t-test based type I errors (p) for testing SMD > 0.00 (zero outside of the 95% CI) were calculated (see Tables II and III). An SMD of 0.20–0.49 is considered small, 0.50–0.79 moderate, and ≥ 0.80 large (29).
All analyses were performed using the statistical software package IBM SPSS 23.0 for Windows® (SPSS Inc., Chicago, IL, USA).
The flow chart of participants is shown in Fig. 1. Complete data were available for analysis of 136 GSP and 35 ISP in sample 1, and 63 GSP and 61 ISP in sample 2. Reasons for exclusion with exact numbers are shown in Fig. 1.
Sociodemographic variables and disease-relevant characteristics are given in Table I. All participants were Caucasian. The mean participant’s age was comparable in both samples. Comparing sample 1 with sample 2, an important difference was found in sex, with no significant difference in sample 1, but in sample 2 more males participated in the study (p < 0.001). In education, ISP were significantly less educated than GSP, especially in sample 2. In sample 1, higher education was reported in GSP (73%) vs ISP (9%) in sample 1 and in sample 2 (62% vs 15%). Significant occupational differences were found in sample 1 (p < 0.001), with 80% of the ISP being unemployed. In sports, ISP were less active (p = 0.034). In both samples, most ISP were living with a partner. In sample 1, 66% of ISP had 3 or more comorbidities in contrast to 43% of the GSP. In both samples, this characteristic was comparable. In summary, ISP were less educated, less occupied, more often married and less active in sports than the GSP, especially in sample 1.
Table I. Sociodemographic and disease-related characteristics at baseline
Age, sex and SF-36 scores for completers were compared with the baseline scores of drop-outs for ISP and GSP in sample 1 and sample 2 each (i.e. 4 comparisons). No significant differences were found in all 4 comparisons in age and sex. In sample 1, significant differences were found in the GSP in Physical functioning (p = 0.034) and in the ISP in Role Physical (p = 0.032) and in Role emotional (p = 0.016). In sample 2, the only significant difference was in the GSP in Role emotional (p = 0.011). All other scores differences within the 4 groups were not significant.
At baseline, physical and psychosocial health for the ISP were worse than for the GSP in both samples, with the exception of less vitality and mental health in sample 1 (Table II) and less pain in sample 2 (Table III). However, the differences in the baseline scores were not statistically tested for significance because the baseline scores were included in the multivariate analysis as confounders.
Table II. Sample 1: SF-36 scores at baseline (T0), at discharge from the pain management programme (T1), at 3-month follow-up (T2) and 6-month follow-up (T3) of German- (n = 136) and Italian-speaking patients (n = 35)
Table III. Sample 2: SF-36 scores at baseline (T0), at discharge from the pain management programme (T1), and at the 12 month follow-up (T4) of German- (n = 63) and Italian-speaking patients (n = 62)
Immediately after the programme at discharge (T1), GSP improved on all scales in both samples. ISP improved on 7/8 scales in sample 1 and 6/8 in sample 2. However, the 3 negative score changes were very small (≥ –0.51 score points). In sample 1, the GSP improved most on Vitality (mean m=14.73), whereas the ISP improved most on Social functioning (12.54).
In the following course (T2, T3, T4), the improvements decreased slightly for the GSP but more markedly for the ISP with increasing time. For example, in Bodily pain, the score changes were 8.75 (T1)/8.92 (T2)/7.49 (T3) for the GSP, but 10.20/3.33/–1.00 for the ISP in sample 1. In sample 2, the corresponding score changes were 8.27 (T1)/8.22 (T4) for GSP and 7.51/2.25 for ISP. At the 6-month follow-up (T3), 8/8 score changes showed improvement in the GSP, while 5/8 showed worsening, and 2/8 showed no change in the ISP. At the 12-month follow-up (T4), 8/8 score changes showed improvement in the GSP, while 7/8 showed worsening in the ISP.
This led to increasing levels of SMDs during the course, since they quantify the differences of the score changes between GSP and ISP. However, adjustment for the confounders attenuated those differences during the course. For example, on Bodily pain, the observed score changes (listed above) led to bivariate, unadjusted SMDs of –0.093 (T1)/0.324 (T2)/0.429 (T3), but 0.055/0.502/0.465 multivariate, adjusted SMDs in sample 1. The differences on Bodily pain in sample 2 were not statistically significant; the adjusted SMD at baseline was –0.030 (p = 0.868) and increased to a SMD of 0.263 (p = 0.141). The same was true for Social functioning.
