
From the 1Research group MOVANT (MOVement ANTwerp), Department of Rehabilitation Sciences and Physiotherapy, University of Antwerp, Wilrijk, 2Multidisciplinary Motor Centre Antwerp (M2OCEAN), University of Antwerp, and 3Rehabilitation Hospital Revarte, Edegem, Belgium
Background: Pre-clinical evidence suggests a period
early after stroke during which the brain is most receptive to rehabilitation, if it is provided as high-dose motor training.
Objective: To evaluate the feasibility of repetitive gait training within the first 3 months post-stroke and the effects on gait-specific outcomes.
Methods: PubMed, Web of Science, Cochrane Library, Rehab Data and PEDro databases were searched systematically. Randomized controlled trials were included to descriptively analyse the feasibility and quantitatively investigate the effectiveness of repetitive gait training compared with conventional
therapy.
Results: Fifteen randomized controlled trials were included. Repetitive training can safely be provided through body weight support and locomotor assistance from therapists or a robotic device. No difference in drop-out rates was reported despite the demanding nature of the intervention. The meta-analysis yielded significant, but small, effects on walking independence and endurance. Training with end-effector robots appears most effective.
Conclusion: Robots enable a substantial, yet feasible, increase in the quantity of walking practice early post-stroke, which might enhance functional recovery. However, the mechanisms underlying these effects remain poorly understood.
Key words: humans; stroke; stroke rehabilitation; exercise therapy; robotics; walking; paresis.
Accepted Oct 8, 2018; Epub ahead of print Dec 4, 2018
J Rehabil Med 2019: 51: 00–00
Correspondence address: Jonas Schröder, Research group MOVANT (MOVement ANTwerp), Department of Rehabilitation Sciences and Physiotherapy, University of Antwerp, Wilrijk, Belgium. Email: jonas.schroder@uantwerp.be
Animal models suggest that rehabilitation provided as repetitive motor training is most effective early after stroke. To investigate whether such a rehabilitation approach can enhance long-term walking recovery in human patients with stroke, this review gathered clinical studies on the effects of repetitive gait training. We found that robots, in particular, provide a substantial, yet feasible, increase in the amount of walking practice in those stroke patients who are unable to walk. This increase in rehabilitation dose improves walking ability in the long-term. However, these effects are inconsistent, rather small, and in contrast with neutral effects on motor functions of the paretic leg. Therefore, the effects of repetitive training in the context of early stroke rehabilitation remain poorly understood and further research is required.
Stroke is a leading cause of long-term disability worldwide and a dramatic increase in incidence is expected (1). The economic consequences are enormous (2), particularly regarding stroke survivors who remain dependent on continuous support (3). For social participation, regaining mobility is obligatory (4). However, more than 20% of stroke survivors do not reach independent walking (5, 6) and even if achieving independence, the great majority struggle to ambulate in the community (7). These persisting disabilities will aggravate physical inactivity, leading to deconditioning and poor long-term outcome (5, 8). If research fails to provide effective rehabilitation, the increasing incidence will inevitably lead to a growing dependent stroke population.
Considering that no therapeutic approach, to date, has proven superior (9) and effect sizes in clinical research are, in general, low (10), it seems reasonable to reflect on basic research. Interesting pre-clinical evidence on timing of stroke rehabilitation has been published. In rodents, motor training loses effectiveness if provided delayed, i.e. 7 (11) and 30 days (12) post-stroke, respectively, compared with earlier exposure. This activity-induced recovery pattern matches the temporal pattern of increased gene expression important for neuronal growth and plasticity in the post-stroke brain (13, 14). Thus, it appears that a limited period of heightened plasticity is induced early after stroke, in which the brain is most receptive to rehabilitation (14). Since this period is time-dependent, it is best described as a critical time-window for stroke rehabilitation (15).
In human stroke survivors, greatest gait recovery gains occur within the first 3 months post-stroke (5, 16) and rehabilitative interventions outside this period have rather modest effects (15, 17, 18). This time-dependent recovery profile corresponds highly to characteristics of a critical time-window, as mentioned above, which might be reflected in the association between earlier rehabilitation and improved outcome (19, 20). This emphasizes the need to develop a rehabilitative approach designed to take advantage of this time-window.
