
From the 1Department of Cardiothoracic Surgery, The Heart Centre, Rigshospitalet, University of Copenhagen, 2Department of Nursing, Faculty of Health and Technology, Metropolitan University College, Copenhagen, Denmark, 3Department of Public Health and Primary Care, University of Leuven, Leuven, Belgium, 4Institute of Health and Care Sciences, University of Gothenburg, Gothenburg, Sweden, 5Intensive Care Unit, Rigshospitalet, Copenhagen University Hospital, 6National Institute of Public Health, University of Southern Denmark, Copenhagen, 7Interacting Minds Center, Aarhus University, Aarhus, 8Department of Cardiothoracic and Vascular Surgery, Odense University Hospital, Odense and 9Copenhagen Trial Unit, Centre for Clinical Intervention Research, Rigshospitalet, Copenhagen University Hospital, Copenhagen, Denmark
Objectives: Rehabilitation of patients following coronary artery bypass grafting (CABG) has been widely studied; however, research into early rehabilitation after CABG is sparse. The aim of this trial was to assess the impact of early rehabilitation, compared with usual care in patients following CABG.
Design: Randomized controlled trial.
Patients: A total of 326 patients treated with CABG.
Methods: Patients treated with CABG were randomized 1:1 to 4 weeks of comprehensive early rehabilitation or usual care. The primary outcome was the Six Minute Walk Test (6MWT). Secondary outcomes were mental health and physical activity (Medical Outcome Study Short Form; SF-12); anxiety and depression (Hospital Anxiety and Depression Scale; HADS); physical and emotional scores; sleep (Pittsburgh Sleep Quality Index; PSQI); pain (Örebro Musculoskeletal Screening Questionnaire; ÖMSQ) and muscle endurance (Sit-To-Stand test).
Results: Sixteen patients dropped out. No significant differences between groups in the primary outcome (6MWT) were found after 4 weeks (p = 0.27). For secondary outcomes the odds ratio of HADS-D ≥ 8 decreased in favour of the experimental intervention (p = 0.04). There was non-adherence to parts of the intervention. Per-protocol analysis showed differences between groups for the 6MWT (p = 0.02) and the Sit-To-Stand test (p = 0.046).
Conclusion: In general, the intervention had no effect on the 6MWT, or secondary outcomes, except for depressive symptoms. However, in adherent participants, the intervention had a positive effect for the primary and several secondary outcomes.
Key words: rehabilitation post-CABG; phase 1 rehabilitation; early rehabilitation; coronary artery bypass grafting; physical exercise; psycho-education.
Accepted Oct 2, 2018; Epub ahead of print Nov 28, 2018
J Rehabil Med 2019; 51: 00–00
Correspondence address: Ida Elisabeth Højskov, Department of Cardiothoractic Surgery, Rigshospitalet, University of Copenhagen, The Heart Centre, Blegdamsvej 9, DK-2100 Copenhagen, Denmark. E-mail: ida.elisabeth.hoejskov@regionh.dk
This trial investigated the effects of an early rehabilitation programme in addition to usual care for patients undergoing heart bypass surgery. The programme consisted of exercise training and 4 planned nurse consultations in the period from admission to 4 weeks after surgery. The programme was tested by 163 patients undergoing heart bypass surgery, compared with a similar number of patients who followed usual care alone. The trial did not show any effect of the programme on physical function, but there was a positive effect in reducing depressive symptoms in the rehabilitation group. Although the rehabilitation programme was scheduled, adherence was low. The reason for lack of efficacy could be poor adherence to the programme, as patients who followed the programme significantly improved in terms of physical functioning 4 weeks after surgery. The results provide important information for health professionals for refining early rehabilitation programmes after heart bypass surgery.
