
From the 1Institute of Neuroscience, Department of Clinical Neuroscience, Rehabilitation Medicine, University of Gothenburg, 2Department of Medicine/Hematology and Coagulation, Coagulation Centre, Sahlgrenska University Hospital, Gothenburg, Sweden, 3Sunnaas Hospital, Oslo University, Norway, 4The Institute of Stress Medicine, Region Västra Götaland, and 5Health Metrics, University of Gothenburg, Gothenburg, Sweden
Objectives: To describe self-reported activity using the Haemophilia Activity List (HAL) for Swedish adults with haemophilia and to detect any changes over time.
Method: The HAL was sent to the adult population with haemophilia A and B, moderate and severe form, living in Sweden (n = 260). Participants completed the HAL and a questionnaire on sociodemographic and medical information. From a previous study cohort, 61 persons had responded twice to the HAL. The investigated group was divided into early and later treatment onset groups with regard to access to medication.
Results: The response rate was 50%. There was a significant difference (p < 0.001) between the early and later treatment groups in all domains in HAL. When analysing HAL “question by question” from the 2 reported time-points, the most prominent outcome was that the reported ability in activities was stable over time at the group level, except for participants who had no access to the clotting factor early in life. They reported greater limitations in some of the activities in the challenging domain “leisure activities and sport”.
Conclusion: The early treatment group reported a significantly better ability in all activities compared with the late treatment group.
Key words: haemophilia; activity; Haemophilia Activity List; longitudinally.
Accepted Apr 11, 2018; Epub ahead of print Jun 8, 2018
J Rehabil Med 2018; 50: 00–00
Correspondence address: Elisabeth Brodin, Institute of Neuroscience, Section for Clinical Neuroscience and Rehabilitation, The Sahlgrenska Academy, University of Gothenburg, Sweden, Per Dubbsgatan 14, 3 tr, Sahlgrenska University Hospital, SE-413 45 Gothenburg, Sweden. E-mail: elisabeth.brodin@gu.se
Compared with the very recent past, persons with haemophilia currently living in Sweden have the opportunity to have prophylactic treatment to avoid frequent bleeding episodes in their joints and muscles. This makes it easier to live an active life. Using a questionnaire on self-reported activity, younger adults reported fewer difficulties than older persons. Over time the older persons reported increased difficulties in some of the more complex activities, such as playing games, sports, and going on active holidays. One reason could be that the older persons had no medical treatment when they were young so they had arthropathy due to bleeding in their childhood, perhaps combined with problems due to ageing. It is important to capture the person’s own perspective of their abilities at their annual check-up.
There are approximately 1,000 males with haemophilia in Sweden (1), of whom 80% have haemophilia A and 20% have haemophilia B. Haemophilia A (factor VIII deficiency) and haemophilia B (factor IX deficiency) are divided into: severe (factor activity < 1%), moderate (factor activity 1–5%) and mild (factor activity 5–40%) forms (2).
The reported prevalence of haemophilia varies considerably among countries (3). For haemophilia A in high-income countries the reported prevalence is approximately 12.8 per 100,000 males, and for the rest of the world 6.6 per 100,000 males (3). For haemophilia B the corresponding prevalence for high-income countries is 2.69, and for the rest of the world 1.20 (4). Approximately 50% of persons with haemophilia (PWH) have either the severe or moderate form (5).
PWH in Sweden have had access to clotting factor concentrates for on-demand treatment as well as prophylactic treatment since the 1960s (6, 7). PWH born in the late 1960s had the opportunity to begin prophylactic treatment early in life (8). This had a major impact on joint status for PWH in the 1970s, giving young PWH the ability to live an almost normal life due to minimal joint damage (7). For older PWH, prophylactic treatment prevents the progression of joint damage (7). The Haemophilia Treatment Center (HTC) follows up PWH throughout life with annual checks/follow-ups of their medical treatment (9). However, until recently, only their medical treatment and joint status has been the focus of the follow-ups. A study of health-related quality of life (HRQoL) using the Short Form Health Survey, SF-36, from the Malmö Centre showed that PWH who had started prophylactic treatment later in life also had to cope with disability due to haemophilia arthropathy, but there was a trend showing that, after orthopaedic surgery, HRQoL improved in many domains of the SF-36 (10). The studied PWH, 35–64-year-olds, compared with a control population of Swedish males showed significant differences in quality of life (QoL), being worse in some of the SF-36 domains, unlike the younger PWH (age < 35 years) and older PWH (age 64–75 years), who reported no significant differences (10).
There is a lack of follow-up studies of activity and participation for adult PWH. One study tried to recall limitations and disabilities before orthopaedic multiple joint procedures, using the McMaster Toronto Arthritis Patient Disability Questionnaire (MACTAR) to compare long-term outcome and post-operative disabilities, but they stated that there was a lack of adequate instruments to measure participation (11). There are difficulties in comparing different populations due to varied conditions, both in terms of healthcare, laws, and cultures (12).