Such an approach should include high-dose training initiated within the first weeks aiming at the recovery of normal function (15). This is in great contrast with how rehabilitation is provided in current practice (21, 22). Therefore, this review aims to detect therapeutic strategies allowing such intensive therapy in the early phase when patients usually have severe weakness and are unable to walk. It is hypothesized that highly-repetitive gait training has the potential to improve long-term outcome when temporally matching the critical time-window.
However, there are concerns that application of rehabilitation too early might slow recovery (23, 24) or even induce infarct-expansion (25). In addition, clinicians might limit the patient’s effort to engage in exercise, since this can lead to short-term increases in spasticity (26) and an increased risk of falling (27). To clarify these aspects, all trials on early repetitive gait training will be collected to investigate feasibility as well as effectiveness.
Which strategies providing repetitive walking practice to non-ambulatory patients early post-stroke have already been investigated in the scientific literature?
Is early-initiated repetitive gait training feasible in terms of safety and patients’ acceptance?
Is repetitive gait training early after stroke more effective than conventional physiotherapy in terms of gait recovery and do these effects persist?
The current review was developed in adherence to the guidelines of Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) (28).
According to the World Health Organization (WHO), stroke is defined as rapidly developing signs of disturbance of cerebral functions lasting > 24 h (unless interrupted by surgery/death), with no apparent non-vascular cause (29).
The focus here is on the early rehabilitation phase, defined as the first 3 months post-stroke, i.e. the period during which most gait recovery gains are observed (5, 16). Studies initiating gait training within a mean of at most 31 days post-stroke were included, to guarantee that the investigated population was exposed to the intervention within this time-window.
Furthermore, participants included in this review were non-ambulatory (Functional Ambulation Classification (FAC) ≤3, or equivalent) (30) as we aim to report interventions which can be provided to patients who are dependent in walking.
The intervention was considered repetitive gait training if an “active motor sequence was performed repetitively within a single training session, and the practice was aimed towards a clear functional goal” (31). In this case, the motor sequence was defined as whole, complex gait cycles and the functional goal as independent walking. The training might be provided with the assistance of therapists or with (electro-)mechanical devices. Trials were excluded if training is combined with another intervention (e.g. electrical stimulation) and the effects could not be isolated.
A study was identified as a randomized controlled trial (RCT) if the participants were assigned prospectively to 1 of 2 (or more) alternative forms of intervention using random allocation. In included trials all groups spend an equal amount of time on therapy.
In October 2017, the following databases were searched for trials published between January 2000 and October 2017: PubMed, Web of Science, the Cochrane Library, PEDro and Rehab Data. Indexing terms and free-text words of the following key terms and synonyms were used: (Participants) “stroke” and “ (sub-)acute” or “inpatient”; (Intervention) “exercise therapy” or “task-specific training”; (Outcome) “gait” or “walking”; (Study design) “RCT”. A detailed search strategy used in PubMed can be found in supplemental material (see Table SI1). A search revision was scheduled while finalizing the manuscript to avoid missing recently published studies.
Search records were saved in EndNote X8. Duplicates were identified and removed. Afterwards, different screening phases based on abstracts and full-texts were conducted. Disagreement between 2 reviewers (JS, WS) performing study selection independently were discussed with a third reviewer (ST) to reach consensus.
Studies were included when: (i) patients had been diagnosed with stroke, (ii) the mean stroke interval (time between stroke onset and randomization) was at most 31 days, (iii) patients were non-ambulant (FAC ≤ 3), (iv) effects of repetitive gait training were investigated and (v) compared with conventional physiotherapy, (vi) the study used an RCT design, and (vii) the article was written in English, German or Dutch.
