
From the 1Department of Physical Medicine and Rehabilitation, Dong-A University College of Medicine, Busan-Ulsan Regional Cardiocerebrovascular Center, Dong-A University Hospital, Busan, and 2Department of Physical Medicine and Rehabilitation, Daejeon St Mary’s Hospital, College of Medicine, The Catholic University of Korea, 64 Daeheung-ro, Jung-gu, Daejeon, Republic of Korea
Objective: To investigate the therapeutic effects of mechanical inspiration and expiration exercise using mechanical cough assist on velopharyngeal incompetence in patients with subacute stroke.
Design: Pilot, randomized controlled study.
Setting: University-based rehabilitation centre.
Subjects: Thirty-six patients with subacute stroke diagnosed with velopharyngeal incompetence by videofluoroscopic swallowing study.
Methods: Subjects were randomly assigned to 2 groups. The study group received conventional dysphagia therapy and additional mechanical inspiration and expiration exercise. The control
group received conventional dysphagia therapy only. Swallowing function was evaluated according to the American Speech-Language-Hearing association scale, functional dysphagia score, and the penetration aspiration scale, based on the videofluoroscopic swallowing study. Coughing function was measured using peak cough flow.
Results: Eighteen patients in each group completed the protocol and were analysed. After treatment, the study group showed significant improvement in functional dysphagia score with regard to nasal penetration degree. Comparing the treatment effect between the 2 groups, nasal penetration degree and peak cough flow showed greater improvement in the study group.
Conclusion: Mechanical inspiration and expiration exercise had a therapeutic effect on velopharyngeal incompetence in subacute stroke patients with dysphagia. This therapy is easy to provide clinically and could be a useful therapeutic strategy for velo-pharyngeal incompetence with dysphagia in patients with stroke.
Key words: stroke; velopharyngeal incompetence; mechanical inspiration and expiration exercise; videofluoroscopic swallowing study; deglutition disorders.
Accepted Oct 23, 2018; Epub ahead of print Nov 14, 2018
J Rehabil Med 2019: 51: 00–00
Correspondence address: Sook Joung Lee, Department of Physical Medicine and Rehabilitation, Daejeon St Mary’s Hospital, College of Medicine, The Catholic University of Korea, 64 Daeheung-ro, Jung-gu, Daejeon 34943, Republic of Korea. E-mail: lsj995414@hanmail.net
Dysfunctional swallowing and coughing are common after stroke. These functions are closely related as they both use the same expiration-related muscles. Velopharyngeal incompetence (VPI) is one of the symptoms of swallowing and coughing dysfunction. However, there have been few studies regarding treatment of VPI. This study investigated the therapeutic effects of mechanical inspiration and expiration (MIE) exercise, using mechanical cough assist, on VPI in subacute stroke patients with dysphagia. The degree of nasal penetration and peak cough flow were improved to a greater extent in patients in the MIE exercise group. MIE exercise was effective on both swallowing and coughing function. This therapy is easy to apply in the clinical setting. Thus, MIE exercise may be a useful therapeutic strategy for VPI with dysphagia in patients with stroke.
After a stroke, many patients experience swallowing and coughing dysfunction. The reported incidence of post-stroke dysphagia ranges from 37% to 64%, and it is one of the most common and serious clinical symptoms during the acute stage (1, 2). Complications of dysphagia include dehydration, malnutrition, aspiration pneumonia, and asphyxia, all of which may be fatal (3, 4). Coughing is an important protective mechanism for maintaining a clear airway. Several studies have revealed that stroke patients can experience a decrease in coughing function (5–7) and decreased coughing may be a predictive factor for aspiration pneumonia after stroke (7–9). Cough function is closely related to swallowing function and plays an important role in airway protection after stroke, since afferent and efferent pathways of the cough reflex are shared with that of the swallowing reflex (9, 10).