The Haemophilia Activity List (HAL) (13) is a disease-specific questionnaire that has been developed to assess the functional health status of PWH according to the International Classification of Functioning, Disability and Health (ICF), in chapters; 4 “Mobility”, 5 “Self-care”, 6 “Domestic life” or 9 “Community, social and civic life” (14). The ability of the HAL to detect clinically important changes over time has not yet been established, according to the World Federation of Haemophilia (15), and, to our knowledge, no longitudinal follow-ups have been published.
The aim of this study was to describe self-reported activity using the HAL questionnaire for Swedish adult PWH with the moderate and severe form of haemophilia. A second aim was to detect any changes in activity over time, with approximatively 2.5 years between assessments.
The HAL questionnaire has 42 items with 6 possible response options: “impossible”, “always”, “mostly”, “sometimes, “rarely”, and “never”. The questions that are asked in HAL are: “In the previous month, did you have any difficulty, due to hemophilia, with: …?”. “Not applicable” is a possible answer for some questions (13). HAL was developed in the Netherlands and is available in several languages. The Swedish version has been validity tested (16). The HAL has a normalized scoring system, from 0 to 100, where 0 is bad and 100 is good. “Not applicable” is a not a valid answer in the algorithm used to normalize the score. The result is divided into 7 domains (17) (Fig. 1).
Fig. 1. Haemophilia Activity List (HAL). Items and domains. The overall question is: “In the previous month, did you have any difficulty due to haemophilia with:….?”
PWH, recruited from the 3 haemophilia treatment centres in Sweden (Stockholm, Malmö, Gothenburg), were invited by post to participate in the study. Inclusion criteria were: age ≥ 18 years, having haemophilia A or B, severe or moderate form (18); ability to read and understand Swedish. The survey was sent to the available population (n = 260) in Sweden meeting the inclusion criteria. In the invitation letter all participants were asked to sign informed consent and return this along with completed questionnaires. In addition to the HAL, a background questionnaire was sent and contained demographic data (Tables I and II). Data from a previous study conducted 2.5 years earlier was also used, and 61 of the PWH had answered the HAL both times (16). In this study the participants also gave their informed consent. For these 61 PWH, information about self-reported bleeding episodes in muscles or joints was gathered during the 2.5-year period. PWH who did not respond after the first invitation letter were sent a reminder letter after 4–6 weeks.
The study was approved by the Central Ethical Review Board of Gothenburg.
Table I. Background data for the participants in the study groups, later treatment onset (LT) and early treatment onset (ET)
Table II. Reported prophylactic treatment regime for the 129 persons with haemophilia (PWH) in the study, divided into type and form of haemophilia diagnosis
Descriptive statistics are given in terms of count and percentages for categorical variables, and means with standard deviation (SD) for continuous variables. Median and min–max scores are given for description of HAL domains. Differences in HAL domains according to when it was possible to have treatment with the clotting factor in Sweden, termed here the later treatment onset (LT) group and early treatment onset (ET) group, respectively (8), as in a previous study (19) were tested using the Mann–Whitney U test. The dividing point was set as participants who were 45 years old or younger at the time of the study in the ET group, most of whom would have been born in or after 1965. The LT group was born before 1965. If the participants answered HAL twice (n = 61) they were included in the same group as in the first survey.
Changes over time were analysed for each item by pairing off the assessments of each item for HAL at the first time-point (HAL T I) and at the second time-point (HAL T II). Frequency distributions of the pairs of data were described in contingency tables, and the row and column frequencies were shown in the marginal distributions. The percentage agreement (PA) of identical pairs was calculated.
Differences were evaluated by a statistical method that identifies and measures the group-related systematic disagreement separately from the additional individual variability. A non-zero measure of relative position (RP) expresses a systematic shift in the use of scale categories between the 2 assessments, and, correspondingly, a systematic change in how the assessments are concentrated on the scale is expressed by the relative concentration (RC). Possible values of RP and RC range between −1 and 1; a zero value indicates lack of systematic disagreement. The rank-transformable pattern of agreement (RTPA) was constructed by pairing off the marginal distributions, and it describes the expected paired distribution in case of systematic disagreement only. Deviation from the RTPA is a sign of additional individual disagreement, measured by the relative rank variance (RV), ranging from 0 to 1, and a non-zero value indicates heterogeneous groups of data (20, 21). The 95% confidence intervals (95% CIs) of RP, RC and RV were calculated using free software (22). IBM SPSS 19.0 (SPSS Inc. Chicago, IL, USA) was used for data analysis.