The Physiotherapy Evidence Database Scale (PEDro), an 11-item scale, was used to assess methodological quality of included RCTs. All scores were obtained from the PEDro database. The first item, eligibility criteria, does not account for the total score and blinding of patients (item 5) and therapists (item 6) is impossible due to the nature of the intervention. Therefore, the maximum score is considered to be 8 and the following classification is used: a study with a PEDro score of 7–8 is considered good quality, while a score of 5–6 indicates moderate quality. To guarantee high-quality reporting, trials with a high risk of bias, i.e. a PEDro score of ≤ 4, were excluded.
The following data were extracted from selected studies: sample size, stroke interval, baseline impairment, type of experimental intervention and characteristics, between-group differences in the occurrence of adverse events and drop-outs, and effects on gait-specific outcomes. In case of missing data or inadequate documentation, the corresponding author was contacted.
Outcomes of this review were reported in correspondence with the proposed research questions. This firstly includes a description of therapeutic strategies allowing non-ambulant stroke patients to repetitively train walking. Secondly, the 2 feasibility items safety, measured by the incidence of adverse events, and adherence to therapy, defined as the number of drop-outs, were investigated. Thirdly, outcomes on effectiveness were investigated and classified according to the domains of the International Classification of Functioning Disability and Health (ICF) model (32). All included studies had to include the ability to walk independently (primary outcome) as an outcome measure. Secondary gait-related outcomes were included, such as motor impairments of the affected leg and different measures on walking performance.
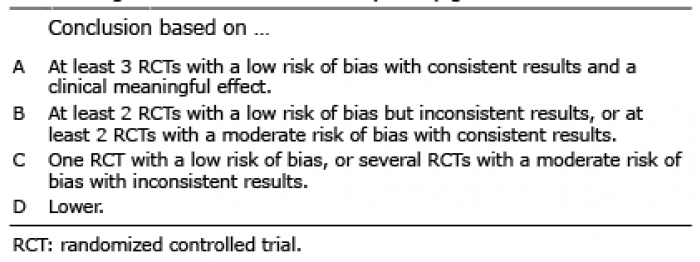
Review Manager software (RevMan 5.3) was used for the quantitative synthesis on the comparative effectiveness. Therefore, the number of participants in both groups together with the means of post-intervention and follow-up scores and its standard deviations were entered in RevMan 5.3 by one reviewer (JS) and cross-checked by another reviewer (WS or ST). If the scores were provided in medians and interquartile ranges, an algorithm developed by Wan et al. (33) was used to estimate means and standard deviations. Summary effect sizes (SES) were calculated with 95% confidence interval (95% CI) based on the effect sizes of individual studies. The mean differences (MD) were calculated since identical measures were used per comparison. When dichotomized outcome on walking independence was reported, an odds ratio was additionally calculated. The I2 statistic was used to determine between-study heterogeneity in results. If heterogeneity was high (I2 > 50%) a random-effects model was used. In each comparison, a sub-analysis on the intervention type was performed. If at least 3 RCTs could be included in a sub-group, the results were reported separately. In addition, if results of 2 or more subgroups were given, the subgroup difference was established using a χ2 test. Finally, the level of evidence drawn from the quantitative analysis were graded using a classification adapted from the Scottish Intercollegiate Guideline Network (SIGN) guidelines (34), where the methodological quality of included RCTs and consistency of results (based on the I2 test for heterogeneity) will be taken into account (see Table I).
Table I. Rating the level of evidence adapted from the Scottish Intercollegiate Guideline Network (SIGN) guidelines
In PubMed, the search strategy (see Table SI1) led to 330 hits on 24 October 2017 and a similar strategy was used in Web of Science. After identifying the 2 main interventions, body weight supported treadmill training (BWSTT) and robot-assisted gait training (RAGT), in other databases (Cochrane Library, Rehab Data, PEDro) the reviewers searched explicitly for those interventions. After de-duplication and a first phase screening on eligibility, 132 unique studies were included for detailed screening on abstract and afterwards on full-text. Finally, 15 studies were included (see Fig. 1). A revision in August 2018 did not reveal additional eligible studies.
Fig. 1. Flow diagram of study identification and selection process. P: participants; I: intervention; S: study design.
