
From the 1Department of Rehabilitation and the 2Department of Neurology, The Affiliated Hospital of Xuzhou Medical University, Xuzhou, Jiangsu, China
#These authors contributed equally to this paper.
Objective: To evaluate whether extracorporeal shock wave therapy significantly improves spasticity in post-stroke patients.
Design: Systematic review and meta-analysis.
Data sources: PubMed, EMBASE, EBSCO, Web of Science, Cochrane CENTRAL electronic databases.
Study selection: Randomized controlled trials assessing the effect of extracorporeal shock wave therapy on post-stroke patients with spasticity were selected for inclusion.
Data extraction: Two authors independently screened the literature, extracted data, and assessed the quality of included studies. Primary outcome was modified Ashworth scale (MAS). Secondary outcomes were Modified Tardieu Scale (MTS), H/M ratio and range of motion.
Data synthesis: Eight randomized controlled trial studies (n = 385 patients) were included in the meta-analysis. There was a high level of evidence that extracorporeal shock wave therapy significantly ameliorates spasticity in post-stroke patients according to the 4 parameters: MAS (standard mean difference (SMD) −1.22; 95% confidence interval (95% CI): −1.77 to −0.66); MTS (SMD 0.70; 95% CI 0.42–0.99,); H/M ratio (weighted mean difference (WMD) –0.76; 95% CI –1.19 to –0.33); range of motion (SMD 0.69; 95% CI 0.06–1.32). However, there was no statically significant difference on the MAS at 4 weeks (SMD –1.73; 95% CI –3.99 to 0.54).
Conclusion: Extracorporeal shock wave therapy has a significant effect on spasticity in post-stroke patients.
Key words: extracorporeal shock wave therapy; stroke; spasticity; neurorehabilitation; meta-analysis.
Accepted Jul 30, 2018; Epub ahead of print Sep 28, 2018
J Rehabil Med 2018; 50: 00–00
Correspondence address: Jie Xiang, Department of Rehabilitation, The Affiliated Hospital of Xuzhou Medical University, 99 West Huaihai Road, Xuzhou, Jiangsu 221002, China. E-mail: 18052268386@163.com
The effect of extracorporeal shock wave therapy on spasticity in post-stroke patients has been evaluated in several clinical trials. In addition, a recent meta-analysis suggests that such therapy is effective; however, the measurement of spasticity was based mainly on the modified Ashworth scale, which is insufficient, and a lack of randomized controlled trials studies in the study design may have biased the results. Therefore, considering the potential limitations of the previous meta-analysis, the aim of the current study was to perform a systematic review and meta-analysis of randomized controlled trials to evaluate the effectiveness of extracorporeal shock wave therapy on spasticity in post-stroke patients. Furthermore, subgroup analysis was performed to identify potential moderators or mediators.
S
pasticity is a common complication of various neurological diseases, such as stroke, and is often defined as a velocity-dependent increase in muscle tone, with exaggerated tendon jerks, due to hyperexcitability of the stretch reflex (1). Stroke has a high morbidity and sequelae rate. Approximately 80% of stroke patients have motor dysfunction, and spasticity status is considered to be the main determinant of this (2). Approximately 20-–40% of stroke survivors will develop spasticity (3). Futhermore, only 15.6% of post-stroke patients have a clinically relevant degree of spasticity (MAS ≥ 3) (4), and the prevalence of disabling spasticity 1 year after first-ever stroke is 4% (5). Spasticity after stroke not only limits the subject’s limb movements, but also impacts on their ability in activities of daily living (ADL), and seriously reduces quality of life (QoL). Therefore, improving spasticity post-stroke would reduce the rate of disability.
Various therapeutic interventions can be used to reduce spasticity, including botulinum toxin (BTX) injections, pharmacological treatment, physical therapy (electrical stimulation, thermotherapy), occupational therapy, and chemical neurolysis (6–9). Extracorporeal shock waves have been reported to be a potential therapeutic intervention to improve spasticity (10, 11).