Previous studies of post-stroke swallowing or coughing dysfunction have focused exclusively on food aspiration or aspiration pneumonia (3, 6, 7, 11). However, there are various clinical manifestations of dysphagia after stroke apart from aspiration, including oral, pharyngeal, and oesophageal phase disorders. Therefore, early detection of dysphagia and appropriate management according to the dysphagia symptoms are important for post-stroke rehabilitation (3, 4).
Velopharyngeal incompetence (VPI), which could be shown as nasal penetration, is one of the symptoms of cough and swallowing dysfunction after stroke. VPI indicates symptoms caused by inappropriate velopharyngeal closure, and is associated with neurological issues, including stroke. VPI is one of 3 categories of velopharyngeal dysfunction; velopharyngeal mislearning, velopharyngeal insufficiency and VPI (12, 13).
Few studies have investigated effective treatment methods of nasal penetration or VPI after stroke. One study showed that treatment with continuous positive airway pressure (CPAP) was effective in patients with VPI (14). CPAP therapy increased the air pressure in the nasal cavities during velopharyngeal closure, leading to strengthening the oropharyngeal muscles, which might be involved in velopharyngeal closure (15, 16).
Mechanical inspiration and expiration (MIE) exercise is a method for improving coughing ability in patients with respiratory muscle weakness. Chatwin et al. reported that MIE exercise improved coughing ability by increasing peak cough flow (PCF) in patients with neuromuscular weakness (17). Like the CPAP therapy, MIE exercise also might strengthen the oropharyngeal muscles, which are involved in velopharyngeal closure. As swallowing and coughing functions are closely related by sharing the same expiration-related muscles (5–9), we hypothesized that MIE exercise may affect both swallowing, especially nasal penetration and coughing functions, in patients after stroke. The aim of this study was to investigate the therapeutic effects of MIE exercise using mechanical cough assist on VPI in patients with subacute stroke.
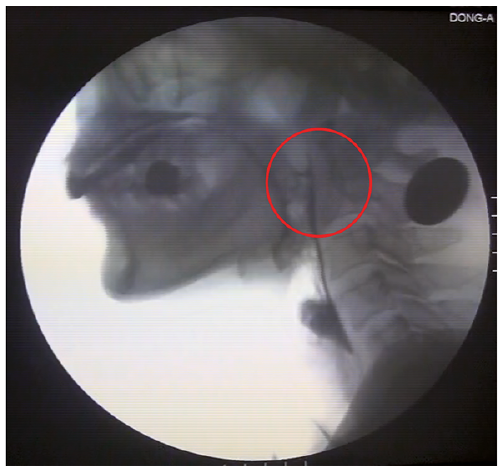
This study was designed as a pilot randomized controlled study and was performed in the rehabilitation centre of a university hospital, specifically a regional cerebrovascular centre from May 2015 to July 2017. No formal sample size calculation was performed. Patients with subacute stroke who had swallowing difficulty were evaluated by a video fluoroscopic swallowing study (VFSS). Among these the patients who showed VPI on VFSS were enrolled in this study. VPI could be shown as nasal penetration on VFSS (Fig. 1) due to inappropriate velopharyngeal closure. Of these patients, those susceptible to barotrauma (atmospheric pressure injury) due to pulmonary diseases, such as emphysema, those with a previous stroke, those with pharyngeal structural abnormalities, those unable to cooperate for MIE exercise due to deteriorated cognitive function or mentality, and those with medical conditions that could affect their swallowing ability were excluded from this study.
Fig. 1. Nasal penetration on video fluoroscopic swallowing study (red circle).
All of the enrolled patients were randomly assigned to 2 groups using a table of random numbers. The study group was administered additional MIE exercise therapy as well as conventional swallowing rehabilitation therapy, while the control group was administered conventional swallowing rehabilitation therapy only.