Cardiac rehabilitation is differentiated into 3 main phases: in-hospital (phase 1); early outpatient (phase 2), and long-term outpatient (phase 3) cardiac rehabilitation (1). Clinical recommendations for phase 1 rehabilitation for patients undergoing coronary artery bypass graft (CABG) surgery are few, and are based on sparse evidence from trials with small sample sizes and non-representative trial populations (2, 3). Patients with chronic conditions can receive surgical treatment (3); however, the postoperative period can be challenging, with physical and psychological problems and symptoms such as anxiety and depression, immobility issues, respiratory complications, insufficient sleep, and fatigue (4–6).
Exercise training after hospital discharge has demonstrated positive benefits (7), and it seems reasonable to start exercise training immediately after CABG surgery (8). Trials have demonstrated improvements in outcomes, measured by pulmonary complications and physical functional capacity, after CABG (9, 10). Trials targeting psychological and psycho-educational interventions in patients undergoing rehabilitation have shown improvements in symptoms of depression and anxiety (11); however, no published randomized controlled trial using phase 1 rehabilitation for CABG patients has had an adequate sample size (12). A pilot trial was conducted to evaluate acceptability of inclusion, feasibility and intervention compliance, which showed high inclusion, feasibility and safety, but moderate compliance with the physical and the psycho-educational interventions (13). It was hypothesized that comprehensive cardiac rehabilitation would increase physical functioning and improve mental health.
The aim of the trial was to assess the impact of phase 1 rehabilitation and early phase 2 rehabilitation, prospectively named early rehabilitation, compared with usual care, in patients undergoing CABG based on the primary outcome of physical function and on secondary outcomes of physical and mental health, anxiety, depression, sleep, pain and health-related quality of life.
The SheppHeartCABG trial (“Shaping outcomes by Exercise training and Psychoeducation in Phase 1 for Heart patients”) is an investigator-initiated randomized controlled trial (RCT) (14). The trial followed the principles of the Declaration of Helsinki and was approved by the Regional Ethics Committee (H-4-2014-109) and the Danish Data Protection Agency (30-1309). The trial was registered at ClinicalTrials.gov (NCT02290262) and reported according to the Consolidated Standards of Reporting Trials (CONSORT).
The settings were thoracic clinics at 2 university hospitals in Denmark: Odense and Copenhagen. Patients were screened consecutively for inclusion. First-time elective patients undergoing CABG who provided informed consent were included. Patients younger than 18 years of age, patients diagnosed with a musculoskeletal or neurological disease precluding exercise testing and training, and patients who did not speak Danish were excluded. Potential participants received verbal and written information at admission and were recruited over a period of 19 months.
Randomization was 1:1 by central randomization, with the allocation sequence computer-generated using blocks varying between 4, 6, 8, 10, 12, and 14, stratified according to site and sex, and concealed from the investigators, as allocation was done through a web-based system. Full blinding of clinicians and participants is impossible in a rehabilitation trial, but data collection, outcome assessment, data management, statistical analyses, and conclusions were blinded to the allocation group.
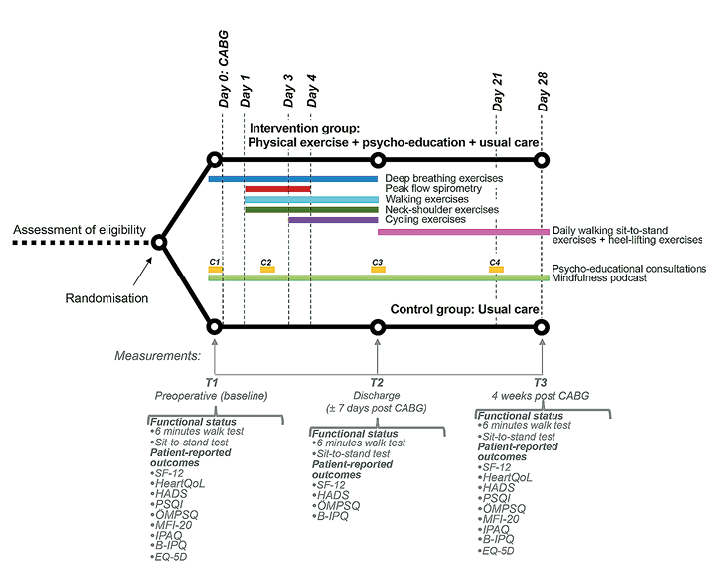
An outline of the trial interventions (14) is shown in Fig. 1 including the intervention components, the timeline for the 2 groups, and the outcome measures.
