
From the 1Department of Health and Care, Arctic University of Norway, Tromsø, 2North Norway Rehabilitation Center, Tromsø, 3Sunnaas Rehabilitation Hospital, Nesodden, 4Department of Coaching and Psychology, Norwegian School of Sport Sciences, Oslo, Norway, 5Department of Epidemiology and Biostatistics, Loma Linda University, Loma Linda, CA, USA, 6Department of Clinical Therapeutic Services, University Hospital of Northern Norway, Tromsø, and 7Department of Cardiology, Oslo University Hospital Ullevål and Institute of Clinical Medicine, University of Oslo, Oslo, Norway
Objective: To assess the effects of manually assisted body-weight supported locomotor training in subjects with chronic incomplete spinal cord injury.
Design: Randomized controlled clinical trial.
Subjects: Twenty subjects with American Spinal Injury Association Impairment Scale grades C or D and > 2 years post-injury.
Methods: Random allocation to 60 days of body-weight supported locomotor training, or usual care, which might include over-ground walking. Walking function, lower extremity muscle strength and balance were blindly evaluated pre-/post-intervention.
Results: A small, non-significant improvement in walking function was observed (0.1 m/s (95% confidence interval (95% CI) –0.2, 0.4)), but subjects without baseline gait function, did not re-establish walking. The effect on lower extremity muscle strength was 2.7 points (95% CI –1.4, 6.8). No difference was observed in balance measures.
Conclusion: Subjects with chronic incomplete spinal cord injury without baseline walking function were unable to re-establish gait with manually assisted body-weight supported locomotor training. A modest, non-significant, improvement was found in strength and walking speed. However, due to study recruitment problems, an effect size that was smaller than anticipated, and large functional heterogeneity among study subjects, the effect of late-onset body-weight supported locomotor training is not clear. Future studies should include larger numbers of subjects with less functional loss and greater functional homogeneity. Intensive training should probably start earlier post-injury.
Key words: spinal cord injury; locomotor training; body-weight support; treadmill.
Accepted Oct 23, 2018; Epub ahead of print Nov 28, 2018
J Rehabil Med 2019; 51: 00–00
Correspondence address: Anu Piira, North Norway Rehabilitation Center, Conrad Holmboes veg 95, NO-9011 Tromsø, Norway. E-mail: anu.piira@kurbadet.no
This randomized clinical trial assesses the effects of manually assisted body-weight supported treadmill training in patients with chronic functionally incomplete spinal cord injury acquired > 2 years earlier. Due to recruitment challenges, it was only possible to recruit two-thirds of the planned number of study participants. The intervention group received gait training 5 days per week over 12 weeks, and the control group received usual care with their local physical therapist. Subjects with no baseline gait function did not regain walking ability. Compared with the control group, the intervention group showed modest improvements in walking speed, lower extremity strength, and body control. However, all between-group differences were non-significant. Because the target number of study participants was not reached, the study was underpowered and non-significant, and thus the findings are inconclusive. It does, however, seem that this training method has benefits, but it is labour-intensive and requires large amounts of human resources.
Body-weight supported locomotor training (BWSLT) has been used to retrain walking func-tion after spinal cord injury (SCI) after experimental SCI in animals (1) and in uncontrolled human clinical studies (2–8). Both older (2, 3) and more recent studies (4–8) have reported encouraging results. Locomotor gait training increased muscle volume (7), improved activation of muscles in the lower limbs (9), increased ankle stability (10), and was associated with decreased spasticity (11). There is also some evidence that BWSLT improves subjects’ wellbeing and quality of life (6), and the benefits seem to be sustained (12). A 2017 review concluded that, so far, locomotor training has not proven more effective in restoring walking speed and distance walked than the same amount of conventional gait training in patients with SCI (13).
Spontaneous improvement in SCI can occur up to 2 years post-injury (14), blurring the effects of training in studies in the early post-injury phase. Such an effect attenuation may explain the null findings of a large multicentre randomized controlled trial (RCT) (n = 146) with subjects enrolled 8 weeks after injury (15). On the other hand, early intervention may be more effective than a later start. In spite of methodological differences, there seems to be consensus that early gait training in motor incomplete SCI improves over-ground walking independently of the training method (15). This also seems to hold true for patients with chronic incomplete SCI (> 1 year post-injury) (7).
Uncertainty exists, however, as to whether patients with incomplete SCI with more severe functional deficit also benefit from such training, because patients without walking function before training are frequently unable to walk independently after intervention (5, 6, 13).