The study group was administered MIE exercise once daily using the CNS-100 Cough Assist® (SungdoMC, Seoul, Korea) and conventional swallowing rehabilitation therapy twice a day. The treatment procedures for inspiration were as follows: starting positive pressure was 15–20 cm H2O, increased to 40 cm H2O according to the patients’ condition. Inspiration lasted 2 s, or longer if required, and was titrated for patient comfort. The treatment procedures for expiration were as follows: starting with the expiration (negative) pressure was similar to the inspiration pressure, and then the negative pressure was increased to 10–20 cm H2O above the positive pressure. Negative pressure was then held for 3–6 s, simulating the airflows that occur naturally during the cough. The patient was then instructed to coordinate their respiratory rhythms according to those of the cough assist machine (Fig. 2).
Fig. 2. Study group received mechanical inspiration and expiration exercise using mechanical cough assist machine.
Conventional dysphagia rehabilitation consisted of oral motor and sensory stimulation, neuromuscular electrical stimulation of the suprahyoid muscle, and oral and lingual exercises to focus on strength and endurance for the efficacy and safety of the swallowing process (11). Twenty sessions of conventional swallowing rehabilitation therapy were conducted for both the study and the control groups, twice a day, 5 days a week, for 2 weeks, with each session lasing 30 min. Ten sessions of MIE exercise were conducted for the study group once a day, 5 days a week, for 2 weeks, with each session lasting 30 min.
Swallowing function was evaluated using the American Speech-Language-Hearing Association’s National Outcome Measurement System (ASHA-NOMS), Functional Dysphagia Score (FDS) and, Penetration Aspiration Scale (PAS) based on the results of VFSS.
VFSS was performed with the patients in a sitting position to allow a lateral view. A modified version of the protocol from a study performed by Logemann was used (18). First, 3 ml of barium-containing thick liquid was administered to the subject. Then, pureed, semisolid, solid, and thin liquid were administered in this sequence. All of the food samples contained barium and were administered 2 or 3 times. All patients received individualized feeding therapy and dysphagia treatment based on the results of VFSS.
The ASHA-NOMS criteria were published by the American Speech-Language-Hearing Association. These criteria comprise 1–8 stages, depending on the patient’s dietary pattern and the range of possible meals. “Stage 1” indicates the most severe condition of dysphagia and “Stage 8” indicates the mildest condition. It correlates with the severity of dysphagia (19).
The FDS is a scale that was developed to quantify dysphagia severity and it consists of 11 items with weighted values representing 4 kinds of oral (lip closure, bolus formation, residues in oral cavity, oral transit time) and 7 kinds of pharyngeal (triggering of pharyngeal swallow, laryngeal elevation and epiglottic closure, nasal penetration, residue in valleculae, residue in pyriformis sinus, coating of pharyngeal wall after swallow, pharyngeal transit time) functions that can be observed by VFSS (Table I). The FDS can be used to identify various physiological measures, such as the aspiration status and nasal penetration of food. The maximum possible score is 100, achieved by applying different weight values to each item; thus, it is useful for quantifying the degree of swallowing difficulty in dysphagia patients and to quantitatively determine the effectiveness of dysphagia treatment. Among the 11 items, “nasal penetration” is a specific item according to the VPI severity, the absence of residual food to the nasal cavity was scored as 0, < 10% of residual food to the nasal cavity as 4 points, 10–50% of residual food as 8 points, and > 50% of residual food as 12 points for evaluation (20).
Table I. Functional dysphagia scale using videofluoroscopic swallowing study
The PAS evaluates airway invasions and has a maximum score of 8 points. Scores are determined primarily based on the depth to which material passes into the airway and based on whether material passes below the vocal fold and any effort to make eject the material. The penetration category corresponds to level 2–5 on the scale, and levels 6–8 correspond to aspiration (21).
In addition, for indirect measurement of the muscle strength of the pharyngeal muscle involved in the expiration process, the PCF was measured using a Digital Peak Flow Meter® (Micro Medical, NY, USA). Before testing, patients were allowed to use the peak flow meter several times to become accustomed to the test; after this the patients were asked to make their maximal effort at least 3 times. PCF was defined as the highest point of the flow volume of 3 attempts was used for analysis. The PCF is useful to monitor expiratory muscle weakness and bulbar involvement in patients with neuromuscular disease (22).
