
From the 1Department of Epidemiology and Preventive Medicine (DEPM), School of Public Health and Preventive Medicine, Monash University, Melbourne, and 2Transport Accident Commission, Geelong, VIC, Australia
Objective: To understand clients’ experiences of the recovery journey through the compensation system and to identify areas and strategies for quality improvement.
Methods: A qualitative study of 23 participants with physical or mental disabilities caused by traffic accidents, which occurred, on average, 4 years ago. Purposive sampling of long-term recovery clients who made a compensation claim after their injuries was applied until data saturation was reached. Data were collected using semi-structured interviews and analysed through conventional thematic analysis.
Results: This study demonstrated that recovery is a complex phenomenon that can be impacted by numerous challenges of navigating the compensation system and using its services. Clients perceived the compensation provider as limited in rules around which services they could access. A common perception amongst clients was that the compensation provider did not have the capacity and knowledge to understand health and recovery processes nor did it provide adequate guidelines or instructions that would assist clients with their recovery. Many clients dealt with numerous case managers and felt insufficiently informed on what to expect and do, which led to a lack of trust in rehabilitation management and case managers’ decisions. According to clients, financial impacts were neglected and not addressed effectively. Many clients felt abandoned by the system which led to perceived feelings of desertion and negligence.
Conclusion: Understanding modifiable barriers to recovery in compensation systems presents opportunities to amend current practices and consider a holistic, person-centred care approach. It is apparent that improved recovery management, communication and adequate provision of guidelines are needed to meet clients’ needs and facilitate better outcomes. A person-centred care approach is likely to improve quality of life and help clients navigate the compensation system more effectively with assistance from health and compensation professionals, who should be actively involved in their recovery processes.
Key words: person-centred care; recovery; health outcomes; road trauma; minor injuries.
Accepted Oct 2, 2018; Epub ahead of print Nov 14, 2018
J Rehabil Med 2019; 51: 00–00
Correspondence address: Stella Samoborec, Department of Epidemiology and Preventive Medicine, School of Public Health and Preventive Medicine, Monash University, 553 St Kilda Road, Melbourne, VIC, Australia 3004. E-mail: stella.samoborec@monash.edu
Injuries from transport accidents are heterogeneous and recovery processes complex and challenging for people, regardless of the severity of injury sustained. Multiple factors influence the recovery trajectory, including pain, poor pre-accident health state, psychological comorbidities, socioeconomic disadvantage and, in some instances, financial compensation. In particular, the results on the effect of financial compensation on health outcomes following musculoskeletal injury remain controversial, indicating that further research is needed to understand the possible barriers and complexities involved in compensation processes and service delivery. This qualitative study investigated compensation-related barriers and found that recovery is indeed impacted by numerous challenges in using compensation services after traffic accident. To overcome these issues, it is recommended that a person-centred approach is used as foundation to inform decision-making for interventions aimed at improving recovery outcomes. An improved recovery management, communication and adequate provision of guidelines is needed and highly recommended to meet clients’ needs and facilitate better outcomes.
Transport-related accidents and injuries have been a longstanding public health problem (1). Injuries from transport accidents are heterogeneous and recovery processes complex and challenging for patients, regardless of the type and severity of injury sustained (2, 3). Multiple factors impact the recovery trajectory, including pain, poor pre-accident health state, psychological comorbidities, socioeconomic disadvantage and, in some instances, financial compensation (4–6).
However, there is a lack of consensus as to what impact the compensation system has on health outcomes (7). Multiple studies have shown that patients claiming compensation have significantly poorer quality of life compared with those who do not claim (8–14). How-ever, a recent systematic review revealed mixed results on whether financial compensation is associated with a poorer outcomes, yet no studies in the review reported association between compensation-related factors and improved health outcomes (13).
Therefore, the results on the effect of financial compensation on health outcomes following musculoskeletal injury remain controversial, indicating that further research is needed to understand the possible barriers and complexities involved in compensation processes and service delivery.