The aim of the present study was to evaluate the effects on physical function of BWSLT with manual assistance compared with usual care, in subjects with chronic incomplete SCI (2+ years post-injury) and severely reduced or no gait function, classified by the American Spinal Injury Association (ASIA) Impairment Scale (AIS) as grade C–D (16).
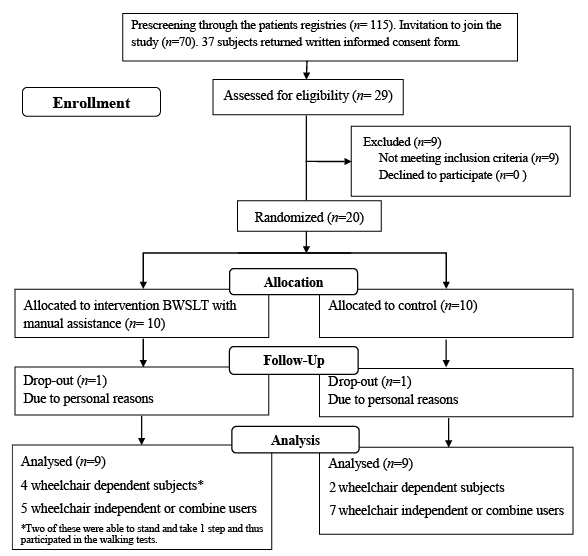
A single-blinded RCT was conducted in collaboration with the 3 Norwegian SCI rehabilitation units in order to investigate the effect of BWSLT with manual assistance in subjects with incomplete SCI who lived outside the Norwegian capital Oslo (where another study was recruiting SCI subjects). Fig. 1 shows patient flow through recruitment, assessment, intervention and follow-up.
Subjects in the control group received usual care from their local physical therapist. Physical therapy sessions varied in frequency and, for some, included merely passive movement of the joints in the lower extremities and stretching, whereas more than 50% of subjects also had some sessions with over-ground gait training and independent training in the gym. Their daily activities and training were recorded in a diary that was submitted monthly, and subjects received follow-up telephone calls and were advised not to change their training programme/leisure-time physical activities during the study.
A treadmill with body-weight support system (Vigor Equipment, Inc., Stevensville, MI, USA) was used for 60 days training, with 2 daily sessions of BWSLT with manual assistance for a total of 90 min per day, 5 days per week during 3 periods, each of 4 weeks. The duration of each training session depended on each subject’s endurance, ability to maintain correct movements in the lower extremities and ability to maintain normal walking rhythm. The aim was to reduce the body-weight support to < 40% and/or increase walking speed towards normal (3–5 km/h). Lower-limb braces or orthoses were not allowed during BWSLT, and there was minimal use of handrails for support. A mirror placed in front of the subject provided visual feedback during training. Each training session involved a team of 3–5 persons to facilitate movements of the pelvis and legs. Subjects received soft-tissue mobilization/stretching before and after each session to prepare for training and reduce spasticity. BWSLT also included over-ground training. The subjects were given home exercises for use between the training periods, selected to improve carry-over of learned skills from treadmill to the community environment. Data from each training session were recorded in an Excel file.
Subjects were recruited from the 3 SCI units in Norway through advertisements in national magazines for persons with SCI. The Regional Committee of Ethics (REK) in North Norway approved the study (P REK NORD 69/2008) (ClinicalTrials.gov identifier #NCT00854555). All potential study subjects gave their written informed consent before final evaluation for inclusion. The inclusion criteria were age 18–70 years and motor incomplete SCI classified as AIS C–D, with a minimum of 2 years since injury. Subjects should primarily be wheelchair dependent with or without some walking ability, have body mass index (BMI) < 30, be cognitively unaffected and motivated for locomotor training. Exclusion criteria included spasticity and contractures that inhibited locomotor training, known osteoporosis in the lower limbs, pregnancy, participation in other intensive training programmes, medical conditions that might interfere with the training protocol, and previous knee or hip replacement. Subjects were encouraged not to change their anti-spasticity medication during the study period.
Assessments before and after the intervention or control period were conducted single blindly at Sunnaas Rehabilitation Hospital outside Oslo. The in-patient intervention site was North-Norway Rehabilitation Center, Tromsø.
Randomization was concealed. Allocation to intervention (I) or control (C) groups was performed by the sealed envelope method, in blocks of 10. The project coordinator prepared the sealed envelopes and a staff member, who was not involved with the study, selected an envelope for each subject and informed the project coordinator on the allocation.