Extracorporeal shock waves are a group of mechanical pulse waves characterized by high peak pressure (100 MPa), fast pressurization speed (< 10 ns) and short cycle time (10 μs) (6). The treatments can be divided into focused extracorporeal shock waves (12) and radial extracorporeal shock waves (rESW) (13). rESW is a relatively new technique that was first applied in 1999. Extracorporeal shock wave therapy (ESWT) has been shown to be a safe, effective, non-invasive treatment for spasticity in patients with cerebral palsy, epicondylitis and multiple sclerosis (13–16). Several studies have shown that ESWT is effective for treating spasticity in post-stroke patients (17, 18). Dymarek et al. (19, 20) indicated that ESWT could effectively improve limb spasticity in post-stroke patients. In addition, a recent meta-analysis demonstrated the effectiveness of ESWT for spasticity in post-stroke patients (21). However, this was not a meta-analysis of randomized controlled trials (RCTs), and the quality of the included studies was not high. Considering the potential limitations of this earlier meta-analysis, the aim of the current study was to perform a systematic review and meta-analysis of RCTs to assess whether ESWT significantly improves spasticity in post-stroke patients. Furthermore, subgroup analysis was carried out to identify potential moderators or mediators.
A systematic review and meta-analysis was performed according to the guidelines of the Cochrane Handbook for Systematic Reviews (22) and the Preferred Reporting Items for Systematic reviews and Meta-Analysis (PRISMA) statement (23). PubMed, EMBASE, EBSCO, Web of Science, Cochrane CENTRAL electronic databases were searched systematically from the establishment of the database to December 2017, with the key search terms: “extracorporeal shock wave therapy” and “stroke”. The reference lists of the resulting publications and reviews identified in the initial searches were scanned for further references. The literature search was limited to publications in English.
The inclusion criteria for selection of studies were: (i) double or single-blind RCTs; (ii) participants with a diagnosis of ischaemic stroke or haemorrhagic stroke who had spasticity of the lower or upper limb with a MAS score >1; (iii) experimental groups treated with ESWT alone or ESWT combined with other interventions; (iv) control groups treated with sham ESWT alone or sham ESWT combined with other interventions; (v) English language publications.
The exclusion criteria were: (i) studies that were not RCTs; (ii) studies in which the participants were children or adolescents (aged less than 18 years); (iii) reviews, case reports/series; (iv) non-English articles; (v) duplicated data; (vi) studies in which relevant outcome indexes were not reported.
Two reviewers (WW, WFJ) independently extracted the following data: (i) sample characteristics (sample size, mean age, sex); (ii) clinical features (diagnosis, spasticity at baseline and study end-point); (iii) ESWT therapy protocol (frequency, intensity, site, number of treatment sessions). Study outcome was based on MAS, MTS, H/M ratio and range of motion before and after ESWT.
The quality of RCTs was assessed independently using the methods recommended by the Cochrane review (24). Two investigators (WW, WFJ) independently assessed the quality of the study, and any disagreements were resolved by discussion and consensus with a third author (QCQ). The quality assessment includes 6 domains: random sequence generation, allocation concealment, blinding of investigators and/or participants, blinding of outcome assessment, degree of incompleteness of outcome data, and selective reporting of study outcomes. Each domain has low, moderate, or high risk.
All statistical analyses were conducted using RevMan 5.3 (The Cochrane Collaboration, Software Update, Oxford, UK) and Stata 12.0 (Stata Corp, College Station, TX, USA). All continuous outcomes are expressed as mean differences (standardized and weighted to be determined by available data). Sensitivity analysis was performed to examine the influence of a single study on the overall estimate by omitting 1 study in turn. A p -value <0.05 was considered statistically significant. If p < 0.05 and I2 value > 50%, the random-effects model was used; otherwise, the fixed effects model was used.
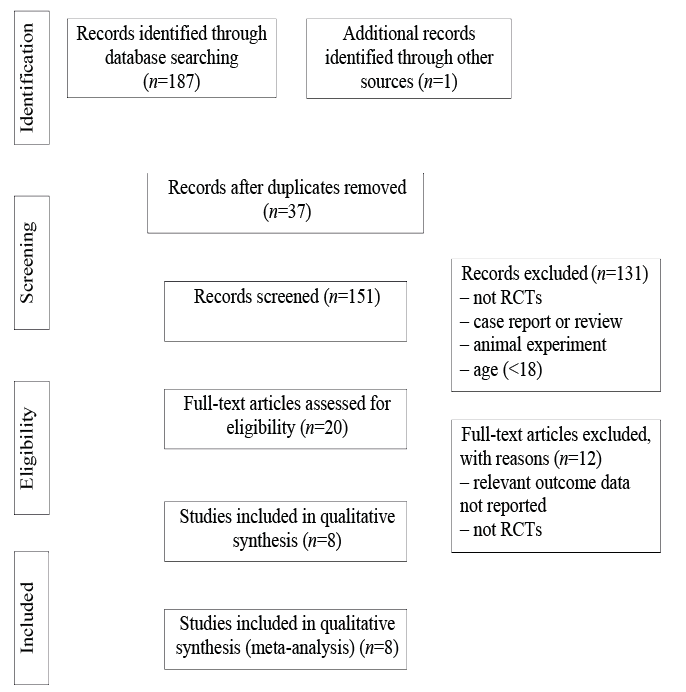
The literature search yielded 188 references, of which 37 were excluded because they were duplicates. After screening the titles and abstracts, 131 were excluded because they did not meet the inclusion criteria, and 12 were excluded after assessment of the full text because they did not meet the eligibility criteria. A final total of 8 RCTs (25–32) was included in this meta-analysis (Fig. 1). Among the 8 RCTs, 3 (26, 27, 29) tested the spasticity of the wrist and finger flexors, 3 (30–32) evaluated the spasticity of the ankle plantar flexor, 2 examined the elbow flexor (25, 30), and 1 (28) evaluated the external rotator muscles of the shoulder. The basic characteristics of these 8 RCTs are described in Table I, and risk of bias assessment of the included studies is shown in Fig. 2. Some studies provided two or more groups of analyzable data for meta-analysis.
Fig. 1. Flowchart for study selection. RCT: randomized controlled trial.
Fig. 2. Risk of bias of included studies.
MAS score after ESWT. Seven studies, including a total of 14 groups, used MAS to compare the spasticity grade between experiment group and control group (25–31). The results suggest that MAS grade was significantly decreased after ESWT (standard mean difference (SMD) = −1.22; 95% confidence interval (95% CI): −1.77, −0.66; z = 4.32; p < 0.001) (Fig. 3). However, considering the significant heterogeneity among the results (χ2 = 97.57, I2 = 86.7%, p < 0.001), sensitivity analysis was conducted after removing the study by Li et al. (29). The heterogeneity remained significant and the results were consistent with the initial results (SMD = −0.88; 95% CI: −1.27, −0.48; z = 4.38; p < 0.001).
Fig. 3. Forest plot of standardized mean difference (SMD) and 95% confidence interval (95% CI) in Modified Ashworth Scale (MAS) after extracorporeal shock wave therapy (ESWT).
MTS score after ESWT. A total of 2 studies (25, 30), including a total of 6 groups, provided analysable data for MTS. The pooled estimate of effect size suggested that, compared with the control group, MTS score was significantly improved after ESWT (SMD=0.70; 95% CI: 0.42, 0.99; z = 4.83; p < 0.001), with no significant heterogeneity among the studies (I2 = 47.2%, p = 0.091) (Fig. 4).
Fig. 4. Forest plot of standardized mean difference (SMD) and 95% confidence interval (95% CI) in Modified Tardieu Scale (MTS) after extracorporeal shock wave therapy (ESWT).
H/M ratio after ESWT. Only 1 study (32) used H/M ratio as the outcome measure in the analysis. A significant difference was found between active ESWT and sham ESWT (weighted mean difference (WMD) = –0.76; 95% CI: –1.19, –0.33; z = 3.48; p < 0.001) (Fig. 5). The results are consistent with the MAS and MTS.
Fig. 5. Forest plot of weighted mean difference (WMD) and 95% confidence interval (95% CI) in H/M ratio after extracorporeal shock wave therapy (ESWT).
Range of motion after ESWT. Four studies including 7 groups assessed the effects of ESWT on improvement of range of motion (26, 28, 31, 32). Compared with the control group, active ESWT had a significant influence on range of motion (SMD = 0.69; 95% CI: 0.06, 1.32; z = 2.15; p = 0.031) (Fig. 6). Significant heterogeneity was detected in the range of motion analysis. When a sensitivity analysis was performed by omitting the study by Fouda & Sharaf. (26), the heterogeneity decreased significantly and the results were consistent with the original analysis (SMD = 0.30; 95% CI: 0.03, 0.58; z = 2.14; p = 0.033).
Fig. 6. Forest plot of standardized mean difference (SMD) and 95% confidence interval (95% CI) in range of motion after extracorporeal shock wave therapy (ESWT).
Four weeks after ESWT. Only 3 studies (25, 28, 29) provided analysable data for MAS at 4 weeks after ESWT. There was no significant difference on the MAS grade (SMD = –1.73; 95% CI: –3.99, 0.54; z = 1.50; p = 0.135) (Fig. 7). Significant heterogeneity was found in the results (χ2 = 41.86, I2 = 95.2%, p < 0.001). A sensitivity analysis was conducted after removing the study by Li et al. (29), and the results were consistent with the original analysis, with no significant difference between experimental and control groups.
Fig. 7. Forest plot of standardized mean difference (SMD) and 95% confidence interval (95% CI) in Modified Ashworth Scale (MAS) at 4 weeks after extracorporeal shock wave therapy (ESWT).
Considering a significant level of heterogeneity in the results of the MAS grade, we conducted 4 comparative subgroup analyses to identify potential moderators or mediators that may affect statistical results, including: (i) frequency: > 5 vs ≤ 5 Hz; (ii) therapy site: muscle belly vs musculotendinous junction; (iii) total session: > 5 vs ≤ 5; (iv) treated muscles. However, because heterogeneity between the subgroups remained high (Table II), we cannot determine the impact of these factors on the results.
Table II. Subgroup analysis examining the impact of therapy protocol on the outcome of ”pre- and post- treatment Modified Ashworth Scale (MAS) scores”
This systematic review and meta-analysis included 8 RCTs that compared active ESWT with sham ESWT, including 385 participants with post-stroke spasticity. ESWT was used as a monotherapy or in conjunction with medication and/or physical therapy as adjunctive treatment for spasticity in stroke patients. The results suggest that active ESWT is significantly superior to sham ESWT for treatment of spasticity in post-stroke patients. Since significant heterogeneity was observed in this analysis, some subgroup analyses were conducted to determine the sources of heterogeneity. However, subgroup analysis showed that the high heterogeneity was not caused by frequency, therapy site, total sessions, or muscles treated. We speculate that the heterogeneity may be due to differences between trials; e.g. individual difference, time after stroke, type of stroke, time of treatment, and degree of spasticity. Previous meta-analyses have demonstrated that ESWT is effective for treatment of spasticity in post-stroke patients. Guo et al. (21) used the MAS grade as measurement of spasticity, and did not consider factors that may affect the results, such as frequency, therapy site, total sessions, and treated muscles. Furthermore, there was a lack of RCTs among the included articles, which might limit its quality. The present study analysed continuous outcomes based on MAS, MTS, H/M ratio and range of motion, and conducted subgroup analyses to identify potential moderators or mediators.
Although ESWT is effective for the treatment of spasticity in post-stroke patients, the mechanism is unknown. Previous studies have suggested that ESWT may affect the production of nitric oxide (NO) (33), spinal cord excitability (34), reduce muscle fibrosis (35), or affect the Golgi tendon (25). ESWT can induce synthesis of NO, which plays a role in the neuromuscular junctions of the peripheral nervous system and is involved in neurotransmission, memory formation, and synaptic plasticity in the central nervous system (17). However the main results are based on MAS score, which reflects exaggerated spinal reflex activity and increased stiffness of the muscles and other tissues. NO can increase muscle and tendon neovascularization, thereby improving muscle stiffness (36). NO may therefore play an important role in reducing spasticity and improving muscle stiffness. In addition, there are no significant changes in F-wave minimal latency and H-reflex latency after ESWT (27, 37); therefore, the effect of ESWT on excitability of the spinal cord and Golgi tendon can be excluded as the main mechanism.
ESWT involves multiple variables, and it is likely that the optimum protocol for this therapy is yet to be determined. Further research should therefore explore new protocols in order to improve the anti-spastic effects of ESWT. Li et al. suggest that receiving 1 session of rESWT per week for 3 consecutive weeks could yield stronger and more lasting benefits (29). Bae et al. showed that the treatment effect was greater in the musculotendinous junction group than in the muscle belly group (25). rESWT has been reported to be superior to fESWT for treating plantar fasciitis and improving the ankle passive range of motion and plantar contact area (38). However, it is unclear whether a higher treatment dosage (e.g. > 1,500 shots), or higher treatment frequency (e.g. > 12 Hz) is more effective for treating spasticity in post-stroke patients. Thus, further studies or systematic studies are required to explore which parameters of ESWT are the most efficient for spasticity in post-stroke patients.
The current study has several limitations. First, significant heterogeneity was detected in the meta-analysis. Secondly, the total number of RCTs and the total number of subjects evaluated are relatively small. Thirdly, relevant data are limited to assessing the longer-term outcomes of ESWT in the acute and chronic treatment of spasticity in post-stroke patients. Fourthly, the measurement of spasticity based on MAS and MTS is not sufficient, and another assessment method, such as H/M ratio, is necessary. Finally, only studies published in English were included, which may have resulted in bias. Based on those limitations, future clinical studies on ESWT should focus on: (i) investigation of larger and more representative RCTs; (ii) including a sufficient number of stroke patients with spasticity; (iii) determining the optimum protocol for ESWT to ensure it is most efficient in the short and long term.
This meta-analysis shows that ESWT can ameliorate spasticity effectively in post-stroke patients. However, due to the heterogeneity and small sample size in this study, these results need to be further confirmed in larger, multicentre RCTs. Further research should also focus on the optimum stimulation parameters in ESWT, in order to develop effective treatment strategies for spasticity in post-stroke patients.
This study was funded by Xuzhou Science and Technology Project (KC17177)
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize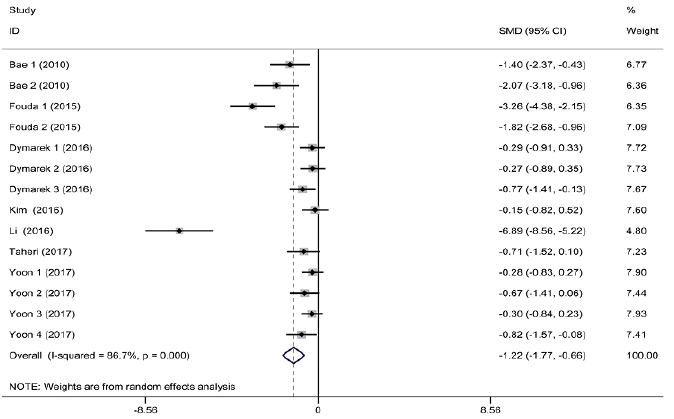 Click to show fullsize
Click to show fullsize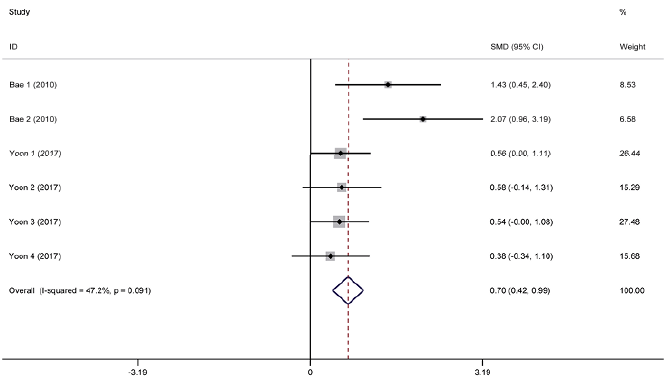 Click to show fullsize
Click to show fullsize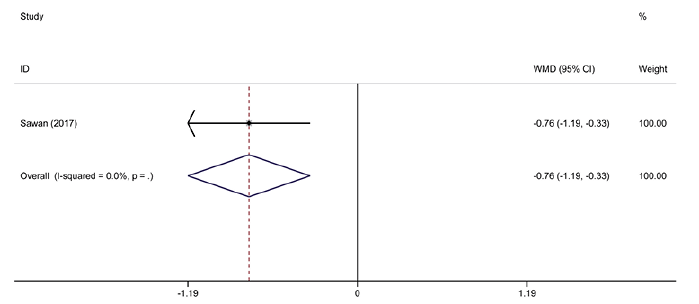 Click to show fullsize
Click to show fullsize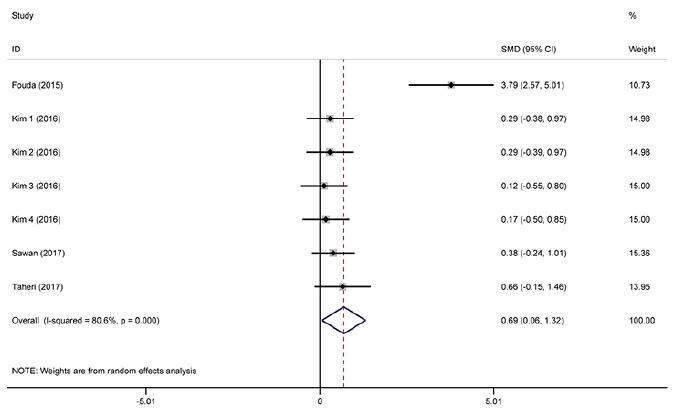 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize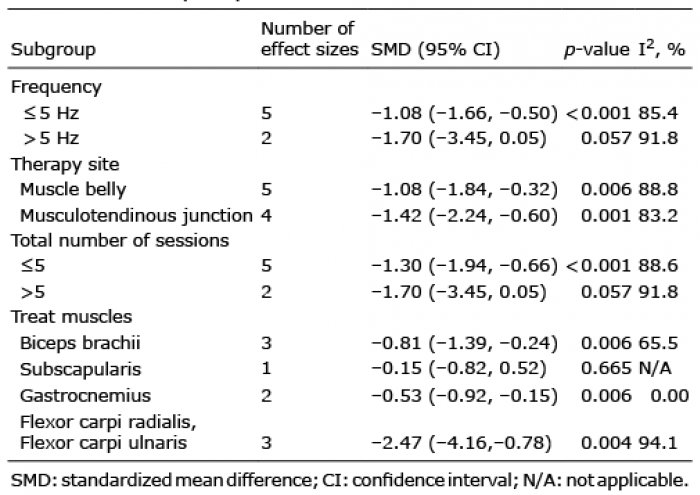 Click to show fullsize
Click to show fullsize