In the final screening phase, 4 studies were excluded due to insufficient quality. Of the remaining 15 studies, 9 presented good (PEDro score 8 (35–37); 7 (38–41)) and 6 moderate quality (PEDro score 6 (42–47); 5 (48, 49)) (see Table II). A detailed scoring is shown in Table SII1.
Table II. Characteristics of included studies regarding the methodological quality, recruited population and applied intervention
In the 15 studies, a total of 915 participants were treated and evaluated: RAGT was provided to 286 participants and BWSTT to 152 participants, while 425 participants were allocated to the control groups.
All participants were provided with repetitive gait training or conventional therapy as an add-on to usual care, depending on the group to which they were allocated. Usual care included 25–60 min of physio-therapy daily.
To allow non-ambulant patients in the experimental group to repetitively practice gait, various forms of manual and (electro-) mechanical assistance were provided. In all but 1 (46) included studies, participants’ body weight and trunk was (partly) supported by an overhead harness system, while stationary practicing walking on a moving treadmill or footplates. In a single study, the trunk is not suspended in a harness, but a robot device supports the legs and trunk for stance stability to allow full weight-bearing by the patient (46). Body weight supported training can be divided into BWSTT and RAGT depending on the kind of assistance in locomotion provided. During BWSTT, patients train on a treadmill while therapists manually assist stance stability, swing initiation and forward progression of the paretic leg in a cyclical motion (36, 37, 41, 47). RAGT involves a similar stationary set-up while patients are not manually assisted by the therapist(s), but with an electromechanical device, i.e. a robot. Two different kinds of robots can be classified based on the motion they apply to the patient (see Fig. 2):
Fig. 2. Graphic illustration of identified interventions.
There is an exception to this division. Ochi et al. (46) investigated a treadmill-based system including robotic arms, which guide the thighs and legs to reproduce a physiological gait pattern. As this system resembles the characteristics of before-mentioned exoskeletons (i.e. precise control of kinematics in the hip and knee joints), it will be accounted as such in the analysis.
These training modalities are compared with a control group, which is provided with conventional physiotherapy. This includes pre-gait exercises aiming at paretic leg strengthening and sitting balance. If possible, manual-assisted over-ground balance and gait training was provided. However, the exact content of the control intervention throughout the included studies is poorly described.
Few studies provided detailed information on the therapy dose. Ada et al. (36) documented that participants were able to walk 129 m during the first session of BWSTT compared with only 26 m in the control group. Tong et al. (39) documented that participants performed 500–1,000 steps during a session using an end-effector robot and during conventional therapy 50–100 steps only. Pohl et al. (35) found that participants walked with the same device 851 to 1,076 steps, similar to the results of Morone et al. (43). In addition, Peurala et al. (48) found that, with robot assistance, participants were able to initially walk 20 min without needing resting breaks, while none in the control group were able to. A similar documentation on exoskeletons is lacking, but authors declared that the exoskeleton allowed patients to practice walking at much higher doses compared with the control condition (45, 49). Overall therapy dose, as measured by the total augmented time spent walking in the experimental group, is found to vary between 300 and 960 min. Most studies provided additional 400 min of walking practice in 20 sessions over 4 weeks, meaning that 5 training sessions were provided weekly (see Table II).
In total, 53 patients dropped out of the experimental group, while 55 dropped out of the control group (see Table III). The great majority of drop-outs were unrelated to the intervention (e.g. scheduling interference). In a single study, adverse events were reported without any difference between experimental and control group (43). In addition, few studies reported minor events caused by training, such as discomfort due to the harness (47), hypotension (43), pain (36, 43) or pressure sores (45), which led to a temporal discontinuity of the intervention. However, no study documented a significant difference between groups in the occurrence of such events (see Table III).
Table III. Extracted data from included studies on feasibility and effectiveness on gait-specific outcomes, as documented in the published article
The following outcome measures on the comparative effectiveness of repetitive gait training were detected and classified according to the ICF.
1. Categorization
Activity level: The measurements assessing the ability to walk are classified under the activity domain “walking” (ICF d450).