Significant change differences between GSP and ISP in sample 1 at each follow-up measurement were seen on the following scales: Role physical (adjusted SMD=0.572, 0.413, 0.404 for T1 to T3), Vitality (0.598, 0.577, 0.612), and Social functioning (0.408, 0.450, 0.371). In sample 2, Physical functioning (adjusted SMD = 0.543, 0.491 for T1 and T4), Role physical (0.531, 0.558), General Health (0.712, 0.441), Vitality (0.429, 0.479), and Role emotional (0.473, 0.473) showed significant differences.
In total, 5 of 8 SMDs were statistically significant (p ≤ 0.027) in both samples at discharge and at the 3-month follow-up. At the 6-month follow-up in sample 1, 7 SMDs (p ≤ 0.045) and at 1-year follow-up, 6 SMDs (p ≤ 0.012) were statistically significant.
Of the total of 8 health dimensions, 5 showed significant differences at discharge, 5 at the 3-month follow-up, and 7 at the 6-month follow-up in sample 1. In sample 2, the corresponding numbers were 5 (discharge) and 6 (12-month follow-up).
This study compared short- and mid-term changes in the biopsychosocial health and quality of life of ISP with GSP with chronic pain before and after a standardized IPMP. GSP improved in all measured scales at discharge and the effects remained almost stable in the follow-up measurements. In contrast, ISP showed less improvement on most scales at discharge and lost these positive effects completely over time.
These score change differences resulted in statistically significant adjusted SMDs on Role physical and Vitality, as well as, although somewhat less on General health over the course. At the mid-term follow-ups (6 and 12 months), all but one of the scales showed significant differences in favour of the GSP. These prominent differences cannot be explained by differences in therapy because both groups underwent the same structured standardized IPMP held in the specific language.
The main focus of the study was to explore possible differences between GSP and ISP. The naturalistic design of the study is one of the factors that led to baseline differences. The design of the study did not allow us to draw causal conclusions that explain the differences in the score changes of the 2 groups, the SMDs. Some cofactors may be found in the sociodemographic and disease-related characteristics (Table I), and some in parameters that were not assessed (e.g. sickness benefits from the insurance). Some can be found in existing literature: ethnicity including cultural, behavioural and attitudinal norms and systems of meaning (5, 30, 31) and socioeconomic level (4, 5) including educational level and work status. For the 3 most relevant confounders, sex, education and baseline score, analysis of the differences was adjusted by multivariate regression analysis. All 3 cofactors are well-known to affect and confound the outcome by epidemiological reasons and showed the biggest differences between the 2 groups at baseline. Even after correction of the unequal distributions of those 3 cofactors, substantial and statistically significant differences in outcome were observed between the 2 groups.
Although language has been described as “a proxy for acculturation” and as “a significant marker of cultural identity”, empirical data to support this are lacking (32). An improving knowledge of the German language in combination with an increasing length of stay in a German-speaking region is assumed to enhance the level of acculturation (33). This means that attitudes, values, customs, beliefs, and (health) behaviours are adapted to another culture and the influence of the origin culture diminishes (33–35). It can be assumed that migrants who have acquired high levels of language skills are also well acculturated in other cultural dimensions. Therefore, cultural differences within the German-speaking group of patients are thought to be small and of minor importance for health status and healthcare utilization, independent of migration status.
It has been suggested that disparities in pain among racial and ethnic minorities may be influenced not only by the patient, but also by the healthcare provider and the healthcare system (2). In Switzerland, healthcare insurance is mandatory and all patients have equal access to the healthcare system. Nevertheless, lower levels of acculturation and no German language knowledge influenced the accessibility and use of the healthcare system (36).
A comparable study examined Italian migrant workers (n = 36) and Swiss GSP (n = 49) with chronic low back pain (37). Both groups underwent an identical 3-month outpatient treatment programme in different languages. The levels of state and change in physical functioning were similar to those of our study. The Italian group showed no improvements in pain, disability, mental state, flexibility and strength after 3 months of treatment, while the GSP reported highly significant improvements in all measurements.
Consistent findings revealed 2 cross-sectional studies: Italian patients with chronic low back pain reported the highest levels of emotional impairment, second-highest levels of social impairment, and third-highest levels of physical impairment compared with different culture groups (38). Migrants from different countries, who lived in Switzerland for longer had worse health than indigenous Swiss people of the same age (36).