Fig. 1. Trial design.
The aim of the physical intervention was to improve physical functioning 4 weeks after CABG. The physical rehabilitation programme was initiated the day before surgery. Patient-reported diaries and a heart-rate monitor were used to monitor. The physical interventions were administrated by physiotherapists and included an exercise programme starting at admission and continued for 4 weeks after CABG. The physical intervention was divided into respiratory physiotherapy and aerobic training. After hospital discharge, until 4 weeks after CABG, exercise included continuous daily walking and muscle and endurance exercises (Fig. 1).
The aim of the psycho-educative intervention was to improve disease coping by applying a patient-centred approach. The conceptual foundation for dialogue with patients was based on the Human Becoming Practice Methodologies by Parse (15). The consultations were performed by 6 trained nurses and most participants met the same nurse at all consultations. A consultation guide was followed to ensure intervention fidelity and the nurses were supervised regularly (13). The psycho-educative intervention consisted of 4 face-to-face consultations. Mindfulness was an integral element in the psycho-educational consultation and was provided as a toolbox of recorded meditation instructions for personal use, e.g. as an alternative to medication for sleep disorders and physically and emotionally stressful situations (14).
All patients in the control group followed usual care procedures (16), which included medical follow-up and standard treatment according to disease-specific guidelines (2). Admission time after CABG is between 5 and 8 days. Usual care includes preoperative and postoperative information provided by physicians, nurses and physiotherapist. Instructions regarding precautions after sternotomy are pre-operatively supplied by physiotherapists covering the immediate postoperative period during hospitalization. Close to discharge the physiotherapists introduced and informed the patients about how to be physically active, but still pretecting the sternum.The main topics of preoperative nursing are: an admission interview, followed by postoperative screening (falls, nutrition); introduction to postoperative pain and nausea medications; pain assessment and postoperative activities. Initial postoperative care focuses on observation of vital signs. The subsequent time in hospital focuses on recovery and preparation for discharge.
Outcome assessment was carried out at 3 time-points: baseline; discharge; and 4 weeks post-CABG.
Primary outcome: physical function. Physical functioning at 4 weeks following CABG was measured with the Six Minute Walk Test (6MWT) (17). Participants walked up and down a 30-m hallway for 6 min according to guidelines (18).
Secondary outcomes. The secondary outcomes were physical activity and mental health measured by the Medical Outcome Study Short Form (SF-12) (19), anxiety and depression by the Hospital Anxiety and Depression Scale (HADS) questionnaire (20), physical, emotional and global scores by the HeartQoL questionnaire (21), sleep expressed by the Pittsburgh Sleep Quality Index (PSQI) (22), pain evaluated by the Örebro Musculoskeletal Screening Questionnaire (ÖMSQ) (23), and muscle endurance measured by a Sit-To-Stand test (24).
The 6MWT was administered by a nurse or a physiotherapist at baseline and by physiotherapists at discharge and 4 weeks after surgery, with defined criteria for termination (18). Serious adverse events were registered and discussed with the responsible physician and primary investigator.
Sample size was calculated to comprise 326 participants based on the expectation of achieving an improvement in 6MWT by 30 m, a standard deviation of 90 m, with alpha of 5% and a power of 85%. The anticipated improvement in the intervention group is assumed to be feasible because the SheppHeartCABG pilot (13) showed a mean of 548 m in the intervention group and 451 m in the control group measured by 6MWT.