A total of 129 (50%) PWH, mean age 43 years (standard deviation (SD) 17.6 years) participated, and 28 (11%), mean age 44 (SD 15.9) years actively declined to participate. There were 103 non-responders (40%). The whole group of drop-outs (n = 131) had a mean age of 37 (SD 14.9) years and 80% had haemophilia A and 20% haemophilia B. Sixty-nine percent had the severe form and 31% had the moderate form of haemophilia. Sixty-one PWH had answered HAL twice.
The reported background data for the study groups (n = 129) are shown in Table I, divided into the ET (n = 76) and LT (n = 53) groups. In the LT group 75% had treatment with the clotting factor as prophylaxis and 25% did not. The most commonly used interval for prophylactic treatment was twice a week (40%), the remaining participants were treated 3 times a week (30%), every second day or other (30%). In the ET group 83% had prophylaxis and 17% did not. The most common interval was 3 times a week (35%) and thereafter every second day (30%), then twice a week (19%) and other (16%). In Table II the different prophylactic treatment regimes for the PWH are shown divided into haemophilia diagnoses and severity for the ET and LT groups. In the LT group, only 7 of 52 subjects had had prophylaxis since childhood and 8 of 48 subjects currently had, or had previously had, inhibitors of the clotting factor. For the ET group the corresponding figures are 47 of 73 subjects for prophylaxis, and 12 of 70 subjects currently or previously had inhibitors of the clotting factor.
The most common comorbidities were: hypertension (56%), liver disease (40%), back pain (17%) and other diseases (30%) for the LT group. For the ET group the comorbidity frequency was lower, with hypertension (11%), liver disease (13%), back pain (8%) and other diseases (14%). Hepatitis and human immunodeficiency virus (HIV) were mentioned within the subgroup “other diseases”. A history of orthopaedic surgery in joints is more common in the LT group compared with the ET group. Of the LT group 63% (n = 32) had undergone orthopaedic surgery with joint replacement in a lower extremity, either in the knee, ankle or hip, and 14% (n = 6) had had joint replacement in an upper extremity, either in the elbow/s or in the shoulder/s. Corresponding figures for the ET group were 16% (n = 12) for joint replacement in the lower extremities and 5% (n = 3) in the upper extremities, in this group only in the elbows.
There was a significant difference between the ET (n = 53) and LT groups (n = 76) (p < 0.001) in all domains of the HAL assessment, where the ET group had better outcomes than the LT group in all domains (Table III). For the ET group the median score was 100 in all domains, except for complex lower extremities, indicating that 50% of the group had almost no difficulties. However, the range of perceived limitations in all domains was large, indicating that some individual differences existed. More than 50% of the ET group had the best score (100) in almost every domain of HAL. The self-reported bleeds between the 2 time-points are shown in Fig. 2. In the ET group, 19 of 26 PWH reported ≤ 3 bleeds (73%) and the corresponding number for the LT group was 21 of 31 PWH (68%). Five PWH reported more than 10 bleeds, 1 from the ET group and 4 from the LT group. None of these PWH had ever had inhibitors of the clotting factor and 4 of them had prophylactic treatment.
Table III. Results of the Haemophilia Activity List (HAL) domains normalized score (0 = worst functional status and 100 = best possible functional status). n = numbers of PWH that have answered the questions in each domain divided into 2 groups: later treatment (LT) and early treatment (ET)
Fig. 2. Reported joint and muscles bleedings between the first and second time-point (2.5 years). Early treatment onset (ET) group, n = 26, 3 missing data; and later treatment onset (LT) group, n = 31, 1 missing data.
In Table IV the changes in HAL score for the 61 subjects who had answered the HAL questionnaire twice, for both the ET and LT groups of PWH are shown. The reported ability differed between the ET and LT groups overall at baseline. Most commonly, there were almost no reported experienced difficulties amongst those in the ET group, in the activities investigated. In contrast, the LT group reported greater limitations in their abilities, in the activities investigated, at baseline. There were no significant changes for the ET group in 37 activities of the 42 investigated and in 29 for the LT group (Table IV). Seven activities had a significant change at the individual level, especially in the LT group, and at the group level there were significant changes in 4 activities for both groups (Table IV). Change in ability over time was most prominent for the LT group in the last domain of HAL, “leisure activities and sport”(items 36–42). There were significant changes at the group level (RP) regarding the reported increased disability in question 36, “playing games”, number 37, “sports”, and number 41, “going on an active holiday”. The pattern was the same, with significantly worse reported ability at the second time-point, at the group level for the LT group. The answer “not applicable” had been used in approximately one-third of the answers in these questions at the second time-point, and the answer “impossible” was also frequently used in the LT group. At the individual level, there was a significant change in the Relative Rank Invariant (RV) for the LT group, showing a heterogeneous result in question 40, “dancing”, number 41, “going on an active holiday”, and number 42, “going on a passive holiday” (see Fig. 3a, b and Fig. 4). For the ET group there were no significant changes in this domain.