Evaluation and testing were carried out prior to randomization, within the last month before start of the intervention/control period. Post-evaluation took place 2–4 weeks after the final intervention/control week. The assessors (physicians and physical therapists) were blinded to each subject’s group allocation.
All primary outcome measures used are common in neurological and SCI rehabilitation: (i) change in over-ground walking speed; (ii) distance walked with use of necessary walking aids; and (iii) lower extremity motor score (LEMS), a subscale in the ASIA classification that assesses muscle strength. The score range is 0–5 for each of 5 key muscles (hip flexors, knee extensors, ankle dorsi-flexors, long toe extensors and ankle plantar flexors) of each leg, with maximum score of 50 (16).
Walking speed was assessed with the 10-m walk test (10MWT), where subjects are asked to walk 10 m as fast as possible with a flying start (17). The mean time of 2 tests was recorded. Endurance was measured by the 6-min walk test (6MWT), where the distance walked within 6 min is measured (17).
Secondary outcomes were change in balance and aerobic capacity. Berg’s balance scale (BBS) was used for dynamic balance test, and the Modified Functional Reach test (MFR) for postural control. The quality of performance on each of the 14 tests is recorded using a 4-point scale (maximum score 56 points) (18, 19). Higher scores indicate better balance. The MFR assesses postural control in the sitting position in subjects without independent standing ability (20). Aerobic capacity was tested on an arm crank ergometer (Lode Angio, Groningen, the Netherlands) and breath-by-breath spirometer (Vmax 220 Sensormedics Corp., USA): stepwise, graded exercise until exhaustion. Maximal oxygen uptake (VO2max) (l/min) was recorded by a computerized standard open-circuit technique breath-by-breath spirometer.
Sample size. It was estimated that 30 subjects (15 subjects in each group) were required to obtain a statistical power of 0.80 with alpha error 0.05 for primary outcomes. The calculations were based on the expected differences between intervention and control groups obtained from primarily our own pilot study (unpublished) and, to a lesser degree, on published literature (15, 21). The expected training improvements, e.g. differences in change between the intervention and control groups, were 0.5 m/s (SD 0.6) in 10MWT, 55 m (SD 40) in 6MWT, and 15 points (SD 7) in BBS.
The main analysis compared mean or median changes from baseline to final evaluation. Comparison of baseline values between the 2 groups was done using χ2 test/Fisher exact test for categorical variables and independent samples t-test (2-tailed test with significance level p < 0.05). For non-normally distributed data, the Mann–Whitney test was used. Paired samples t-test or Wilcoxon signed-rank test was used to analyse change within groups. The difference in change between the 2 groups was assessed using linear regression. The data was analysed with the 23rd version of SPSS for Windows (IBM SPSS, Armonk, NY, USA). Because of low numbers, the intervention and control groups were imbalanced on several parameters at baseline. Therefore, multivariable analyses adjusting for a priori selected variables potentially related to treatment effect were also carried out (Table SI1).
As shown in Fig. 1, only 20 of the planned 30 study subjects were recruited within a reasonable timeframe. Based on search of the medical records from the 3 SCI units in Norway, 115 potential participants were identified based on injury type, time of injury, functional level and age. In addition, some subjects contacted project workers directly as a result of information they had obtained from advertisement campaigns. These subjects were pre-screened for eligibility through a phone call. A total of 70 subjects who met the inclusion criteria, were invited to join the study and, of these, 37 returned the written consent form. Eight of the 37 did not attend the clinical pre-screening, leaving 29 subjects who completed the full screening procedure at Sunnaas Hospital. However, nine subjects did not meet the inclusion criteria and thus 20 subjects were randomized.
Fig. 1. CONSORT (Consolidated Standards of Reporting Trials) flow diagram of participants.
The training intervention was well tolerated with no adverse events, and there were only minor side-effects, such as superficial abrasions, which did not interfere with the regular training programme. Baseline data on the study subjects are shown in Table I. Some differences and potential imbalances in baseline levels of outcome variables are seen between the groups in strength, distance covered, walking speed, balance and aerobic capacity (Table II). Detailed BWSLT data were recorded daily for each person in the intervention group, and are summarized in Tables III and IV.
Table I. Baseline demographics of study subjects according to intervention or control group
Table II. Outcome measures at baseline
Table III. Body-weight supported locomotor training data from the intervention group, n = 9
Table IV. Mean change in walking distance and walking speed on the treadmill from first to last training session
In each group, 2 subjects with AIS grade C (22%) were unable to walk at baseline, and did not gain independent walking post-intervention. Thus, only 7 subjects in each group, those with some ambulatory function at baseline, were available for post-intervention testing of walking speed (10MWT) and distance covered (6MWT). Fig. S11 shows individual changes in walking speed (10MWT) and distance covered (6MWT) in each group.