Body function level:
The results of the meta-analysis for each outcome, as defined above (see Table IV), are described below. Forest plots are derived from RevMan (see Figs S1–S71).
Table IV. Results of the quantitative analysis on the comparative effectiveness of repetitive gait training. This includes gait-specific outcome on both body function and activity level. Sub-analyses based on the intervention type are performed for each comparison and results are analysed if at least 3 RCTs could be included
2. Results
Activity level:
Body function level:
No between-group difference in the occurrence of adverse events and drop-outs was found despite the demanding nature of the intervention. This suggests it is feasible to provide repetitive training early after stroke by the use of an overhead harness system for support of body weight and manual or electromechanical assistance in forward progression of the paretic leg. Statistical significant effects on walking independence (at follow-up) and endurance is found in favour of repetitive training, according to level B evidence. Sub-analyses revealed that these effects are based mainly on studies investigating RAGT provided with an end-effector robot.
Dose-response relation in stroke rehabilitation
In the context of neurological rehabilitation, repetitive training leads to task-specific improvements (10, 31) and associated neuroplastic re-organization (50) if a sufficient dose of practice is provided. In animal models, synaptic changes in the motor cortex are observed after 400, but not after 60 reach-movements (51) and gait training is effective only if at least 1,000 steps are performed during a treadmill session (52). Corresponding findings in clinical research are in favour of a dose-response relation in stroke rehabilitation (17, 53). Despite this solid association between larger quantities of practice and greater gains, inpatient rehabilitation is described as a time of being physically inactive (54, 55) and the practice dose is far less than is provided in previously mentioned stroke models: patients walked for a mean of 250 (21) steps, while non-ambulatory patients walked for as little as 6–16 steps (56) during a therapeutic session aiming at gait recovery.
Technological advances can be of great value in providing more intensive rehabilitation, as robots let non-ambulatory patients train at much higher doses (57). For example, the Gait Trainer allows patients to execute approximately 1,000 steps in a session, while assistance of a single therapist is usually sufficient (35, 39, 43). In line with a dose-response relation, training with such a device appears effective in improving walking independence and endurance. This implies the importance of practice repetitions when designing effective interventions (58) and, in more general terms, the significance of motor learning in stroke rehabilitation (14, 50, 59).
However, the dose-response relationship is not linear, indicating that other factors have an influence (53). Morone et al. (43, 44) compared responsiveness to training between groups who differ in baseline scores on the MI-L (MI-L≈16 vs 52). Outcomes clearly demonstrate that only the more impaired patients benefit (43, 44), which is supported by Pohl et al. (35) as they found impressive effects in a more affected population (MI-L≈32; see Table II). Interestingly, the initial muscle strength of the paretic leg (e.g. assessed with the MI-L (6)) measured within the first days to weeks post-stroke is associated with walking ability at 6 months (5, 6, 60). Therefore, it appears that robot-assisted training was most effective in those patients with a poor prognosis. This might be related to a greater treatment contrast, since the more affected patients do not engage in intensive rehabilitation under conventional conditions (56). As suggested by Morone et al. (57) future research should not investigate if RAGT is effective, but rather who may benefit (43, 57).
It is essential to consider that the task performance in the context of stroke rehabilitation can improve either via restitution of impairments or compensation strategies (15, 61–63). While the included participants potentially improved their ability to walk, we do not know how these changes are achieved, as the FAC does not reflect whether patients “returned towards more normal patterns of motor control” (i.e. restitution), or learned to “accomplish the goal through a new approach by the use of intact muscles, joints and effectors” (62, 64). Since participants improved their ability to walk without normalization of motor control and strength of the paretic leg (see Table IV), it seems that it is rather through compensation that the included patients improved. Indeed, compensation is frequently observed in the recovery of standing balance (65–67) and walking (68) as patients adopt an asymmetrical pattern to shift the kinetic control towards the unaffected side, while normalization of motor control of the paretic leg is almost lacking (69, 70). However, robots provide practice in a symmetrical pattern, which at first sight appears paradoxical. In future trials, analyses of the quality of the gait pattern, including inter-limb coordination in spatiotemporal and kinetic parameters, should be included to provide definitive evidence on mechanisms underlying effectiveness of early training (64, 71). This knowledge will have major implications for practice and designing robots for rehabilitation (i.e. trying to improve impairments or teaching compensation strategies) (15, 72).