All tests were performed before and after 2 weeks of rehabilitation therapy under the same conditions by 2 blinded physiatrists. Basic information of the stroke patients, including their age, sex, type of stroke, and the time from diagnosis to VFSS evaluation were also investigated. The study protocol was approved by the Institutional Review Board, and all participants provided written informed consent.
All statistical analyses were performed with the SPSS ver. 21.0 (SPSS Inc., Chicago, IL USA). Statistical significance was evaluated with the Wilcoxon signed-rank test for comparing the results before and after treatment in each group. To investigate the differences in swallowing function between the 2 groups, the Mann–Whitney U test was performed. A p-value < 0.05 was considered statistically significant.
A total of 62 subacute stroke patients with VPI were initially enrolled. Among them, 21 patients with a past history of pulmonary disease or neurological damage, with medical complications that could affect VPI, or who were unable to cooperate were excluded. The remaining 41 patients were randomized and divided into the study group and the control group for treatment. Three patients in the study group and 2 in the control group were lost to follow-up because of early discharge, recurrent stroke, or deterioration of their medical conditions and were thus excluded from the study. A final total of 36 patients (18 in the study group and 18 in the control group) completed the study, including follow-up evaluations (Fig. 3).
Fig. 3. Flow diagram of the study.
Baseline demographic characteristics and initial evaluations are presented in Table II. No significant differences were observed in baseline characteristics between the study group and the control group. Initial evaluation of swallowing and cough function between the 2 groups showed no significant difference (Table II).
Table II. Baseline demographic characteristics
After 2 weeks of rehabilitation, the study group showed significant improvements in the swallowing score of the ASHA-NOMS, FDS and PAS, and cough function for the PCF (Table III). In the control group, significant improvements were also observed in the swallowing score of the ASHA-NOMS, FDS and PAS. By contrast, no statistically significant differences were observed in the sub-scores of FDS for the oral phase, for the degree of nasal penetration, and the PCF in the control group (Table III).
Table III. Changes of measurements before and after exercise in each group, within-group comparison
When the therapeutic effect was compared between the 2 groups, the study group showed more significant improvement in the sub-scores of FDS for the degree of nasal penetration and PCF than the control group. However, no statistically significant differences were observed in the swallowing scores of the ASHA-NOMS and in the FDS in total, for the oral phase, the pharyngeal phase, and the PAS (Table IV).
Table IV. Comparison of the exercise effect between 2 groups
This study aimed to investigate the therapeutic effects of MIE exercise using mechanical cough assist on VPI in patients with subacute stroke. The results indicated that patients in the study group who received additional MIE exercise showed greater improvements in the degree of VPI and PCF than did the patients in the control group. To our knowledge, this is the first study regarding the effect of treatment on VPI in patients with subacute stroke.
VPI, which is represented as nasal penetration, is caused by inappropriate velopharyngeal closure. VPI is one of the various symptoms of cough and swallowing dysfunction after a stroke and is associated with oropharyngeal muscle weakness. Nasal penetration can be considered clinically significant because it is associated with serious upper respiratory tract infection, recurrent or chronic sinus infection and cellulitis (23). Furthermore, post-stroke dysphagia is a risk factor, not only for malnutrition and dehydration, but also for serious complications that can delay functional recovery in stroke patients, prolong hospital stays and cause death (3, 4). Therefore, early detection of dysphagia and appropriate treatment method is important in order to treat each swallowing symptom (3, 4).