Both groups walked faster (10MWT) at post-test. However, the difference between the 2 groups was small (0.1 m/s (95% CI –0.2, 0.4)), and not statistically significant.
Endurance (distance walked), as measured by the 6MWT, improved approximately the same amount in both groups; the standard deviations were very large and there was no significant difference between the groups (–4.3 m (95% CI –52.7, 44.1)) (Table V). One subject was unable to walk due to pain in his lower limb, thus we were only able to repeat the 6MWT in 6 subjects in the control group.
Baseline range in LEMS was similar in the 2 groups, 6 to 46 and 8 to 40 points in the intervention and control groups, respectively. In the intervention group, LEMS increased by a mean of 2.1 points (SD 2.8, p = 0.05), whereas there was little change in the control group (mean change –0.6 (SD 5.1), p = 0.75). The difference in mean changes between the groups was 2.7 (95% CI –1.4, 6.8, p = 0.19) (Table V).
Table V. Changes in walking speed and walking distance, strength, balance, aerobic capacity, from baseline to evaluation 2–4 weeks post-intervention/control period
As part of the statistical plan, a few a priori variables were selected for possible adjustment in the final analyses. Because of the small numbers, the intervention and control groups were imbalanced with respect to baseline levels of some of these a priori selected variables. Adjustment by multivariable linear regression did not change the main results (Table SI1).
Changes in balance, as measured by BBS and MFR, are shown in Table V. There was no significant difference in change between the groups for either outcome, –1.2 points 95% CI (–4.3, 1.9), p = 0.42 and 6.6 cm (–5.4, 18.5), p = 0.26, respectively, for BBS and MFR (Table V). There was no significant change in VO2 measurement in any group, nor in the difference between them ((0.0 l/min, 95% CI (–0.2, 0.3), p = 0.87)) (Table V). However, for the VO2 test there were small numbers of subjects, since 2 subjects missed the baseline testing, and 3 were unable to perform the post-test due to technical problems.
To the best of our knowledge, the present study is the first RCT to include only subjects with longstanding incomplete SCI (AIS C and D), > 2 years post-injury, i.e. when spontaneous improvement is no longer expected. In addition, the study included a control group that received usual treatment. The treatment effects were modest, and not statistically significant.
There are a number of previous RCT training studies in SCI (13). However, they merely compare various training forms without a control group receiving the non-intensive training that is usual at this stage post-injury. In the present context, these studies must therefore be regarded as observational, presenting the sum of spontaneous improvements and true training effects. Only one non-randomized study from 1995 has a control groups similar to ours (3). The positive results of this study sparked interest in conducting training studies, but the findings have not been replicated. A large observational multicentre study recruited 146 patients early after SCI (8 weeks post-injury). The patients were unable to walk, or needed assistance to ambulate (15). Similar to our study, authors report measured, but not statistically significant, improvement in walking speed. A meta-analysis of the effects of training is inconclusive (13), but methodological issues complicate comparison of the studies. In general, uncontrolled studies achieve better results, probably due to spontaneous recovery, assessors’ bias etc. (2–6).
The majority of subjects in the current study had some walking function at baseline, and both their walking distance and speed increased or were maintained in the intervention group. However, the improvements were modest. The small improvement in walking speed (0.1 m/s) may, however, be clinically relevant (15, 22), but this is uncertain, since a walking speed of at least 0.44 m/s is required for community walking (7, 22, 23). A minimum of 46 m (22) or 31 m (13) increase in the 6MWT is considered clinically meaningful, but the improvement in both of the groups in the current study was smaller.
In line with this research, most previous studies report small effects. Some found increased walking speed of magnitude similar to the current study (0.2 m/s increase for the intervention group) (4, 5, 7, 13), 2 studies report greater (6, 24), and 2 somewhat poorer improvement (8, 21). On average, our subjects improved distance walked/endurance by 25 m, comparable to the findings of 2 other studies (8, 21). Two studies have reported better results among those with post-injury time from 8 weeks to < 3 years (5, 15) and 1 reports poorer improvement (24).
Similar to 3 observational studies (5, 6, 21), subjects in the current study who were unable to establish walking function, had poorer baseline neurological status (5, 6, 21) and balance (5) than the rest of the group. On the other hand, and in line with previous findings (5, 6, 21), subjects in the current study with the weakest walking function tended to make the largest percentage improvement.