Despite evidence in support of repetitive training, small effect sizes are found. These are statistically significant, but the clinical importance is questionable, e.g. an improvement of 24 m on the 6-min walk test does not exceed the minimal clinically important difference (50 m (73)). We have to consider that interventions investigated to date are treadmill- or footplate-based. This means that massed practice of the same action is provided while the device controls balance via a supporting harness and gait via the pre-set belt speed (74, 75). Consequently, the patient is simply exposed to repetitive monotonous movement. However, animal models established that it is not such exposure to movement, but skill learning, that guides neuroplasticity (50). This suggests that stroke rehabilitation requires a whole different concept of RAGT, where the patient is constantly challenged in engaging environments and through variable practice (59). The introduction of mobile exoskeletons might enable the combination of high-dose practice through robotic assistance with the challenging nature of over-ground walking, since the patient has to actively initiate each step and control their balance, meaning that every step taken is treated as a novel problem to solve (59, 74). However, while this intervention may be promising, by exposing the patient to a learning environment, research on the usage of such devices is just beginning.
Only 15 studies, of which 3 are dependent follow-up studies, met the inclusion criteria. Those are mostly phase I or II trials with small sample sizes. Therefore, this review agrees with Stinear et al. (76), who found that less than 10% of clinical trials are initiated in the first 30 days post-stroke (76). A priority shift in research towards the first weeks is required (15, 62).
This research requires a new approach (62, 77, 78). Stratification seems important, since a growing body of evidence suggests that not all patients have the same potential to recover (6, 79). Using prognostic models will help to discriminate between these groups and to identify those patients who are most likely to benefit (80), e.g. by assessing muscle strength of the paretic leg when enrolling participants (6). In addition, our quantitative analysis is based on post-intervention data, which means that the process of recovery is measured as a single outcome score assessed on an arbitrary time-point. Considering that such trials are taking place in the background of spontaneous neurological recovery, a time-dependent process responsible for the majority of improvements on both body function and activity level (63, 81), recruitment and assessments of participants should be performed repetitively and at fixed time-points (77). This allows us to encapsulate the process rather than simply the outcome of recovery. Besides that, the majority of trials describe characteristics of the interventions poorly. A documentation on the dose in terms of repetitions is a far more accurate outcome compared with time scheduled for therapy (23, 53) and would allow us to quantify the treatment contrast between groups to analyse a dose-response relationship in more detail (53). This review highlights the great need to shift the selection of outcome measures from scales simply measuring task accomplishment to those measuring the quality of movement, to gather evidence on how patients improved when engaged in repetitive task practice (14, 15, 63). Taken together, not only a priority shift toward the first weeks is required in rehabilitation research, but also a corresponding shift in methodology with a need for more precision in our trials (77).
In total, 15 eligible studies were identified, which are in general pilot studies with small sample sizes. Consequently, well-designed motor rehabilitation trials starting in the first month post-stroke remain scarce. Repetitive gait training appears feasible and safe. Such training can lead to long-term functional improvements if provided early, but these effects are small. In sub-analyses, RAGT provided with an end-effector appears most effective and it seems that the more impaired patients benefit most. However, analyses on body function level yielded neutral effects and consequently the mechanisms underlying functional gains achieved after augmented gait training remain poorly understood. In the context of walking recovery after stroke, this review suggests that clinical research on early motor rehabilitation and robot-assisted training is still in its infancy.