In previous studies, most dysphagia and/or coughing dysfunction treatments have focused on prevention of pharyngeal aspiration; few studies have investigated effective treatment methods of nasal penetration or VPI after stroke. Kummer (24). reported that speech therapy was effective for reducing VPD, and another study also showed that therapy using CPAP was useful for VPD patients (14). The results of the current study revealed that the study group that received additional MIE exercise showed greater improvement in both swallowing, especially nasal penetration, and coughing function than did the control group. Using a mechanism similar to CPAP therapy, MIE exercise could increase the air pressure in the nasal cavities during velopharyngeal closure, leading to strengthening of the oropharyngeal muscle, which is involved in velopharyngeal closure in the swallowing process. Strengthening of the oropharyngeal muscle may improve the degree of nasal penetration in swallowing. While swallowing and coughing, the same expiration-related muscles are used. MIE exercise may strengthen the expiration-related muscles. As a result, both swallowing and coughing functions may have improved.
First, in terms of swallowing functions, this study demonstrated that patients in the study group showed significantly better degrees of nasal penetration of FDS than did the patients in the control group. The FDS can be used to quantify dysphagia severity and to identify various physiological measures, including the aspiration status and nasal penetration of food. To determine the effect of MIE exercise on VPI, the FDS score was divided into subsections and was analysed. We found that only the degrees of nasal penetration of FDS showed statistically significant improvement in the study group. There were no significant differences in the total scores of FDS that indicated overall swallowing function or in the swallowing score of the ASHA-NOMS that indicated clinical severity. It was difficult to demonstrate the superiority of the MIE exercise therapy for all kinds of dysphagia symptoms after stroke.
Secondly, in terms of coughing function, the current study found that MIE exercise using cough assist was also effective in increasing the values of PCF, thus improving coughing function after a stroke. Clinically, cough is an important protective mechanism for maintaining a clear airway, removal of sputum or aspirated food from the airways, and previous studies revealed that patients with stroke could experience a decrease in cough function (5–7). Kulnik et al. emphasized that a high PCF value was associated with a lower risk of pneumonia in acute stroke (25). Our previous study suggested that voluntary coughing exercises could be helpful for dysphagia to prevent pulmonary complications in patients with stroke (26).
According to a literature review, cough and swallow pattern generators are tightly coordinated because they share afferent and efferent pathways (6, 8, 10, 27). The relationship between the coughing and swallowing function in stroke patients has been demonstrated in previous studies (5–9). Because the expiration-related muscles used in coughing are also used in the swallowing process, strengthening effect of the expiration-related muscles through MIE exercise improves both coughing and swallowing function in stroke patients.
Previous studies also found that MIE exercise could improve coughing or swallowing function in other diseases. Pitts et al. showed the impact of expiratory muscle strength training on voluntary coughing and swallowing function in Parkinson’s disease (27). Another study demonstrated that MIE exercise improved coughing ability by increasing peak cough flow (PCF) in patients with neuromuscular weakness (17). Sivasothy et al. reported that cough function could be improved by strengthening the muscles involved in expiration through MIE exercise (28).
To our knowledge, this is the first study to demonstrate the effects of MIE exercise on VPI after a stroke. Based on these findings, MIE exercise using cough assist is expected to be applicable to patients with post-stroke dysphagia and VPI. In addition, this therapy is easy to use in the clinical setting and can also be used at the bedside for patients who cannot move in a wheelchair. Therefore, it is likely to be used widely in the future with other various treatment methods.
This study has several limitations. First, the results may not be generalizable to all stroke patients because we enrolled patients who showed VPI in the results of the VFSS. Secondly, the reduction in VPI in this study was observed only after a short-term exercise period of 2 weeks, and the effect was only measured immediately after the treatment period ended. We could not distinguish this effect from spontaneous recovery of dysphagia after stroke. The current study could not reveal the effect of additional MIE exercise on all the phases of the swallowing process. As swallowing and coughing functions have different characteristics according to the stroke lesion types (26), well-designed studies are needed to evaluate the effect of MIE exercise according to the stroke lesion type. Finally, the comparisons in this study were performed on a relatively smaller number of patients, with no long-term follow-up records. Thus, further research on a larger sample size and long-term follow-up are required to confirm the results of this study.