In our data, important improvements in various health dimensions were observed at discharge after intensive inpatient treatment of GSP and ISP. Improvements in ISP were lower and in some health dimensions even negative (worsening). Most of the short-term improvements were maintained up to mid-term (6 or 12 months) in GSP. In contrast, ISP lost almost all of these improvements. This loss might be caused by some of the complex interactions mentioned above. Chronic pain can be initiated and increased by psychological distress caused by perceived discrimination (39). One possible interpretation is that the special needs of patients with a migration background may partially be met within an inpatient IPMP held in their native tongue, but are not generally met at home after discharge. At the end of the programme all patients receive individually tailored recommendations for subsequent outpatient management irrespective of the language.
The differences in outcome between GSP and ISP in this study cannot be explained by differences in the language-specific programmes, since all therapies and therapist were the same for both groups. Differences in effects cannot be attributed to therapeutic characteristics or comprehensibility. Inequalities in baseline characteristics, which were (Table I) or were not assessed in the study, are superficial. In addition, heterogeneities of characteristics within the fibromyalgia syndrome and back pain may have an impact. Knowing these factors, higher sample sizes would be needed to adjust for them.
Reducing language barriers by administering the treatment in Italian language seems not to be sufficient, because the improvements observed in the Italian group were smaller than those of the German group. In addition to language barriers, cultural barriers have been shown to have a negative impact on the recovery process (35): “Cultural differences may result in diverging and conflicting representations of health, illness and therapy, and this may hinder the healing process or even cause its failure”. Four mediating factors in intercultural care have been identified to facilitate or hinder the care relationship and, by that, the rehabilitation process: (i) humanity in care, (ii) communication, (iii) the role of the family, and (iv) the hospital’s organizational culture (40). Adapting the therapy content in combination with specific intercultural competence training of all involved medical personal might enhance the treatment effect in the IPMP by implementing a comprehensive “cultural sensitive care in which patients are cared for in a holistic and dignity-enhancing way” (40).
For detailed insight into these complex clinical situations, various factors should be further investigated: (i) influence of migration details (e.g. migration background, migration trajectories), (ii) level of acculturation (language skills among other factors), (iii) identification of key aspects of intercultural competence and communication in different care settings and health professions, (iv) adaptation of methods and content of treatments, (v) definition of health and pain, particular needs and specific expectations from a patient’s perspective, and (vi) choice of assessments to measure change of main problems of these patients.
This study has several weaknesses. There was a lack of detailed information about socioeconomic status and migration information, including land of origin, place of birth and reasons for migration. Socioeconomic status was approximated by education and occupation level. The high number of patients lost to follow-up is a potential threat to the internal and external validity of this study. However, sensitivity analysis showed rare differences in baseline characteristics between the subjects who completed the study and those who dropped out during observation time. This means, that selection bias due to sex, age and SF-36 baseline score differences was small. A further weakness is the lack of knowledge about the treatment during follow-up periods after discharge. Continuation of the recommended therapies after dismissal was not assessed. Although both versions of the SF-36 have been derived from and validated to the English original, cross-validation between the German and Italian version has not been performed. Psychometric differences between the 2 versions may exist and contribute to the differences of the outcome measurement.
A strength of this study is the naturalistic, prospective study design with comparison of 2 groups participating in the same IPMP with the same therapy components in different languages. ISP received the same therapies as the GSP in their own language. A further strength is the consistency of the differences across 2 different samples. Although the observational, non-randomized study design without a control group did not permit a causal statement on the effectiveness of the treatment, quantification and comparison of changes in health were possible. The differences in changes in health between the 2 groups were adjusted by cofactors that were unequally distributed at baseline and which possibly confounded the outcome changes.
In conclusion, ISP reported lower improvements in state of health after an IPMP than GSP. In the subsequent follow-ups, these differences were further accentuated. The reasons for these differences remain unclear, but may have consequences for the future management of ISP in IPMPs. Patients with a migration background may have special needs in therapeutic management and addressing them might enhance the positive outcome in the short- and mid-term.
The authors thank all patients for participating in the study and the members of the Pain Center of the rehabilitation clinic “RehaClinic” in Bad Zurzach, Switzerland. We would also thank Joy Buchanan and Stacy Müller for English editing. The authors received no financial support for the research, authorship, and/or publication of this article.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize