
From the 1Faculty of Medicine and Health Sciences, Department of Rehabilitation Sciences and Physiotherapy, Occupational Therapy Programme, Ghent University, 2Department of Occupational Therapy, Artevelde University College, 3Department of Physical and Rehabilitation Medicine, University Hospital Ghent, 4Faculty of Psychology and Educational Science, Department of Personnel Management Work and Organizational Psychology Ghent University, Ghent University, and 5Department Gerontology and Frailty in Ageing (FRIA) Research Group Vrije Universiteit, Brussels, Belgium
Background: Rehabilitation services are increasingly targeting involvement in daily life. In the International Classification of Functioning, Disability and Health this is referred to as “participation”. How-ever, questions have arisen regarding the conceptualization of participation, and consensus is lacking.
Methods: The first phase of this study is a critical review of the literature to detect recurring conceptual problems in the application of participation and how researchers deal with these. The second phase is a systematic review to identify how participation measures are operationalized.
Results: The critical review found possible solutions to 4 recurring key limitations: (i) how to deal with ambiguity and vagueness regarding the term “participation”; (ii) how to differentiate between activity and participation; (iii) what is the current empirical knowledge about the subjective aspects of participation; (iv) what are the different ways to measure participation. The systematic review found 18 instruments operationalizing participation in different ways: (i) unidimensional: frequency of performing activities; (ii) unidimensional: limitations in experiencing participation when performing activities; (iii) multidimensional: multiple subjective dimensions when performing activities; and (iv) multidimensional: objective and subjective dimensions.
Discussion and conclusion: Notwithstanding an increasing body of knowledge, some issues remain unclear and how participation is measured is subject to debate. This results in difficulties in the use of participation in clinical practice. However, insight into the current body of knowledge and awareness of shortcomings might help clinicians who aim to apply participation in practice.
Key words: World Health Organization; social participation; classification; participation; limitations, WHO; ICF; measures; concept.
Accepted May 8, 2018; Epub ahead of print Jun 26, 2018
J Rehabil Med 2018; 50: 00–00
Correspondence address: Dominique Van de Velde, Faculty of Medicine and Health Sciences, Department of Rehabilitation Sciences and Physiotherapy, Occupational Therapy Programme, Ghent University, De Pintelaan 185, BE-9000 Gent, Belgium. E-mail: dominique.vandevelde@ugent.be
Participation is defined by the International Classification of Functioning, Disability and Health (ICF) as “involvement in a life situation”’. For this concept to be used in rehabilitation, some issues require clarification. When aiming to use this concept and to measure participation it is necessary: (i) to define the context (home, school, work, community, etc.) in which the patient (child, adult or older person) wants to participate; (ii) to make clear in what dimension exactly one wants to measure participation: the frequency, the limitations, the subjective appraisal of activities, or combinations of these; and (iii) to be aware of the level of power and autonomy the patient aims for in performing activities: from being informed about the activity to being involved in decision-making. Based on the results of this study, a more informed choice could be made about which measurement instrument to use. However, a clear single agreement on the concept of participation will foster clinical practice and action is required to reach consensus.
Rehabilitation service providers are increasingly interested in improving social functioning and regaining performance in the daily lives of their patients. Within the World Health Organization (WHO) International Classification of Functioning, Disability and Health (ICF), this domain is referred to as “participation” (1).
Participation has become a feature of contemporary rehabilitation services, and this has been induced by changes in society. Traditionally, health policy was based on a biomedical model, in which disability was considered as a problem within the person, directly caused by disease, trauma or health conditions (2, 3). This biomedical concept of disability has been criticized and has failed in terms of society’s current vision on health, illness and disability (4, 5). There is increasing acceptance that health and disability are determined not merely by behavioural, biological and genetic factors, but also by a range of economic, environmental and social factors (6). The growing emphasis on social determinants has necessitated a new way of theoretical thinking about fundamental issues in healthcare and welfare, and has created a shift towards a social model of illness, in contrast with the biomedical model (7, 8). This social model focused primarily on the causation of disability by society. It originated from the work of disabled activist groups (9, 10) and theory about the normalization principle (11). However, this reasoning from purely a social perspective has also been the subject of criticism. Different authors have criticized this excessively narrow focus of illness (biomedical or social) and have offered a holistic alternative to the prevailing biomedical and social models (11–13). The various dimensions of illness (biological, psychological and social dimensions) were emphasized, and this created a new model; the bio-psycho-social model (14). From this moment, concepts such as community integration, inclusion, customer-orientation and autonomy became pivotal in clinical and scientific reasoning in rehabilitation (15).
These societal changes were also clearly visible in WHO decisions and policies and were expressed in their reports. In 1976; the World Health Assembly of the WHO responded to the biomedical-oriented approach to health by approving the publication of a classification instrument incorporating the social model (16). The result of this decision was the publication of the International Classification of Impairments, Disabilities and Handicaps (ICIDH), in which the role of environmental factors in the process of disablement was recognized (17). Despite the intention to shift away from the biomedical model, the ICIDH failed to provide a flexible tool for guiding research and data collection in all aspects of disability; the social aspect was never operationalized (16), there was lack of attention to the environmental impact, there was cultural bias and lack of clarity about temporal and causal relationships (18). Therefore, in 1993, the WHO started revising the ICIDH in order to counter these criticisms, and developed the ICIDH-2. In this new version, each dimension of disablement was conceptualized as an interaction between individuals and their social and environmental factors, and a separate list of environmental factors was added. In addition, the terminology was adapted: impairments remained the same, but disability became activity limitations and handicap was changed to participation restrictions. The term participation was described for the first time and was used to “identify the nature and extent of a person’s involvement in basic areas of human life” (16). The ICIDH-2 embodied and operationalized a bio-psycho-social model: a synthesis of the medical, psychological and social approaches to disability. This revised version was presented to the WHO Executive Board in January 2001, and finally evolved into the ICF (1), in which the negative connotation of the components were changed: impairments was replaced by body functions and structures, activity limitations was changed into activities, and participation restrictions was replaced by participation. Participation was defined as “involvement in a life situation” and was clarified by “the lived experience in the actual context in which people live” (1).
The authors of the ICF conceptualized participation as the actual performance of activities in a real-life context: “from the mundane (taking care of one’s physical appearance) to the highest planes of human existence (education, employment, etc.)” (16). At that time, this way of looking at disability was revolutionary because it overcame the negative connotation of disability and focused on the understanding of health that incorporates a relationship between people’s daily life and health.
Since its publication in 2001, the term participation, defined as involvement in a life situation, has been translated into different languages, and most translations exactly match the original English. For example, involvement in life situation is translated literally as “engagemanget i livssituationer” in Swedish, “il coinvolgimento in una situazione di vita” in Italian and “Einbezogensein in eine Lebenssituation” in German. In French, a little nuance emerged in the translation, since they added the word “réelle” (real) to life situation: “l’implication d’une person dans une situation de vie réelle” (literally, involvement in a “real” life situation). This nuance clarifies that it is about a real-life situation, but it stays close to the original definition. However, the Dutch collaborating centre has translated involvement in a life situation as “deelname aan het maatschappelijke leven”, which literally means “taking part in social life.” This latter definition differs somehow from the original and has a different connotation, because it brings in a social component and interprets involvement as taking part. These cross-cultural differences in the translation of the original English term might reflect a bias or a particular interpretation by local authors or translators, and shows that there is room for discussion regarding the conceptualization of participation.
However, incorporating the concept of participation in contemporary reasoning in clinical rehabilitation offered opportunities to consider patients’ goals, needs and preferences in their therapy plans. Thus, and notwithstanding the differences in the translations, the concept of participation has been used increasingly in clinical work, education and research (19). After 16 years of use, it has also been thoroughly investigated and critiqued worldwide (20). As a consequence, the body of knowledge is increasing, but this goes hand-in-hand with criticism. It is generally known that there are 4 important recurring limitations with regard to the concept of participation described in the literature: (i) there is ambiguity and vagueness about the term itself (21–23); (ii) differentiating between activity and participation remains unclear (24–28); (iii) the subjective aspects of participation are missing (23, 29); and (iv) there is no consensus about how to measure participation (23, 26, 30–36). These limitations, which are somewhat inter-related, hamper the application of participation in clinical practice. For example, when professionals are asked to work towards participation, they experience difficulties in how to focus on participation and intertwine participation with related concepts, such as working towards social engagement, more patient involvement in the therapy or decision-making process, community integration, independency, autonomy or perhaps a combination of these. These difficulties are apparent in the literature (37–40) and when participation is measured, because different measures result in different outcomes (41).
It is not relevant to focus only on the limitations of this concept; in order to move forwards it is more appropriate to focus on how to deal with these limitations in practice. The aim of this study is therefore to gain an overview of how researchers and clinicians deal with the recurring limitations of the concept of participation and to determine how it is operationalized and how it can be applied.
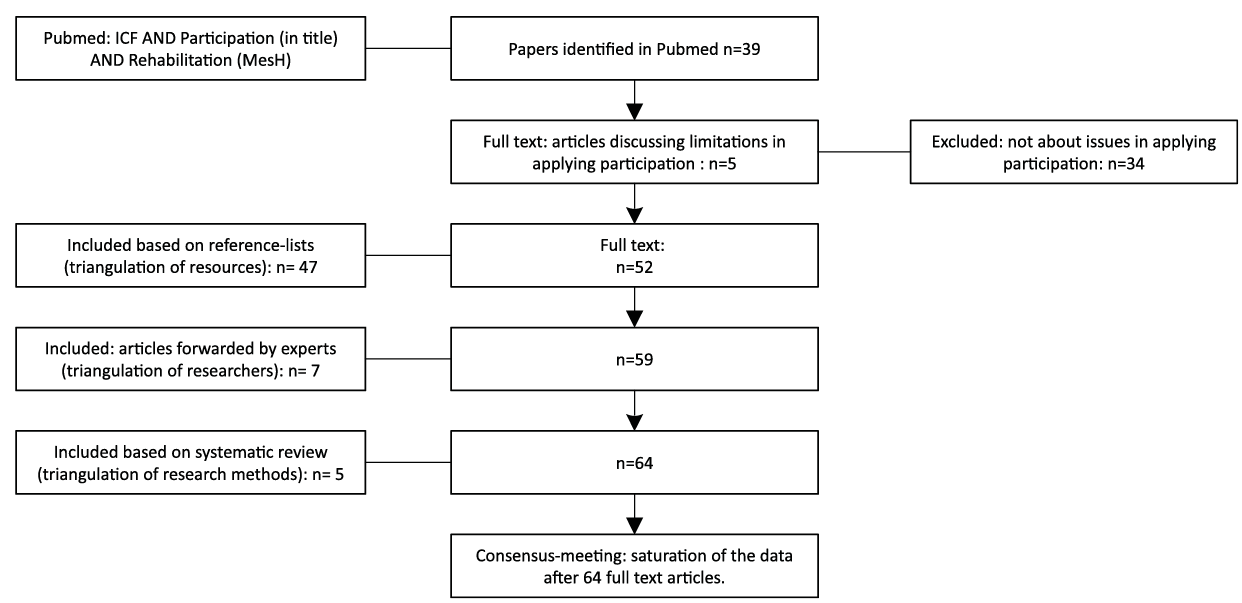
A 2-fold method was used, comprising a critical review of the rehabilitation literature and a systematic review of the existing instruments for measurement of participation. In the first phase, a critical review (42) of the rehabilitation literature between 2001 and 2017 was performed to clarify current limitations to the application of the concept of participation, and to determine how professionals deal with these issues. A search of PubMed was performed, using the following key words: ICF AND participation (in the title) AND rehabilitation (MeSH); the latter term was chosen to limit the scope of the search to the field of rehabilitation medicine. PubMed was chosen as the only search engine because it is primarily oriented to medical and paramedical content and is used most frequently by specialists in rehabilitation medicine to retrieve information. In addition, the study focused solely on medical and paramedical discourse on the concept of participation, in order to determine how these professionals cope with the recurring limitations. All retrieved articles were read and analysed to gain a clear idea of the content. Specifically, the study searched for issues in applying the concept of participation in a rehabilitation context.
The critical review is characterized by the iterative process of adding new knowledge and information until saturation was reached. The process of saturation was characterized by 3 main features; triangulation of: (i) resources, (ii) researchers, and (iii) research methods. The references in the selected articles were checked for additional articles, which were also analysed. From this point on, literature from adjacent research fields and literature from before 2001 was also included, when relevant to the rationale of this review. Articles that included new knowledge were added to the list; articles concerning already-known information were withheld, but only to confirm the already-known information. When 2 or more articles confirmed the already-known information, only the most recent was withheld. A second aspect of saturation is the triangulation of the researchers with expertise in applying participation. After the first author, with research expertise in participation, 3 of the researchers in this project (with expertise in children: 2nd author; adults: 3rd author; and older adults: last author) were asked to read the gathered information critically and determine whether possible published information was missing. If information was missing, the experts were asked to forward articles. Thirdly, this first phase was carried out in triangulation with the second phase (see section below: Phase 2: a systematic review). The second phase was used to confirm acquired information and to determine whether other ways to operationalize participation should have led to further searches. In that case, the articles from the systematic review were added to the list. Constant peer debriefing with the research group and a final consensus meeting led to an agreement regarding saturation. Considering this triangulation of multiple resources, different researchers and 2 different research methods, this review can be considered as a stock-take of accumulated knowledge of the concept and solutions for shortcomings.
In the second phase, a systematic review (42) of instruments for measuring participation was conducted to determine how participation is operationalized. In order to capture the concept of participation, the search was limited to dates between 1998 (to include instruments based on the ICIDH-2) and 2017. The review focused on articles in which instruments are described that were intended to measure participation based on the ICF definition. Consequently, there was only one criterion: “referring to the ICF definition of participation of the WHO in the development process.” In order to detect these articles, the following key words were used in PubMed: ICF AND participation AND measure (OR scale OR instrument OR rating OR assessment OR test). Articles were selected when it was indicated in the title and abstract that the article described the development and validation of an instrument for measuring participation. Kappa statistics were applied in this phase to check agreement in the selection between the first and the third author (of this study), and was defined as > 0.70. After this phase, the full articles were read by the first and third author, and further selection was performed in consensus. If there was more than 1 article about a specific measure, only the article published first was retained. Furthermore, articles were included only if the word participation appeared clearly in the name of the instrument. If the title of the instrument narrowed the concept of participation to social participation, community participation, sports participation, etc., these articles were excluded. If the instrument was not available in English, the article was also excluded. After the final selection, an analysis of the content of the included instruments was carried out to clarify how the concept of participation is comprehensively represented in the questionnaire, with reference to Guyatt et al. (43) and Terwee et al. (44). The goal of this analysis was to clarify different aspects of the measures; specifically to elucidate: (i) the different dimensions in the scales and whether the scales are divided into different subscales; (ii) the different items in the (sub)scale(s); (iii) the way the (sub)scale(s) is (are) operationalized; (iv) the questions that were asked in the different subscales; (v) the different answer options in the (sub)scale(s); and (vi) whether all ICF domains were covered.
The authors with expertise in applying participation (children: second author; adults: first and third author; and older adults: last author) were asked to analyse the measure based on the above-described features. To check whether the analysis was performed accurately, the 4 authors confirmed each other’s analyses and added information, if necessary, in a consensus meeting. Thus, the study aimed to provide an overview of the diverging operationalization of participation appearing in the instruments claiming to measure participation.
In this critical review saturation appeared after analysing 64 articles and a subsequent consensus meeting with the research group (Fig. 1).
Fig. 1. Flow chart of the selection procedure for the critical review.
As described in the introduction, there are 4 recurring limitations of participation. These limitations are used as a lever and provide the structure for this section. They guide the inventory of the results of our critical review. The focus is, however, on possible solutions to these problems, as described in the literature.
Possible solutions to deal with ambiguity and vagueness about the term participation. Participation, or “involvement in a life situation”, is considered a key contributor to health and well-being regardless of age, pathology, culture and gender, but it is difficult to implement in clinical practice due to lack of clarity in the definition (26). Dijkers clarifies why this definition is not useful in its current form and argues that “everything we do between being born and dying is involvement in a life situation” (24). However, by explaining what constitutes involvement and what constitutes a life situation, it is possible to overcome this problem (45); 3 ways have been described in the literature and are described below.
One way to overcome this problem is to add an adverb to the noun participation. Therefore, in most cases, different authors add an adverb explaining the geographical or social context of the life situation or the specific action of the involvement. The following descriptions exemplify the reference to the context or the actions. They range from very broad descriptions, such as community participation (34), social participation (46), participation in society (47), societal participation (48), participation in activities (33), occupational participation (49, 50), social involvement (51) and socio-occupational participation (50), to more detailed descriptions, such as sociopolitical participation (52), citizen participation (53), school participation, labour participation (54), student participation, sports participation, patient participation (55), etc.
As a result, participation, or the life situation in question, becomes less vague. Heinemann and colleagues endorse this method to overcome vagueness and suggest conceptualizing participation as concentric circles of “world, nation, community and home” (37), thereby allowing participation to be viewed as individuals engaging in their own context of life and referring to the work of Bronfenbrenner, in which individuals live in a micro, meso and macro world (Fig. 2).
Fig. 2. Concentric circles of contexts in which participation can be experienced, based on Heinemann et al. (37).
Furthermore, this way of thinking about participation can be applied within different contexts. There is already a lot known about where individuals experience opportunities to participate. For example, in the older population, an important locus for experiencing participation (besides the community) is in their own home (56) or nursing home (57, 58). For younger adults, another place (other than home) to experience feelings of participation is primarily the work-community (59); in children, school is considered an important locus for experiencing participation (60). Specifying the context offers possibilities to operationalize participation.
A second way to overcome the vagueness of defining participation is to clarify the aspect of involvement by referring to the level of power that individuals possess, often referred to as the participation ladder (Fig. 3), originally published by Arnstein (61).
Fig. 3. The participation ladder (Arnstein et al. (60)). (1) Manipulation and (2) Therapy. These 2 rungs describe levels of “non-participation” that have been contrived by some to substitute for genuine participation. Their real objective is not to enable people to participate in planning or to conduct programmes, but to enable powerholders to “educate” or “cure” the participants. (3) Informing and (4) Consultation. These 2 rungs describe the levels of “tokenism” that allow the have-nots to hear and to have a voice: when they are proffered by power-holders as the total extent of participation, citizens may indeed hear and be heard. However, under these conditions, they lack the power to ensure that their views will be heeded by the powerful. (5) Placation is simply a higher level tokenism because the ground rules allow have-nots to advise, but to retain for the power-holders the continued right to decide. Further up the ladder are levels of citizen power with increasing degrees of decision-making clout. Citizens can enter into a: (6) partnership that enables them to negotiate and engage in trade-offs with traditional power-holders. At the topmost rungs, (7) Delegated Power and (8) Citizen Control, have-not citizens obtain the majority of decision-making seats, or full managerial power (Arnstein, et al. (60)).
This ladder shows that participation can range from being manipulated in performing activities (no participation) to possessing total control and decision power over the activities (full participation). This way of looking at participation stems from the goal to provide more power to the citizen in the community through their involvement in activities, often referred to as citizen participation, but has also been shown to be applicable in healthcare and rehabilitation (62). Tritter argues that it is individually defined, based on whether a person wants to be in charge and wants more power (as the highest rung on the ladder) or can generally reconcile him- or her-self to a lower rung on the ladder where he or she is informed about decisions that have been made (62). Both ways can be satisfactory for the individual, depending on how the individuals perceive their desired level of power, and from this perspective, the participation ladder is a possible way to operationalize involvement (63).
A third way to clarify participation is by thinking of life situations as life roles, thereby linking participation to the roles that people fulfil in society (e.g. mother, engineer, dancer, etc.) and the possibility of switching between these roles throughout their lifespans. Thus, the activities that individuals have to perform are placed in a broader perspective, which emphasizes participation (64, 65). Operationalizing participation as life roles has been applied in recent studies regarding, for example, stroke (66), traumatic brain injury (67) and older adults (68).
How to differentiate between activity and participation. In the ICF, the concepts of participation and activity are amalgamated in a single list covering the same 9 domains: [d1] learning and applying knowledge; [d2] general tasks and demands; [d3] communication; [d4] mobility; [d5] self-care; [d6] domestic life; [d7] interpersonal interactions and relationships; [d8] major life areas; and [d9] community, social and civic life. These domains are qualified by 2 qualifiers: capacity and performance. The capacity qualifier refers to an individual’s ability to execute a task and aims to indicate the highest possible level of functioning that a person may reach in a given domain at a given time (1, p. 15). The performance qualifier describes what an individual does in his or her current environment (1, p. 15).
In the ICF (1), activity is defined as the execution of a task or an action by an individual, while participation is, as described above, defined as involvement in a life situation. When applying the principles from the ICF regarding capacity and performance, the distinction is clear; the activity is on the level of the individual; what he or she can do, regardless of the environment, in other words, capacity. If and when the environment is considered, it is about involvement, i.e. “participation”. However, some authors argue that there cannot be an action without involvement in a life situation (69). This issue is considered the most important in the literature when examining this problem from the perspective of semantics, nomenclature and psychometrics, but is disputable given the clear difference proposed by the ICF if applying capacity and performance qualifiers correctly. In annex 3 of the ICF (1, p. 250), 4 different options are proposed to differentiate between activities and participation: (i) designating some of the domains to activities and others to participation, allowing no overlap (e.g. the domain learning and applying knowledge is designated as activities and the domain civic life is designated as participation); (ii) designating some of the domains to activities and others to participation, allowing partial overlap; (iii) designating all broad categories of the domains as participation and all detailed categories as activities; and (iv) designating all domains to activities or participation, depending on how the user defines activity or participation. Researching how the terms activity and participation can be distinguished from each other in the context of the ICF is one of the aims of WHO, as stated earlier (1).
Magasi & Post (70) reported that the majority of researchers agree that some domains belong to activities and others to participation and that the cut-off between activity and participation is somewhere between [d4] mobility and [d6] domestic life. However, this agreement is based on theoretical assumptions. Jette and colleagues examined the boundaries of the activity and participation domains of the ICF (27, 28). They reported the first empirical evidence of separate activity and participation dimensions (28), but in a follow-up study they concluded that a distinction between activity and participation could not be identified (27). Van de Velde and colleagues empirically proved that every activity ranging from [d1] to [d9] can be the trigger to experience participation (71). On the one hand, they provided evidence that both concepts belong to the same chapter in the ICF; on the other hand, there is a fundamental difference between them. The difference seems to depend on the individual’s subjective appraisal of the activity (71, 72). No further empirical evidence is yet available, but a lot of opinions and discussions from experts on the topic add to this body of knowledge and fit the above-described view that participation refers to the subjective aspects such as the level of engagement (69, 71, 73). These studies shed new light on the conceptual distinction between the concepts activity and participation.
Current empirical knowledge about the subjective aspects of participation. Subjective aspects are personal perceptions regarding performed activities; for example, the patient’s satisfaction with activities. Although there is a lot of discourse that the subjective aspects are missing in the ICF (23), this is not entirely true because the ICF provides the possibility to qualify participation with a qualifier that indicates an experienced problem or with a qualifier that indicates the level of satisfaction (1). Therefore, it is more correct to state that both the “experienced problems” and the “satisfaction level” are not operationalized in subjective variables, instead of arguing that the subjective aspects are completely missing. Following the limited empirical evidence described above about the difference between activity and participation, a great deal of research has been done regarding the subjective aspects of participation (21, 40, 50, 56, 74–80). These studies offer some evidence on how participation is perceived or experienced by individuals with and without a disability. The overall conclusion of these studies is coherent: participation cannot be defined purely as objective aspects, such as the amount of activities that individuals perform or the capacity individuals have to perform activities (50), but rather as a cluster of subjective variables and experiences, such as being able to choose activities, experiencing challenges, experiencing control by performing activities, experiencing engagement, having responsibilities, experiencing autonomy, experiencing meaningfulness, sense of belonging, etc. Participants in these studies elaborated on the importance of the social context they belong to, in which they feel safe and secure, and on the variety of activities that were important to them. A recent configurative review came to the same conclusion and recommends incorporating subjective perceptions of autonomy, sense of belonging, challenge, engagement, mastery and meaning associated with participating into the conceptualization and operationalization of the participation construct (81).
Different ways to measure participation. There is ongoing debate on how to rate or measure participation (36), and this might be considered as an external expression of the preceding 3 recurrent limitations and accompanying discussions regarding the WHO definition of participation (26, 82, 83). Systematic reviews on participation measures have been conducted and already a huge body of knowledge is available on how participation instruments are operationalized. A recent review from Ballert et al. shows 41 different instruments to measure participation (84) and includes instruments that clearly aim to measure participation, as defined by the ICF, such as the Participation Scale (P-scale) (85), the Participation Objective, Participation Subjective (POPS) (86) and the Keel Assessment of Participation (KAP) (87). These reviews, however, also include instruments that measure juxtaposing constructs, for example: health-related quality of life measures, such as the MOS Short-Form Health Survey (SF-36) (88); functional status instruments, such as the Functional Independence Measure (FIM) (89); community integration measures, such as the Community Integration Questionnaire (CIQ) (90); measures of life habits, such as the Life-Habits questionnaire (91); and measures of limitations in daily routines, such as the Late Life Function and Disability Instrument (LLFDI) (92, 93). In older reviews (70, 94–96), similar adjacent constructs were included next to the exclusive participation instruments. Including these adjacent constructs in the reviews shows the conceptual overlap with other related constructs, such as community integration, life habits and quality of life. In all of these reviews, the authors discuss the fact that there is a grey zone and that they experienced difficulties in selecting instruments. They argue for including adjacent constructs because participation aspects are included in these instruments, sometimes in subscales or sometimes because single items in the scale are related to participation (84, 97). The rationale to do so is clear and defendable, but also raises questions. Without questioning the value and scientific rigour of these studies, it limits clinicians’ abilities to make a clear choice. It entails the insidious risk that clinicians are confusing level of participation with functional independence, health-related quality of life, community integration or something else. To clarify exactly how participation measures are operationalized based on the WHO definition, a systematic review of PubMed was performed in phase 2 of this study.
This section discussed how participation is operationalized in measurement instruments. The literature search resulted in 1,266 articles (ICF AND participation AND measure: n = 225; OR scale: n = 192; OR instrument: n = 109; OR rating: n = 52; OR assessment: n = 438; OR test: n = 250) (Fig. 4).
Fig. 4. Flow chart of the selection procedure for the systematic review.
A total of 1,199 articles were excluded because development or validation of a participation instrument was not described in the title or abstract. This resulted in 67 articles being selected for further reading. A kappa of 0.93 (standard error [SE] 0.07) between the authors who performed the review showed almost perfect agreement. Thirty-six articles were excluded because they were follow-up articles of a previous article about the same instrument. Five instruments claimed to measure at the level of participation, but did not clearly indicate the name of the instrument and were excluded: the WHO-Disability Assessment Schedule 2.0 (WHO-DAS 2.0) (98, 99), the Life habits (Life-H) (91, 100), the Life habits for children (Life-H children) (101), the Community Integration Measure (102) and the Community Integration Questionnaire-Revised (CIQ-R) (103). Twenty-six instruments had participation in their title; 6 of which were excluded because of the combined words and narrowing the concept to social or community participation in the title: Australian Community Participation Questionnaire (ACPQ) (104), the Maastricht Social Participation Profile (MSPP) (105), the Activity & (community) Participation Questionnaire (APQ) (106), the Temple University Community Participation (TUCP) (107), the Community Participation Domains Measure (CPDM) (108) and the ICF Mental activities and Participation Measure (ICF-Mental-A&P) (109). Two instruments were excluded because they were not available in English: the Index zur messing von Einschränkungen der Teilhabe (IMET) (110) and the Mini Instrument for the observer rating according to ICF of Activities and Participation in Psychological disorders (MINI-ICF-APP) (111). Finally, 18 instruments were included (Fig. 3).
After scrutinizing these 18 instruments (Table I), the common ground is 2-fold: (i) every instrument uses activities as the vehicle to rate participation, and (ii) there is no discussion that participation is equated with performance because every instrument refers to performing activities in the actual environment of the individual and not what they can do in a standardized environment, which should be named, capacity, according to the ICF.
Table I shows a more detailed overview of how the 18 included measures are constructed and which of the 9 ICF domains they cover. The results were structured according to the way the instruments are operationalized: (i) unidimensional, the frequency of performing activities; (ii) unidimensional, the experienced limitations in performing activities; (iii) multidimensional, multiple subjective dimensions; and (iv) multidimensional, combining objective and subjective dimensions.
Unidimensional instruments: the frequency of performing activities. The Keel Assessment of Participation (KAP) (112) and the Participation, Patient Reported Outcome (PAR-PRO) (113) build on objective and normative standards (frequency and/or duration of performing activities) and have operationalized unidimensional participation through the frequency or duration of performing activities.
Unidimensional instruments: the experienced limitations in performing activities. The Participation scale (P-scale) (85), the ICF measure of Participation and Activities Questionnaire – screener part (IMPACT-S) (26) and the Oxford Participation and Activities Questionnaire (Ox-Paq) (114) are also operationalized as unidimensional, but as the perceived limitations or difficulties in performing activities. This is an attempt to rate participation based on a subjective appreciation.
Multidimensional instruments: multiple subjective dimensions. The Impact on Participation and Autonomy Questionnaire (IPA) (35, 115) has operationalized participation as multidimensional because this measure also includes the dimension of choice and control (hereby considering autonomy as an important aspect of participation). The Participation Enfranchisement instrument (PE) (116) also has operationalized participation as multidimensional and further includes being valued by others and the contribution to the community as dimensions. The Rating of Perceived Participation (ROPP) (117) has operationalized participation in 3 dimensions: perceived restrictions, satisfaction and the urge for support. Finally, the Time Organization and Participation Scale (TOPS) (118) has been constructed as the satisfaction to perform and organize activities within a normal time window.
Multidimensional instruments: combining objective and subjective dimensions. The shift from a uni- to a multi-dimensional assessment of participation also led to a growing tendency to operationalize patient-perceived measures, including both the objective and the subjective aspects of participation (47). For example, the Participation Objective, Participation Subjective (POPS) (86), the Participation Measure for Post-Acute Care (PM-PAC) (119), the Utrecht Scale for Evaluation of Rehabilitation – Participation (USER-P) (120), the Participation and Environment Measure for Children and Youth (PEM-CY) (121) and the Child and Adolescence Scale for Participation (CASP) (45, 122) include objective variables, such as frequencies and duration, and a set of variables to explain the perceived satisfaction or engagement in each activity performed. Consequently, these measures also operationalize participation as multidimensional, but include both types of variables, objective and subjective, although they keep them as separate dimensions. The Participation Survey/Mobility (PARTS/M) (123) follows a similar multidimensionality and includes, in addition to the frequency of performing activities, the aspect of choice and control in the measurement instrument. The Participation Measure – 3 domains, 4 dimensions (PM-3D4D) (124) also includes, in addition to the frequency and the diversity of activities, the desire for change and the perceived difficulty. Finally, the Ghent Participation Scale (GPS) (71, 72) is a multidimensional scale that includes 15 different subjective and 2 objective variables and combines them into a single overall score.
In addition, when looking at the operationalization and associations with the 9 domains of activities and participation in the ICF, all of these measures differ regarding the ICF (or ICIDH-2) domains covered (see also Table I). Only the GPS covers all 9 domains (71); other instruments do not cover all domains and they differ in the number of domains they cover (26, 85, 86, 112, 113, 117, 119, 120, 123). Some instruments claim to rely on the ICF, but have operationalized domains other than those described in the ICF (45, 114–116, 118, 121, 124, 125).
The ICF delivered a positively oriented international classification system for health and health-related domains and offered the advantage of providing a global language for health and disability (126). In particular, the concept of participation provides a resource for better understanding disability in the real context in which a person lives. Nowadays, it is argued that rehabilitation delivery strives to enable people to remain active, perform daily activities and participate in important life roles when they age (127, 128) or after they are affected by injury or disease (15, 129).
Researchers and clinicians, however, have raised a lot of questions regarding the concept of participation. The field has not yet reached a consensus, and there seems to be confusion about the concept because of the different interpretations and the different ways it is operationalized and measured. Therefore, this article is primarily intended to set out an overview of how researchers deal with these issues, through a critical review of the current knowledge and a systematic review of participation instruments.
Fortunately, there is already a huge body of knowledge, and if this knowledge is used wisely, the concept of participation offers opportunities to enrich clinical practice. Based on the professional and expert opinions described in the literature and the patient’s lived-experiences, it can be concluded that participation is indeed involvement in a life situation. Participation is multidimensional (comprising objective and subjective variables) and could be considered as an interdependent relationship between the individual’s specific activities performed (or in which they are involved) and/or their level of autonomy, and/or the roles they fulfil and/or the context in which they live.
Some aspects of participation remain unclear and further discussion or research is needed. Firstly, the variety of different interpretations (as evidenced by participation descriptors, such as community participation, social participation and sports participation) indicates that there is little agreement among researchers in conceptualizing participation. Without an adverb descriptor, the term participation is like an empty box. However, it also means that participation is highly individually defined and depends on the context in which people live. The concept of using concentric circles places the focus on the importance of environmental factors in relation to participation. It confirms that disability results from the interaction between the person and the environment (130), and it highlights the premise that participation can be understood as the “experience of people in the actual context in which they live” (1). Although the impact of the environment has been studied, there remains a need for a better understanding of the interaction of the environment and people’s experience of functioning in life, as stated by Stucki and colleagues (131).
Secondly, concerning the differentiation between activity and participation, a crucial aspect of any classification system or framework should be the ability to differentiate between juxtaposing concepts within the system (44), as provided by the ICF. However, many researchers have criticized this effort as confusing and even a backward step from earlier disability frameworks (27, 28, 69, 132, 133). As a result, an expert panel at the International Symposium on Measurement of Participation in Rehabilitation Research stated that the failure of the ICF taxonomy to distinguish clearly between activity and participation exacerbated the conceptual ambiguity about how to define and delineate participation (37). In addition, problems arise when trying to prove this differentiation empirically and, as there is currently no definitive answer, further research is necessary.
Thirdly, concerning subjective aspects of participation, common ground can be found mainly through qualitative research showing patients’ experiences that every activity can lead to participation. According to patients, this experience depends on the subjective appraisal attributed to the activity in relation to the environment in which the activity occurs. Based on this knowledge, there seems to be an agreement that the key to untangling “activity” and “participation” lies in the subjective appraisal of activities. Subjective appraisal highlights, once again, the importance of the “experience of people in the actual context in which they live” (1). Many studies have aimed to capture the subjective aspects of participation by supporting the call for including personal values in the coding system of participation in the ICF, the lack of which has led to criticism (22, 23, 72, 81). However, further empirical research is necessary. The debate is ongoing, and as long as there is no agreement about whether to include subjective aspects in the discussion about how to define participation, there is also no agreement on how to rate or measure it.
Fourthly, there is a wide variety of measures, allowing a choice of different instruments. At present, there is no consensus among researchers, nor a strong argument in favour of any one of the existing participation instruments. It remains difficult to choose an instrument when evaluating participation. In a study in which different instruments were used to measure participation, the authors concluded that “a lack of conceptual consensus makes participation an ambiguous concept in research, and this ambiguity makes evidence-based decisions directed at enhancing participation difficult” (41). Each of the authors of the instruments has a strong rationale for the way they operationalized participation and has validated them accordingly. Consequently, clinicians have to make their own choice to use participation in a unidimensional or multidimensional way. In this case, the use of a multidimensional instrument might offer more detailed information about the patient. This enables a patient-centred approach and offers opportunities for shared decision-making. The overview in Table I may enable clinicians to choose the most suitable instrument. The initial question for the clinician should be to determine exactly what they want to measure for a particular case or patient: frequency, duration, satisfaction, importance, choice, control, time organization, need for support, contribution to the community, desire for change, wishes, social appreciation, etc. Each of these dimensions and tools could have its value in the clinical setting. It depends, to a great extent, on the specific aim of the clinician in relation to the goal of the patient. Notwithstanding the lack of clarity on how to operationalize participation, there is no doubt that it is all about performance, and this consensus could be considered a strong point. Further research is needed to identify the items underlying the success or the failure of this performance.
PubMed was the only search engine used for both phases of the study. The search could have been expanded by also using Web of Science, Psych-Info, white books or grey literature. Thus, it is possible that a broader view of participation, e.g. from a more sociological or psychological point of view, was missed. It can therefore be questioned whether this study captured all biopsychosocial perspectives from PubMed, as this is primarily a medical database. In addition, by excluding grey literature, such as dissertations, new views and participation instruments may have been missed.
The critical review in this study provided an opportunity to take stock and evaluate what is known and what can be learned from this existing body of knowledge. A critical review may provide an incentive for a new phase of conceptual development of participation. However, a critical review also has some shortcomings; it emphasizes the conceptual contribution of each article and not the formal quality assessment, as in a systematic review or meta-analysis (42). It should be noted that the critical review is based on what was written in the literature, and thus cannot determine whether the researchers entirely understood the principles and philosophical background of the ICF. The review intended only to provide an overview of what was apparent in the discourse. Considering that this is a stock-take of the current knowledge and shortcomings until saturation was reached, it is not repeatable in the exact same way. Critical reviews do not typically demonstrate the systematics of other more structured approaches, such as systematic reviews. However, when repeating the study, the same results could be found, but perhaps referring to other authors. Therefore, the results of this critical review should be the starting point for further evaluation, and not an endpoint. It is hoped that this critical review will lead to further work on defining and operationalizing participation and will stimulate a more multidimensional, contextual approach to participation. In addition, in the search strategy for this review, ICF was used as a key word. Notwithstanding the fact that the term participation was used for the first time in the ICIDH-2, we did not include ICIDH-2 as a key word in this first phase, and this could have influenced the results. However, the ICIDH-2 and the rationale behind it emerged from the selected articles, since the ICIDH-2 has been referenced many times in these articles. Therefore, we consider the ICIDH-2 and the rationale behind it sufficiently covered.
In addition, there are some limitations in the systematic review of the instruments. First, we did not intend to duplicate existing systematic reviews on measurement instruments, since this has been done previously (62, 78, 85–86). We intended only to show the different ways of operationalizing the concept. Thus, we focussed only on the instruments that: (i) carried the word participation in their name; and (ii) did not narrow the concept to community or, for example, social participation in their title. This strongly limited the number of instruments included. Moreover, we excluded instruments claiming to measure, sometimes partly, participation. For example, the WHO-DAS 2.0 (89) was excluded for this reason. Nevertheless, the included instruments clearly show the differences in operationalization, which was the goal of this study. Secondly, we only performed a content analysis and not a quality analysis of the included instrument with regard to psychometric properties. For an overview of these properties, we refer to existing reviews (62, 78, 85–87), detailed articles about the instruments and specific articles in which psychometric properties of different instruments have been researched (134–137). In addition, the present study shows that there are different ways to operationalize participation, including different subscales, items and rating systems. This brings into question the overall content validity of each of these different measures. The content analysis in the present study was performed with limited experts in the field and did not lead to any quantitative appreciation of the content; therefore, it may be of interest to expand the methodology. Further research is necessary to determine whether the content of these measures is valid. For example, a broad group consisting of international experts with different professional backgrounds could be asked to rate each item from the instrument as “essential”, “useful” or “not necessary” and a content validity ratio (CVR) could be calculated for each of these instruments (138).
The two different reviews can be considered as separate parts. However, combining a study in which new articles are included until saturation appears with a study that starts broad and excludes studies based on clear inclusion and exclusion criteria has been shown to be complementary. On the one hand, the critical review confirms the results of the systematic review and vice versa; both studies reveal the remaining ambiguity of the concept and the need for further research. On the other hand, when considering the results in greater detail, both studies also reveal the possibility of applying the concept in a more rational way. The so-called vagueness of the concept, which has been discussed by many authors, can be considered an advantage because it offers opportunities for rehabilitation professionals to customize the concept to the needs of the patient and the needs of the rehabilitation centre. For example, the solution that has been offered to overcome the vagueness of the concept, by conceiving participation as concentric circles, is also visible in the measures that have included variables of the context (e.g. home, work, school) in which participation can occur. Combining the described limitations with the suggested solutions and aligning these with the most suitable measure offers more possibilities than limitations. This way of thinking can also be applied when using the concept of participation as an outcome in research.
Based on the above-described features (limitations and solutions to the application of participation in clinical practice), there is already a lot of knowledge, which has a strong focus on moving towards participation in physical and rehabilitation medicine. However, participation is only relevant when: (i) the other concepts in the ICF (health condition, body functions and structures, environmental and personal factors); and (ii) the correct use of capacity and performance qualifiers are considered equally in clinical practice. This paper is intended as a discussion paper and should also be considered as a call to all experts in the field, including measurement developers and scientific researchers, to combine their knowledge and expertise in order to find common ground in refining and further operationalizing participation. Clinical practice would be improved if there was a clear, single agreement on the precise meaning of participation.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize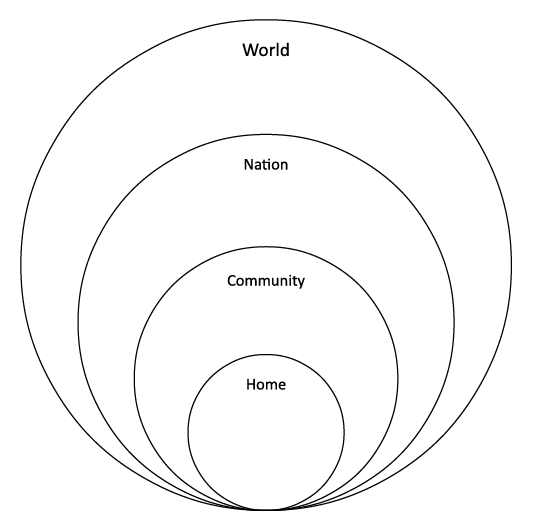 Click to show fullsize
Click to show fullsize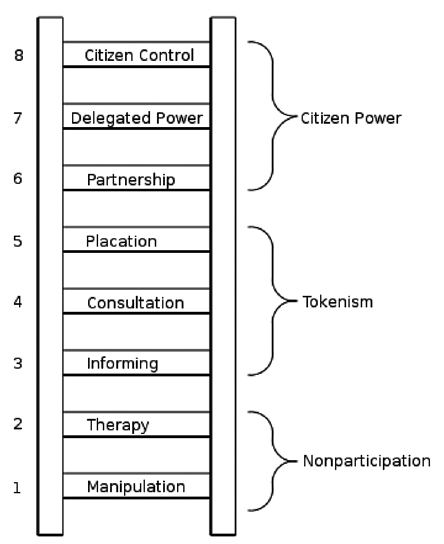 Click to show fullsize
Click to show fullsize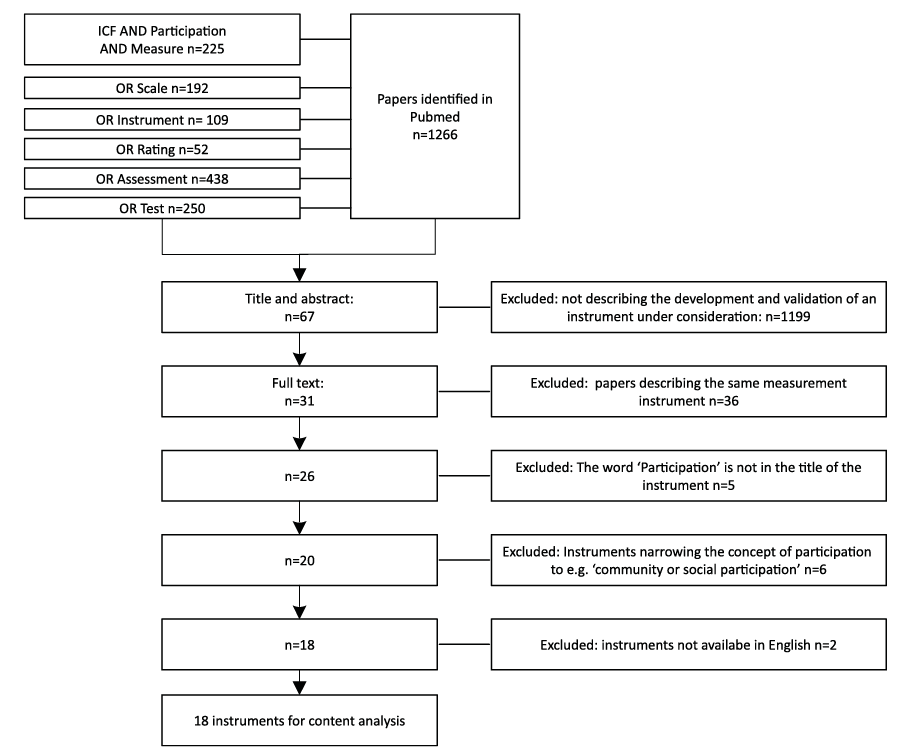 Click to show fullsize
Click to show fullsize