The MIE exercise using cough assist has a therapeutic effect on VPI in subacute stroke patients with dysphagia. Furthermore, this MIE exercise affects both swallowing and coughing functions in patients after stroke. A combination rehabilitation therapy including additional MIE exercise was more effective for alleviating the symptoms of VPI than conventional rehabilitation therapy alone. This therapy is easy to apply in the clinical setting, and can be a useful therapeutic strategy for VPI with dysphagia in patients with stroke.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize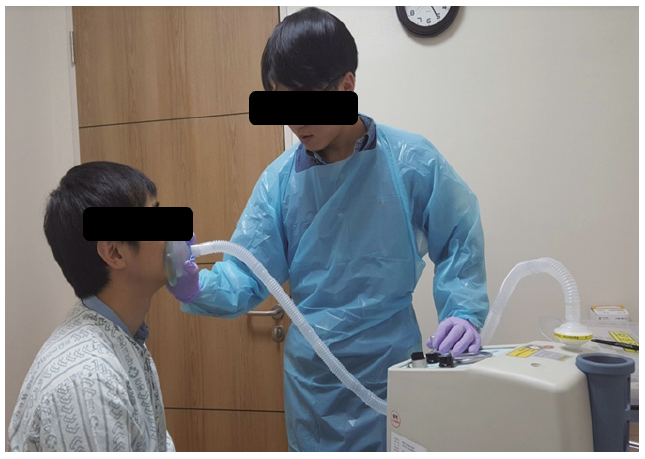 Click to show fullsize
Click to show fullsize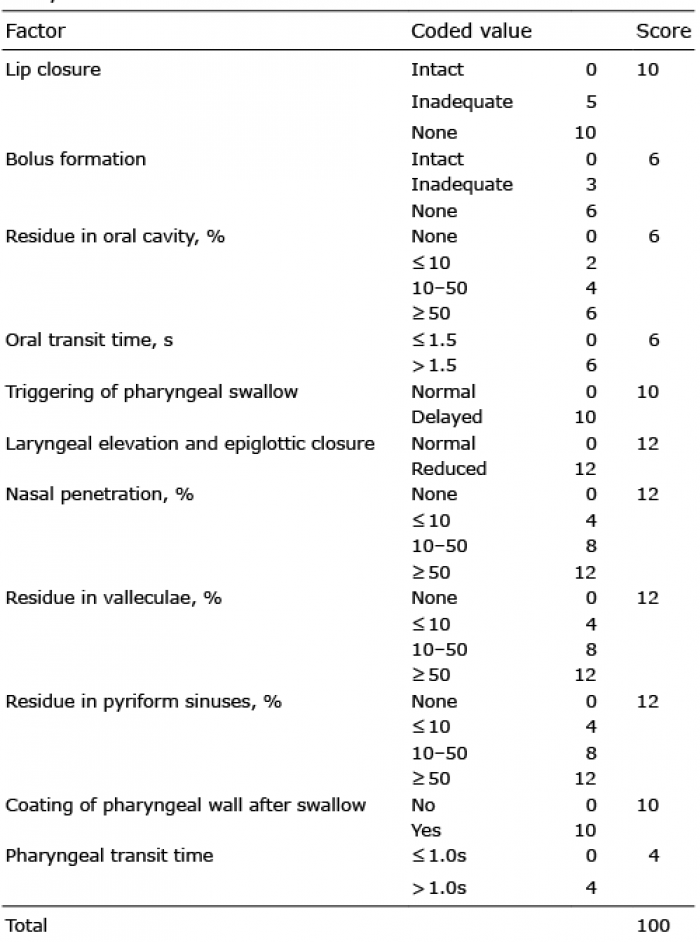 Click to show fullsize
Click to show fullsize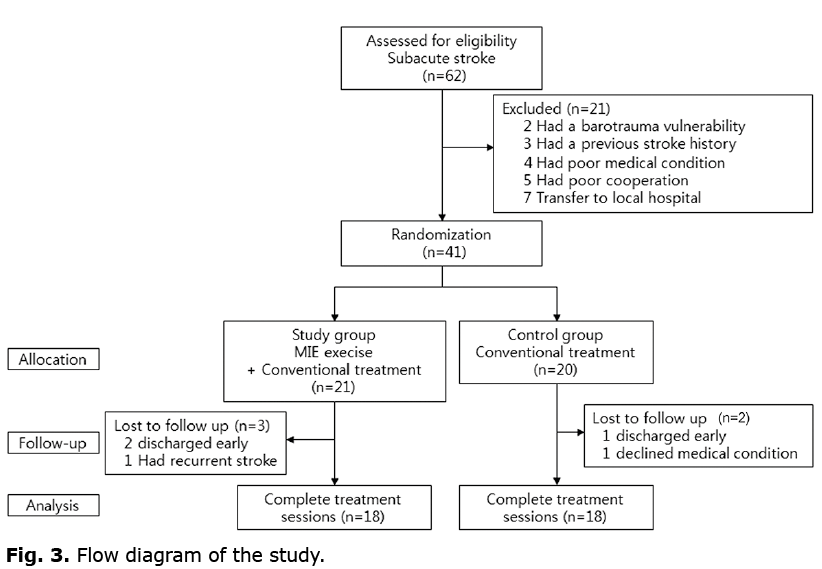 Click to show fullsize
Click to show fullsize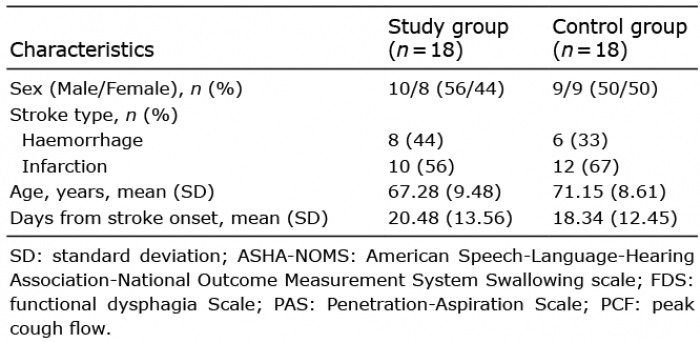 Click to show fullsize
Click to show fullsize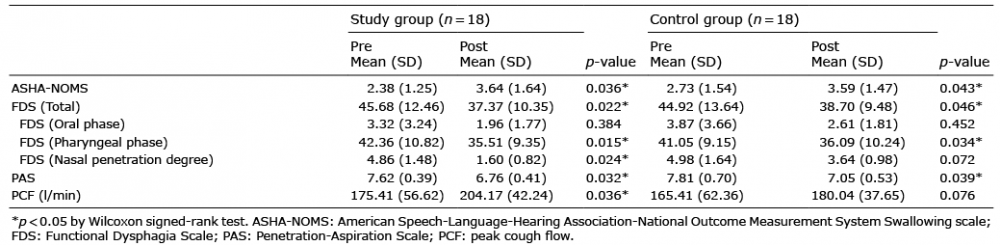 Click to show fullsize
Click to show fullsize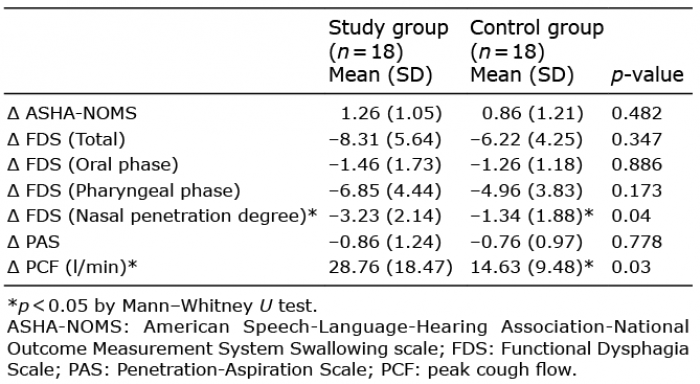 Click to show fullsize
Click to show fullsize