Lower extremity muscle strength can predict walking function in subjects with SCI, and scores of 30 or more are common in subjects with functional/community walking ability, whereas scores < 20 are associated with poor walking ability (7, 25, 26). LEMS improved 2.7 points more in the intervention group than among controls (not significant). Several studies have shown that BWSLT improves lower limb strength in subjects with SCI (3, 7, 8, 15, 21). Two studies (4, 21) report improvement of similar size as in the present study, whereas another study (7) found as much as 9.1 points improvement in LEMS in the BWSLT group vs 2.9 points reduction in the physical therapy group, possibly due to early onset of training and better baseline function. In contrast to our study, others have found that those with higher baseline LEMS experience most improvement in walking speed (7, 25, 26). An improvement of > 6 points in LEMS may be needed to detect a significant clinical change. It is thus questionable whether the present small, borderline significant improvement in LEMS contributes to subjects’ walking ability. However, it is possible that BWSLT can improve postural stability in standing and sitting positions, through increased muscle strength and coordination. The clinical importance of the current findings seems to be modest, but even a small improvement may be important to an individual who struggles to cope with activities of daily living (5, 13).
We chose to study subjects with poor baseline walking function since data on their training effects are scarce. Previous studies included no, or only a few, subjects who were unable to stand or to move at least 1 step (4, 7, 15). In the large observational study the majority of non-responding subjects were among those with poor baseline function (5). However, in addition, a large proportion (13 of 19 AIS D and 15 of 50 AIS C) who were unable to ambulate at baseline, had regained some walking function at the final evaluation (5). Thus, poor baseline function does not preclude benefit, but training is perhaps most useful for those who can already walk a little (4, 5, 7, 8).
In 3 trials with early enrolment (≥ 7 months, 9–11 months or 1+ years post-injury) walking ability improved significantly (7, 8, 24). Yang et al., studying 22 participants with post-injury time ≥ 7 months, found significant 27-m improvement in distance walked in the BWSLT group (focus on endurance training), similar to our findings, compared with 10 m in controls (precision training) (8). Harkema et al. report the greatest improvements among those recruited ≤ 1–3 years post-injury, compared with later onset of training, whereas training initiated > 3 years post-injury, resulted in less functional improvement (5). Findings among the group with longest post-injury time were similar to our results. Several of our subjects were included even later than this. Interestingly, some have also reported good results with training starting several years after SCI (21). BWSLT should possibly start earlier, but then spontaneous recovery of function is frequent, and a much larger study is required to account for large variations (27).
Balance control scores were below 45 at baseline, indicating poor balance (18), and did not improve. Some (3, 5, 21), but not all BWSLT studies (7), show improved balance. Falls and fall-related injuries are well-known complications after SCI (28), and improvement gained in truncus stability and balance after BWLT could contribute to the prevention of such events.
In spite of the training, there was no improvement in maximal oxygen uptake. Alexeeva et al. (7) reported similar findings. The negative findings are, however, not surprising because testing was done with arm crank cycling, while training was directed at legs and trunk.
The present training protocol was conventional. We doubt whether patients would tolerate more intense or longer training, and this was also limited by available resources. Furthermore, recently no correlation was found between training dose and outcome in various gait training protocols (29). However, increasing the amount of over-ground training could be considered (4, 15, 24).
This study has several strengths. The single-centre study design reduces method variation, and the single-blind design reduces evaluation bias. Post-injury time >2 years reduces spontaneous improvement, allowing a lower number of study subjects. The main weakness is the slow rate of patient recruitment, which forced us to close the study when only two-thirds of the target patient number was reached. Post-hoc analysis revealed that, assuming better balanced groups, we would need a study size between 76 and 208 participants to detect significant improvements. Thus, the study was statistically underpowered, resulting in unbalanced groups at baseline (Table I), and a low probability of detecting modest improvements. The number of eligible and willing subjects was overestimated. Due to our 2-year post-injury requirement, some subjects had adapted well, and were reluctant to invest time, travelling and efforts on a project with an uncertain outcome. Another limitation is that we relied on usual care for the control group. At least 2 control subjects increased their training during the trial, attenuating the effect size of the intervention. Also, the majority of the control group had over-ground gait training as part of their regular physical therapy. Despite the limitations of the present study, our experience illustrates the complexity of conducting such clinical research.
BWSLT with manual assistance was well tolerated, and led to statistically non-significant improvements in walking and lower extremity muscle strength. The present results neither prove nor disprove the efficacy of this training, but suggest that the benefit is, at the best, modest in patients with poor function long after injury. Future research should include a higher number of participants and use block randomization based on function.
Several factors made this study possible: healthcare, including rehabilitation, is free of charge in Norway, allowing subjects to receive inpatient rehabilitation; the 3 primary rehabilitation centres for SCI in Norway all contributed to patient recruitment; and the project was supported financially both by the government and non-governmental institutions (the Norwegian Health Authorities and Norwegian Health and Rehabilitation funds). This study was initiated by 2 patient organizations (LARS – National association of the spinal cord injured and LTN – National association of the traffic injured) and could not have been completed without their continuous help and involvement throughout the study. The efforts of staff, who guided the locomotor training in Tromsø, are highly appreciated, as well as the testing team at Sunnaas Rehabilitation Hospital.
Study funding. The study was funded by the Norwegian Health Authorities and Norwegian Health and Rehabilitation Funds.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize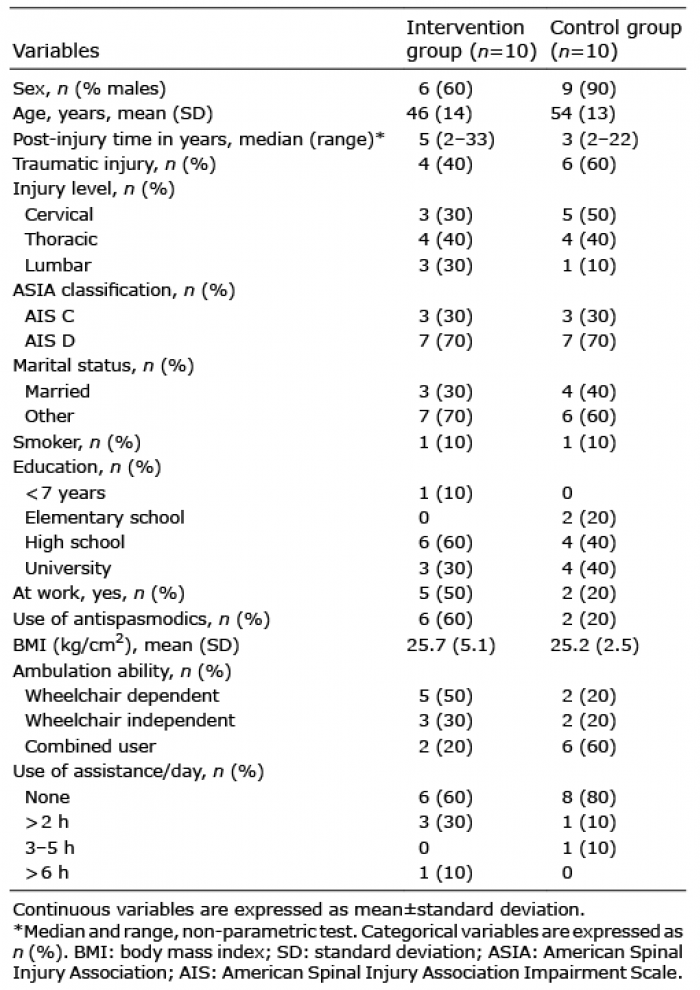 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize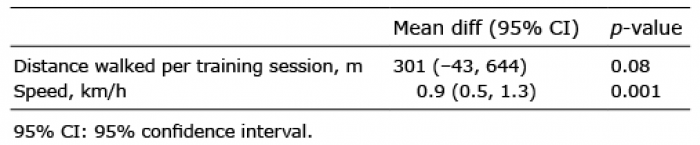 Click to show fullsize
Click to show fullsize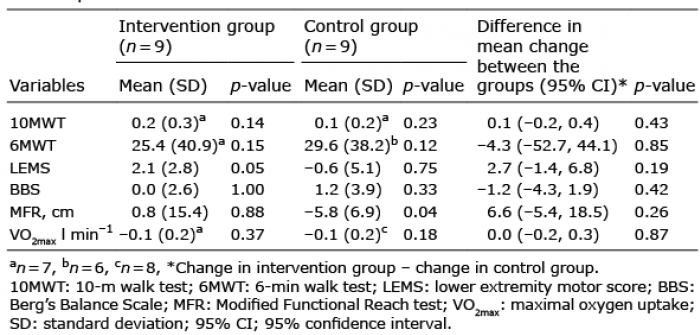 Click to show fullsize
Click to show fullsize