In 2014, Grant et al. (15) have identified common stressors in the claims process. Some of the common stressors included high levels of stress associated with understanding what needed to be done with the claim; claim delays; number of medical assessments; and the amount of compensation received. However, from the aforementioned studies, it is difficult to disentangle the role of the compensation system from other stressors affecting poor health outcomes, including the injury itself and the patient’s pre-existing health state (16).
Based on the above, it is somewhat obvious to conclude that compensation after a transport-related injury (TRI) is a complex sociological phenomenon (7). Injury compensation aims to provide payment for medical care needed to treat injuries, replace, to some extent, loss of earnings, and provide support in reaching independence after injury (17), but, as numerous studies have shown, it seems that sometimes compensation can do more harm than good.
However, the compensation system operates within a larger socio-environmental context, and hence may be affected by other public systems, such as the health system. The complexity of service delivery navigated from compensation and health system may consequently result in variations in care and lead to patient perceptions of receiving poor quality care (personal communication).
In Australia, different State and Commonwealth organizations are liable for providing accident compensation. The level of compensation and access to benefits is directed by peoples’ residential address (18). In particular, in the state of Victoria, those injured in land-based transport accidents are eligible to claim compensation for treatment, income replacement, rehabilitation and long-term support services via the Transport Accident Commission (TAC), regardless of fault.
Due to the growing number of minor injuries and consequent long-term non-recovery in Victoria, the objectives of this study were primarily focused on exploring current barriers and obstacles to recovery, focusing on the cohort that sustained predominantly minor injuries.
Therefore, the primary aim of this study was to understand personal experience of recovery in Victorian claimants and to identify barriers and complexities involved in their recovery processes. The secondary aim was to understand the gaps in compensation service delivery and to identify areas and strategies for quality improvement.
This qualitative study was conducted in Victoria, where all transport compensable injury claims must be lodged through TAC (19). TAC is a Victorian government organization whose role is to promote road safety, improve the trauma system and support those who have been injured on Victorian roads. The TAC pays for treatment and benefits for people injured in transport accidents. It is a population-based scheme, funded from annual car registration payments by Victorian motorists. This study was approved by the Ethics Committee at Monash University Human Research (MUHREC 2016 0971-7666).
The study sample included clients who were managed by the TAC Supported Recovery team and were participants in their Client Outcome Survey (COS). The COS commenced in 2009 and annually tracks health, clinical and vocational outcomes of clients. Supported Recovery clients mostly claim for minor and moderate transport-related injuries; have a life of claim exceeding 12 months; and account for approximately 19% of claims and 62% of total claim costs. The current guideline on non-fatal transport-related injuries defines a Minor injury as follows: “minor injury means a sprain, strain, whiplash-associated disorder, contusion, abrasion, laceration or subluxation and any clinically associated sequelae” (20).
A random selection of 41 Supported Recovery clients who, when last contacted in November 2016 for the COS, agreed to be available for future research and had received a TAC-funded service were invited to participate. To recruit participants living in both regional and metropolitan areas, oversampling occurred from people residing in regional Victoria.