Intention-to-treat analyses were used. There were 2 types of comparisons between the intervention groups: (i) comparison of values at week 4 after surgery, this analysis used a general univariate linear model (excepting HeartQol and HADS (see below) adjusted for baseline values and stratifying variables (sex and site)) and (ii) comparison of values at discharge and at 4 weeks. This analysis used a mixed linear model including an unstructured covariance matrix. In this model, the interaction between intervention and time was of principal interest. This analysis was adjusted for baseline values and stratifying variables (sex and site). If the assumptions of the models were not fulfilled with reasonable approximation, removal of outliers and transformation of outcome were performed. HeartQol quantities were converted to binary quantities based on the median score among available cases. HADS was reported as mean and standard deviation and converted to binary quantities (score ≥ 8) as probable anxiety or depression. For both outcomes, logistic regression models were used to compare the experimental and control group (usual care) at 4 weeks, adjusted for value at baseline. Since almost all secondary outcomes were overpowered (14), Cohen’s d was calculated for primary and secondary outcomes as a measure of effect size.
For the primary and secondary outcomes, multiple imputation of missing values using the Markov chain Monte Carlo approach was carried out, since the number of participants with missing values was above 5%. The variables included group, stratifying variables (site and sex), time (baseline, discharge and 4 weeks after discharge) and all outcomes. The primary outcome (6MWT) was tested using a significance level of 0.05. Analyses of the secondary outcome measures as pre-planned in the protocol were analysed with no adjustment of p-values due to multiplicity. Instead, the interpretation of each secondary outcome measure was assessed in the light of multiple testing.
The pre-specified per-protocol level of intervention adherence was defined (14) as completing at least 75% of the exercise sessions and consultations and using one of the mindfulness tools on 75% of the days. However, only one participant reached that level. Therefore, it was decided before the start of analysis to change the per-protocol level to participation in at least 50% of the exercise sessions and psycho-educational consultations. Adherence to the exercise intervention was assessed using the patient-reported exercise diary, and the recordings made for the psycho-educational intervention at each visit.
Statistical analyses were conducted in SPSS V.22 (SPSS Inc. IBM), R version 3.1.2 (R Foundation for Statistical Computing, Vienna Austria) and SAS V.9.3 (SAS Institute, Cary, NC, USA).
Between November 2014 and June 2016, 717 patients were identified and screened. A total of 277 patients were excluded and 114 of the remaining 440 participants (26%) declined to participate. A total of 326 patients were randomized (Fig. 2).
Fig. 2. Flow of patients in the SheppHeartCABG trial. Consolidated Standard of Reporting Trials (CONSORT) flow diagram.
The sex ratio was equal among those patients who declined to participate and the included patients. In the randomized group 11 patients dropped out from the experimental group and 5 from the usual care group (control group). Of the 310 remaining patients, 87% were men, with a mean age of 65 years (range 33–83 years). NYHA class ranged from I to IV (Table I).
Table I. Baseline characteristics: experimental group and control group
Primary outcome. There was no statistically significant difference between the experimental and control groups at 4 weeks after CABG on 6MWT (16.2 m (95% confidence interval (CI): –13.0 to 45.4 m), p = 0.27) and no significant interaction between intervention and time was observed (p = 0.55). Cohen’s d was 0.14 (Table II).
Secondary outcomes. Testing the secondary outcomes no p-value less than 0.05 was observed, except a difference in favour of the experimental intervention detected on HADS-D ≥ 8 (odds ratio = 0.46 (95% CI: 0.22 to 0.97), p = 0.04) (Tables II and III). The secondary outcomes showed a tendency toward better scores in the experimental group on all outcomes except SF-12 PCS (Physical Component Scale).