The author would like to thank Professor Gert Kwakkel for scientific guidance and his support with the interpretation and documentation of results.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize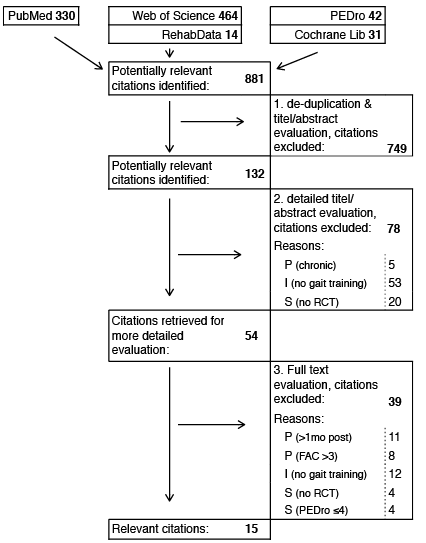 Click to show fullsize
Click to show fullsize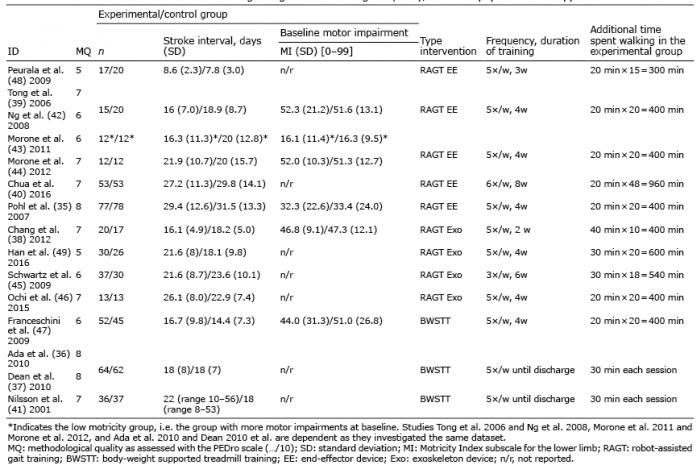 Click to show fullsize
Click to show fullsize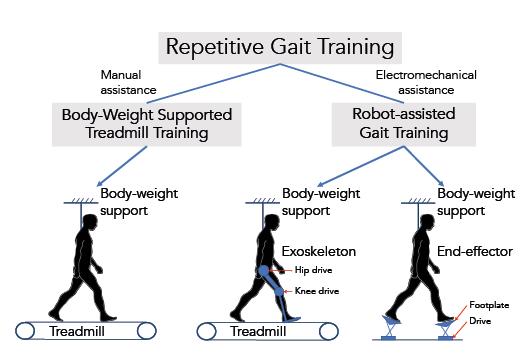 Click to show fullsize
Click to show fullsize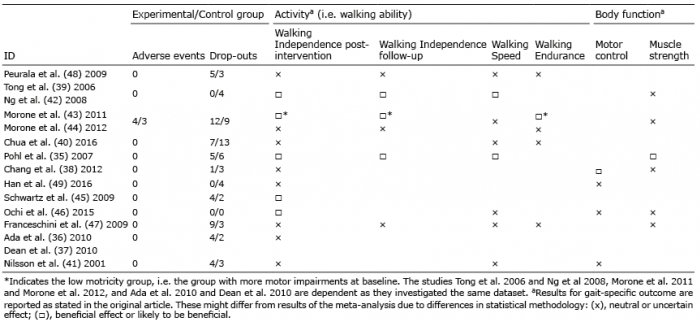 Click to show fullsize
Click to show fullsize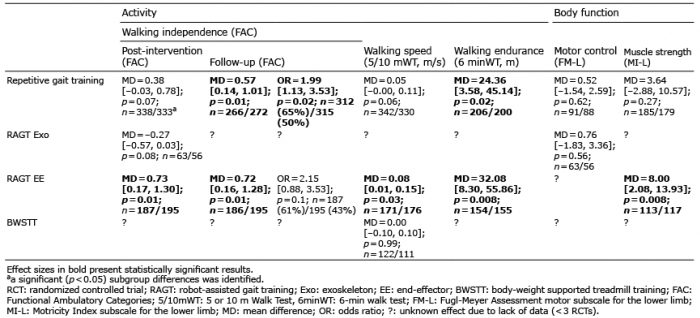 Click to show fullsize
Click to show fullsize