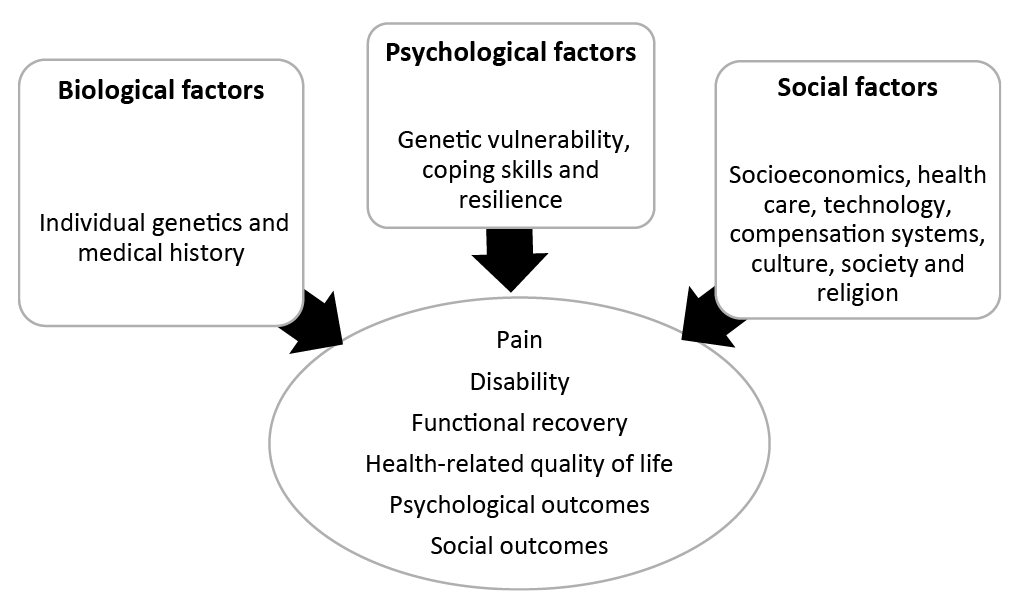
he previously defined conceptual framework was a key part in the development of the interview guide. It was designed based on the Biopsychosocial model (BPS) model ensuring that biological, psychological and social domains of the model were explored in-depth (21). As per the complexity of different domains explored in this narrative inquiry, this paper focuses and describes in depth only one component of the social domain of the model: barriers related to the compensation system and its service delivery.
The conceptualized framework (Fig. 1) guided the development, ensuring that already known risk factors were captured and allowing for the new themes to be identified. Specifically, questions in the social domain covered the clients’ environment including health system, quality of healthcare and relationships with the healthcare professionals; family and friends; and the compensation system and its service delivery. Clients’ needs were also discussed and highlighted in each domain.
Fig. 1. Conceptual framework for identifying factors impacting recovery after a transport-related injury.
A semi-structured interview guide was developed by the principal researcher and reviewed by a team of research experts with experience in qualitative research. The interview guide contained a mix of direct and structured questions (Appendix S11),
which, during interviews, were expanded in order to capture individual experiences. The interview questions facilitated consistent responses from all participants, allowed for flexibility in probing questions and enabled patients to describe their experiences in their own way. This approach allowed clients to speak freely, especially about negative experiences or behaviours.
Recruitment was conducted in 3 phases to avoid recruiting more clients than required to gain data saturation. Data saturation defines the point at which no new themes are identified and it is suggested that it is usually reached at around 12 interviews (22). This phased approach also enabled the researcher to review the interview questions at the conclusion of the first phase, to allow adjustments to be made in subsequent interviews.
The first phase was conducted between March and May 2017. Ten clients were interviewed during phase 1. After phase 1, purposive sampling was employed to ensure adequate representation of male clients and clients from regional areas. The second phase was conducted between May and August 2017. Ten clients were interviewed during phase 2. The final phase was conducted between August and September 2017 during which 3 clients were interviewed. In total, 12 clients were interviewed face-to-face and the other 11 by phone based on the client’s personal preference.
The interviews were audio-taped and typed verbatim by a principal researcher who also conducted the interviews. A thematic approach was taken to identify key issues. Thematic analysis of transcripts was undertaken using NVivo, a qualitative research software (QSR International). Deductive coding was conducted with the conceptual framework used to guide the analysis (Fig. 1). Inductive coding using open and axial coding captured emerging concepts. The constant comparative method was used by comparing concepts between individual transcripts, and later comparing developed codes with emergent themes. Regular meetings between the 4 authors allowed accurate categorization and classification, and the development of typologies and explanatory records to be pursued. In addition, to ensure rigour in data analysis, data were blindly coded by a second qualitative researcher and developed themes were reviewed and examined. After outlining connections between concepts and categories, theoretical concepts and main themes and sub-themes were developed.