Table II. Mean difference in outcome and odds ratio between experimental group and control group
Table III. HADS-anxiety and HADS-depression in experimental and control groups
In the intervention group, 110/152 (72%) patients participated in the exercise training programme with the number of sessions completed depending on length of hospitalization. Sixteen (15%) participants conducted ≥ 75% of the training programme, 35 patients (32%) 50–74%, and 59 (54%) patients carried out < 50% of the sessions. The patients participated in 65% (median 68) of the training programme during admission and 54% (median 63) after discharge.
All participants in the experimental group participated in the psycho-educational intervention, of whom 115/152 (76%) attended all 4 consultations. Regarding mindfulness 91/152 (60%) participated in the introduction given as part of the psycho-educational consultation. Of these, 2 patients (2%) used the mindfulness toolbox exercises on ≥ 75% of the following days in hospital, 10 (11%) on 50–74% of the days and 79 (86%) used them rarely or not at all.
Per-protocol analysis was performed on patients who completed more than 50% of the exercise training programme in and out of hospital and the psycho-educational consultations (n = 51 (34%)). There was a difference between the experimental and control group on the 6MWT as primary outcome (41.1 m (95% CI 8.0–74.3 m), p = 0.02) and on 1 of the secondary outcomes, the Sit-To-Stand test (1.87 repetitions (95% CI 0.04–3.70 repetitions), p = 0.046) 4 weeks after surgery. These differences corresponded with a Cohen’s d of 0.40 and 0.36, respectively (Table IV). The remaining secondary outcomes, showed no significant differences.
Table IV Results of per-protocol. The estimates are the mean difference in outcome and odds ratio between experimental and control groups
One serious adverse event was reported at baseline in the experimental group after administering the 6MWT. The participant had 2 episodes of ventricular tachycardia after ending the 6MWT. The event was evaluated to be independent of the 6MWT. There were no serious adverse events in the control group.
To the best of our knowledge, this is the largest randomized controlled trial to examine the effect of a comprehensive early rehabilitation programme including a physical and a psychological component in patients who have undergone CABG surgery. The intervention appeared safe, with only one serious event, which was not related to the trial. The difference between the experimental group and control group for 6MWT was statistically non-significant and only a small clinical effect was indicated by Cohens’ d.
The secondary outcomes showed no difference between groups, except a potential difference in favour of intervention with regard to HADS-D. The intervention might have had a beneficial effect on depressive symptoms. However, it is a secondary outcome and the result should be interpreted with caution. Data from HADS was dichotomized, which produces a risk of reducing the complexity. When looking at the mean scores, there is a 0.6-point difference between the groups in favour of the intervention group. Symptoms of depression compared with anxiety are more prevalent in patients undergoing CABG surgery (25), but they reported a greater reduction in symptoms after surgery compared with others undergoing open heart surgery (26). No trial has investigated the effect of psycho-education combined with physical training after CABG. A systematic review found psycho-education intervention to have a moderate effect in decreasing anxiety and depression after CABG surgery (27), which is in line with our findings.
The intervention showed no effect on self-reported physical and mental health, anxiety, pain, sleep or health-related quality of life, but there was a positive tendency in all outcomes. It is possible that the choice of primary and secondary outcomes was inadequate. The comprehensive test battery included separate valid instruments used in other rehabilitation trials. However, the order of the instruments could influence the responders’ approach to the answers. Even though the instruments were different, questions sometimes looked similar, which could have been annoying for some responders. It is not obvious why changes were not found, but a plausible explanation is poor adherence to parts of the intervention. Patient adherence was high for the psycho-educational consultations. Subsequent use of the mindfulness toolbox varied greatly. In most cases the recorded mindfulness instructions were used in a few instances for a specific problem, reflecting mainly male participants’ scepticism towards mindfulness (28). The sporadic use of mindfulness tools was expected given the brief rehabilitation programme. In other contexts the effect of mindfulness components requires regular practice (e.g. weekly meetings extending for 4–8 weeks after hospitalization) (29).