Of the 41 patients contacted by phone to participate in the study, 7 opted out, 11 were uncontactable and 23 agreed to participate in the study. Their characterictics are shown in Table I. Those who declined to participate were more likely than those who agreed to participate to have a higher life back on track (LBoT) score (mean score of 7.5 vs 6.9), but other characteristics (age, sex, injury type and education level were not significantly different between the 2 groups.
Table I. Characteristics of 23 interviewed clients who sustained a minor transport-related injury and made a claim at the Transport Accident Commission (TAC)
More participants resided in metropolitan than regional areas (71%); and were female (67%). There was an over-representation of soft tissue injuries compared with other types of minor injuries (67%). The mean time since accident was 4 years with time from injury ranging from 2 to 7 years. Twelve participants were identified as not having their life back on track (LBoT 1–6) and 11 reported their life was back on track during the initial survey (LBoT 7–10).
The majority of “poor recovery” clients (LBoT 1–6) were aged between 41 and 55 years of age, married, with moderate levels of pain and moderate to low quality of life scores. These clients reported that they did not recover or were only partially recovered at the time of the COS survey.
The “good recovery” group (LBoT 7–10) consisted of clients aged between 27 and 70 years of age, living in the metropolitan area, with a claim duration of approximately 25–36 months. In the COS survey, these clients reported moderate to mild level of pain and to have nearly or partially recovered.
Themes captured in social domain and relevant to this paper are shown in the Table II.
Table II. Emerging themes of the access and delivery of compensation services
benefits in using compensation services, but most (17) have raised numerous issues with the compensation system and claiming processes. Some included limits on amount payable or limits on compensated services and others described compensation insurance as a “forced insurance” (considering Victorians must pay for registration and extras), which did not provide adequate social and financial support. The system was also described as limited in scheme rules with certain services that cannot be approved (e.g. plasma therapy). Clients found the guidance in navigating the compensation system to be disappointing and a source of ongoing frustration. Hence, some clients decided not to “bother” with the compensation regulations and paid for services themselves, while others still reported that they had services under review or were using their private health insurance. Surprisingly, 9 of the 11 clients identified as being in “good recovery”, according to the LBoT, reported that they had not recovered and did not believe they were in good health during the subsequent interview conducted by the researcher as part of this project. Consequently, it was not possible to conduct a comparison between the poor health and good health groups due to the small number of people reporting to be in “good recovery”.
1. Benefits of the compensation system
a) Right to use home assistance. Clients (n = 4) felt grateful for assistance provided by the compensation provider following physical incapacitation and stressed how crucial this was in facilitating their recovery. Most clients discussed feeling lost and shocked after the accident, some also experiencing excruciating pain days after the accident. For that reason, timely and early intervention and support with daily duties was crucial for them. Although not everyone experienced this level of support, clients who were supported in their homes or work found this to be vital for their recovery.
The occupational therapist has been here to see me because of assessing for the household things that they are doing. They provided some support with home assistance as I could not do much at the time. This was obviously very important for my recovery. (Female, 48 years old, soft tissue – neck and back)
b) Provision of equipment and/or tools needed to improve daily functioning. Injuries left some clients with ongoing physical disabilities, which consequently led to them needing to make significant adjustments to their home and work environment. This included adjusting steps to aid access and providing chairs/new equipment. This was particularly important for people who were self-employed and still working, so that they could go back to work as early as possible, with adjustments that helped them in dealing with functional limitations they were left with after the accident.
They gave me a new chair that I can lift up and down because if I look down I get dizzy. They also got me a new trolley which is about 6 inches higher than the old trolleys that I had which was really good as well. They sort of did that for me. (Female, 55 years old, soft tissue-contusion)
2. Limitations of the compensation system
c) Scheme limitations. Some issues with the compensation system included limits on the amount payable or limits on compensated services and access to certain services. The compensation insurance system was described as a “forced insurance”, which did not provide adequate social and financial support and was limited by scheme rules which prohibited certain services. “Forced insurance” was a term that clients commonly used in describing how they must pay for car registrations and TAC access fees, but when they needed financial support and help, they have not received what they felt they were entitled to.
Because I wanted to do the alternative treatment and [the compensation provider] said no, so then I had to go back and forth to get things approved. It is a limited service that we are forced to pay but don’t get anything back. (Female, 45 years old, soft tissue- neck and shoulder)
d) Lack of information and guidance. Issues commonly reported by clients involved complexities in the recovery journey with no guidance provided by the compensation provider, in particular, its primary point of contact, the case managers. Clients reported perceived lack of capacity by the case managers to advise on what type of services and when those can be accessed. While some clients (7) reported being confident in navigating the health and compensation process, others (16) stated a preference of having more structured information and guidance at the beginning and throughout the recovery journey.
I keep asking them I want a job [at the compensation insurer] because nobody seems to know anything there and I don’t know anything so I’ll be very good at it and I’ll be quite nice on the phone and will be nice to people and say I don’t know anything and don’t even ring next week cause the people above me don’t know anything either. (Female, 55 years old, soft tissue-contusion)
e) Lack of single point of contact and lack of trust in case managers’ decisions. Case managers were identified by clients as playing an important and enduring role in the coordination of services they receive during their rehabilitation process. It was perceived that case managers were challenged by time and resource restrictions in the management of a large number of clients in need. Clients were aware of the challenges faced by case managers. However, they complained about poor handover of information, constantly repeating their story when trying to get in touch, dealing with administrative people who do not understand medical terminology and the recovery process and a lack of response from the compensation provider when they were contacted. This consequently led to lack of trust in the system in general and even giving up on their claim as some clients expressed they could not have been “bothered” with the provider.
If there was anything that was required I had to have a huge fight. You cannot get this and cannot get that. What can I get!? I was dealing with administrative people who perhaps have no understanding of the real level of capacity after injury and recovery. (Female, 50 years old, soft tissue – neck and back)
f) Lack of understanding the system, its policies and procedures and lack of guidelines. Approximately 60% of clients reported there was no introduction to the compensation processes, no structure about what to expect and what services they can use and who to report back when recovery is not progressing as expected. Clients found the guidance in navigating the compensation system to be disappointing and a source of ongoing frustration.
No … no one explained … no one introduced me to the system or how it works … There was very minimal information provided unless we asked the direct question. The amount of time to get to the same person you can count of one hand … they asked about the medications stuff but even filling that form was a nightmare. Sorry … It was a real nightmare. (Female, 53 years old, soft tissue – neck and back)
g) Financial impacts. Clients also reported financial consequences from inadequate reimbursement of costs for treatment received and from an inability to undertake paid employment to the same extent as they were undertaking pre-accident. Reduced working hours following the accident was in most cases the result of physical injury. Some clients reported that it was very difficult for them to find a new job after the injury due to their disabilities, while other reported being out of pocket due to the misunderstandings on their entitlement under the compensation system.
For the first 3 months I was paying all out of my pockets because they said they need like 12 weeks or something before they can step in. And then after that $600 … yes that’s right I had to pay $600 and after that they started paying for my GP. And then they said it was too much and even though my GP and physio said I need these services they said it’s too much and they won’t pay for it anymore. (Female, 45 years old, soft tissue – neck and shoulder)
This research highlighted that recovery is a complex phenomenon, regardless of the severity of injury attained. Specifically, it demonstrated some advantages of using the compensation benefits, but highlighted numerous challenges in navigating the system and using compensated services.