The per-protocol analysis showed differences between the 2 groups in 6MWT and Sit-To-Stand test, albeit with a small clinical effect expressed by Cohen’s d. This suggests that non-adherence to the rehabilitation has affected our results. The findings from the experimental adherent group are identical to those of the few studies of physical training in early rehabilitation (9, 30) and the pilot test prior to this trial (13). Hence, we hypothesize that low adherence has biased the results towards null. Adherence is a known challenge in rehabilitation (31) and was highlighted in the pilot trial (13). Physiotherapists placed more emphasis on “why and how to do exercise” in this trial and the self-reported diary was simplified to enhance adherence. Further research in adherence and in the profile of non-adherent individuals is needed. The exploratory and hypothesis-generating analysis could indicate from a comparative effectiveness research point of view that the intervention had an effect in those patients who had a certain level of participation. The per-protocol analysis showed that, for the majority of the secondary outcomes, the experimental group had a more advantageous development than the control group, resulting in a Cohen’s d indicating a small clinical effect.
The complex intervention used here reflected the problems associated with CABG surgery. It was developed to be “comprehensive” and included both physical and psycho-educational components. However, the programme may have been too ambitious, because when evaluating the intervention that addresses separate components it becomes difficult to identify the specific effect of each element. Further research is needed to optimize the components of rehabilitation and to identify barriers to adherence in early rehabilitation after CABG.
Patients were included consecutively from an unselected CABG population with a number of exclusion and inclusion criteria securing external validity. The trial applied central stratified randomization to secure against selection bias, and a blinded assessment and statistical analysis to reduce detection and interpretation bias. Of the 440 eligible patients 326 were randomized, which is a high inclusion rate in rehabilitation. Participating in a clinical trial might exert an effect on the physical and mental health of patients through contact with health professionals. A concern is that the control group might have received unintended intervention during admission or at testing by the trial personal. The trial results might have been affected by the participants being aware that they were being studied or that they received additional attention. Self-reported outcomes as used in the diaries and the questionnaires are by nature subjective and therefore likely to have a risk of recall bias. Nonetheless, the patients completed the questionnaires independently of researchers.
In conclusion, the SheppHeartCABG had no effect on the primary outcome, the 6MWT, or on secondary outcomes, except that the intervention might have had a beneficial effect on depressive symptoms. Parts of the intervention were associated with a high level of non-adherence, jeopardizing the “dose” received. From the point of view of comparative effectiveness research the intervention had a positive effect for adherent participants, showing differences between the 2 groups in the physical outcomes 6MWT and Sit-To-Stand test. Furthermore, the majority of secondary outcomes in the experimental group showed a more advantageous development than in the control group. However, these differences were non-significant and had a small clinical effect.
The authors would like to thank the 326 participating patients. We further thank the test and rehabilitation team from the Departments of Occupational Therapy and Physiotherapy at Rigshospitalet and Odense University Hospital. We thank Jette Hallberg, Graziella Zangger, Signe Gils Andersen, Karina Gregersen Jensen, Tina Torobi, Katrine Thingholm Erhardsen, Asker Kristensen and Jesper Topperup for training the patients and Peter Schmidt-Andersen, Freja Sønder, Kasper Ipsen, Jess Hasselby Nielsen, Katri Vainio-Pedersen, Camilla Nielsen and Rikke Sørensen for testing. Thanks also to Bente Birgitte Brodersen, Camilla Larsen, Tine Logan and Line Dan Jensen for conducting the psycho-educational intervention in collaboration with BB and IEH. Last but not least, we thank the steering committee.
Funding: The SheppHeartCABG has received funding from: The Heart Centre Research Foundation, Rigshospitalet, The Foundation of Cardiothoracic Surgery, Rigshospitalet, Metropolitan University College, The Lundbeck Foundation (FP 55-2013), Aase & Ejnar Danielsen Foundation (10-001245), Association Oestifterne (14-105 and 16-070), Research Foundation Rigshospitalet, and Odense Universitetshospital (13-A752).