The findings highlighted numerous complexities involved in compensation service delivery, especially for clients dealing with chronic pain and psychopathology, which often present as vague conditions problematic to definitively diagnose and adequately treat. It has been acknowledged that there are multiple challenges when dealing with people with chronic pain and mental health conditions (23, 24), which are common comorbidities after any road trauma. Previous studies have shown that these challenges commonly lead to trust issues between clients and other professionals and impact the quality of care received (25, 26).
Unfortunately, there is still scarcity of qualitative studies on people with minor injuries and protracted recovery, but few studies that have explored this in-depth have described similar results to this study. A recent study led by Ritchie et al. (27) which focused on patients suffering whiplash associated disorder (WAD) stated that many participants described complexities in navigating and understanding recovery processes incurred by interactions with compensation and funding systems (27). Another qualitative study carried out in Sweden found that medically classified minor and moderate injuries have a long-lasting and detrimental impact on patients’ quality of life (28).
Therefore, it seems that certain complexities are expected during recovery, but the question is how to identify and overcome these issues and provide the best possible support to each client.
The first point to consider is that all the barriers identified in this study are modifiable, which undoubtedly gives room for further action and improvement. A further action plan is likely to be developed based on current gaps, whereas modifiable barriers may serve as the foundation to inform decision-making for interventions aimed at improving recovery outcomes. This will be of great value to recovery management planners, rehabilitation professionals, and affected individuals. Subsequently developed interventions should focus on improving relationship and communication with an ultimate focus on improving recovery outcomes for clients. The most recent research conducted in an injured occupational cohort in 2015, emphasized the importance of the good relationship between the injured clients, case/rehabilitation managers and the healthcare professionals and recommended that good relationship can be achieved only if a person-centred care approach is adopted and followed (29).
This study supports the view of including person-centred care as a foundation for building interventions for improved recovery. A person-centred care approach involves working in partnership with people to understand their unique needs and concerns. Tailoring strategies to these needs leads to more effective and satisfying health outcomes (30). We suggest that a person-centred care approach be used to plan, manage and coordinate clients’ recovery in compensation practices. This means that some of the current processes and activities may need to be focused and tailored based on clients’ experience and needs. A proactive communication with clients and other stakeholders, such as healthcare practitioners is recommended, to ensure consistency and transparency. In addition, a biopsychosocial approach is highly needed to understand psychosocial impact alongside biological factors (31). However, more research is needed in order to understand how exactly the aforementioned person-centred interventions may overcome the identified issues and it is currently underway. Besides that, future efforts should be directed towards exploring how prevalent these issues are among a wider cohort of traffic accident claimants and how to identify them as early as possible so that adequate support can be provided on time. Thus, one problem and massive challenge is the lack of recovery tools that measure the aforementioned issues. It may be possible to consider the development of a new targeted survey in which clients could be asked about barriers to services, system navigation and their unmet needs. Hence, further research on current tools and gaps in measuring recovery is needed and highly recommended.
This qualitative study provides in-depth understanding of the perceptions of clients with a minor injury and protracted recovery navigating the compensation system. Even though this was extensive in-depth qualitative study with well-designed and rigorous methodology, there are limitations. The study represents the views of the clients and does not provide an opportunity for the compensation provider to respond and provide clarifications from their practice. Also, the initial methodology was to compare barriers and facilitators of recovery, which was not achievable due to the small number of clients who have fully recovered. This is probably due to the lack of sensitivity of the LBoT tool, which was unable to capture certain degrees of functional or psychological aspects of recovery. Given this lack of sensitivity, further research is required and these investigations are currently underway. In addition, this study was not intended to be generalizable; yet it is representative of client experiences navigating compensation systems. The findings of this study are hypothesis generating of key themes, which will require further examination in quantitative studies to determine generalizability.
Understanding modifiable barriers to recovery in compensation systems presents opportunities to amend current practices and consider a holistic, person-centred care approach. It is apparent that an improved recovery management, communication and adequate provision of guidelines are needed to meet clients’ needs and facilitate better outcomes. In addition, understanding clients’ experiences and using this information to work in partnership with them may facilitate the development of innovative, person-centred strategies to address unmet need, return clients to health earlier and reduce the length of the compensation claim.
The authors would like to thank the funders and the Steering Committee members. The authors gratefully acknowledge the technical advice and support from the TAC’s representatives. Finally, we express our gratitude to the individuals who participated in the study.
Funding statement: SS, Monash ID 26381494 has received Capital Markets Cooperative Research Centre (CMCRC) living allowance scholarship for conducting this study. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize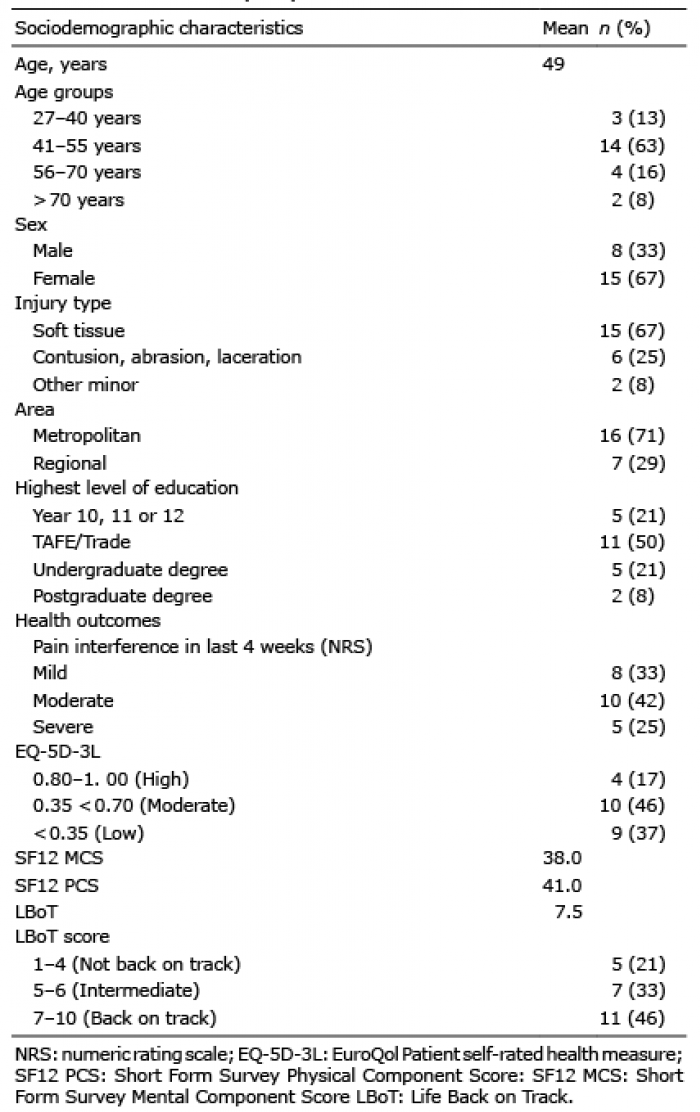 Click to show fullsize
Click to show fullsize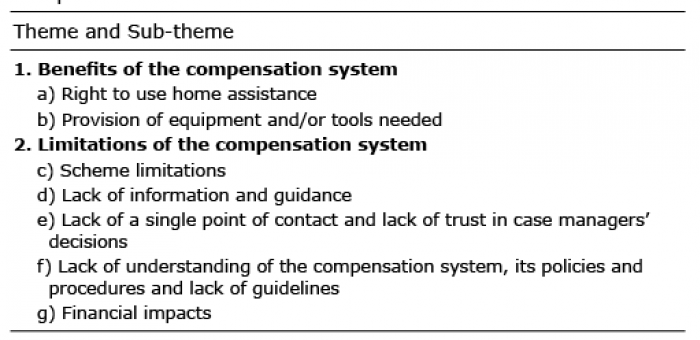 Click to show fullsize
Click to show fullsize