 Click to show fullsize
Click to show fullsize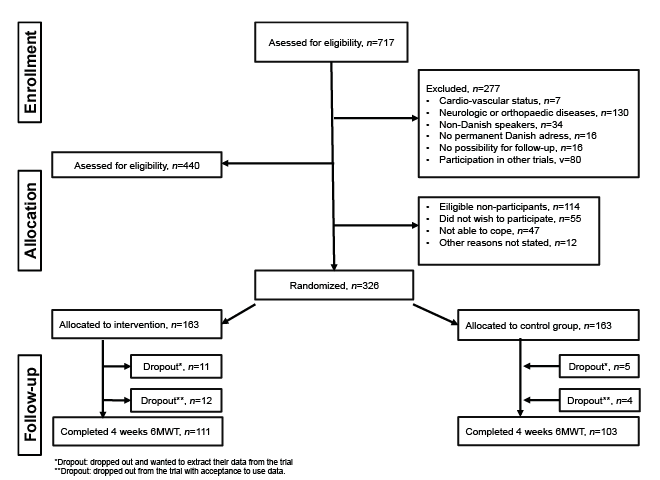 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize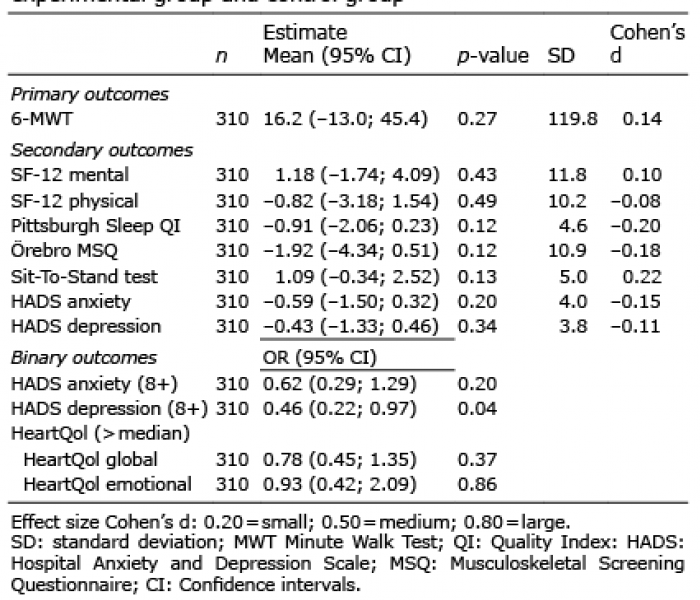 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize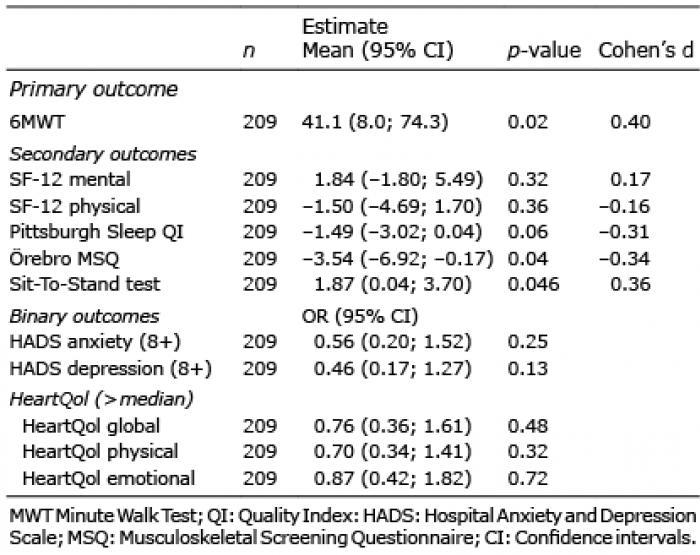 Click to show fullsize
Click to show fullsize