Table IV. In the previous month did you have any difficulty due to haemophilia with: item by item for the Haemophilia Activity List (HAL) divided into early and later treatment onset groups over 2.5 years
Table IV cont.
Fig. 3. (a and b) Illustration of the ability for the early (ET) and later (LT) treatment onset groups in the domain “leisure and sport”. n/a: not applicable. Haemophilia Activity List (HAL) T_I: first time-point in HAL; HAL T_II: second time-point in HAL 2.5 years later. ET n = 29 and LT n = 32.
Fig. 4. Paired distribution for the LT group for the HAL question no 36 playing games (%). n/a = not applicable. The vertical scale steps are HAL I, the first time point (HAL T I) and the horizontal scale steps are HAL II the second time point (HAL T II). Light grey are reported better and middle grey are reported worse and dark grey are reported stable over 2.5 years’ time
In the domain “lying/sitting/kneeling/standing”(items 1–8), the ET group showed a significant change, and reported their ability as being better in question 1, “sitting down”, at the group level, relative position (RP). Ninety percent (90%) had answered; “never” had difficulty with sitting down due to haemophilia at the second time-point. The same pattern was seen for this group in question 4, “kneeling/squatting”. The LT group reported at the group level (RP) their ability as being better in question 3, “rising from a chair without armrests”. In the LT group they reported significant changes in question 5, “bending forward”, at the individual level (RV). The answer “never” had difficulty with the activity in this domain was unchanged between 55% and 82% of the ET group. Corresponding figures for the LT group were 6–41% of the different activities.
In the domain, “function of the legs” (item 9–17) there were significant changes in 2 questions in the ET group; at group level in RP in number 9, being better to “walk short distances”, and in RC, number 13, “strolling”. In strolling their reported ability concentrates in the 3 categories “sometimes”, “rarely” and “never” had difficulty at the second time-point. “Never” had 69% of the answers at the second time-point. In the LT group there were significant changes at the individual level (RV) in question 9 “walking short distances”. In question 14, “climbing up the stairs”, the LT group had significant changes at the individual level (RV).
In the domain, “use of transportation” (items 22–24) there was a significant improvement in question 23 “get in and out of a car” in the ET group at the group level (RP). In the LT group there was a significant change at the individual level (RV) in question 24, to “use public transportation”.
In the domain, “self-care” (items 25–29), there were 2 questions; number 25, “drying your whole body” and 27, “putting on sock and shoes”, with significant changes in the RC for the LT group. The scale step “rarely” was reported more at the second time-point for both questions, indicating that the LT group had increased this answer both from a better and a worse self-reported answer. No other significant differences were seen in this domain. The ET group, to a great extent, reported “never” in the activities in this domain.
In the domain, “function of the arms” (items 18–21) there were no significant changes in reported activity over time in either group. The ET group reported “never” in this domain to a great extent, and the LT group reported stability in their answers. Their answers were more evenly distributed over the scale, meaning that their ability had not changed over time, but many had difficulties with the activities, especially with the activities lifting and carrying heavy objects (questions 18 and 19).
In the domain, “household tasks” (items 30–35), there was no significant change over time. The patterns in answers were similar to those for the domain “function of the arms”.
This study revealed differences in self-reported activity in HAL for PWH living in Sweden. Being able to access prophylactic treatment with the missing clotting factor for PWH in Sweden leads to a clear difference in self-reported activity levels and abilities.
The most prominent results over time were found in the domain “leisure activities and sport”, where the most prominent differences were seen between the ET and LT groups. The ET group reported no difficulties as a group, but the LT group showed greater limitations in their self-reported ability in some of the activities. This domain is the one that is most dependent on society’s environmental factors, but these are not included in HAL. All we know is that the investigated population lived in Sweden, but not what it is like where they lived or what opportunity they had for participation in the asked about activities.
A Swedish study of HRQoL in adult PWH showed that patients who started prophylactic treatment later in life also had to cope with disability to a greater extent than the PWH who had prophylactic treatment early in life (10). This was also borne out in this study population. The LT group had more difficulties with activities compared with the ET group, and one reason could be haemophilia arthropathy.
In the HAL questionnaire the capacity and the performance quality of the investigated activities are not asked for. The PWH just report if they perform the activity or not and if they have had difficulties due to haemophilia in the last month.
For the domains involving the upper extremities there were 2 domains with no significant changes over time; “function of the arms” and “household tasks”, showing that the PWH had no changes in their function using the upper extremities. The reported abilities for activities using lower extremities showed more difficulties, especially for the LT group, indicating joint disabilities.
A limitation of using HAL is that it is self-reported, an opinion of a PWH, and not an objective measure of difficulty. However, because HAL is often not used in isolation, it allows for the gathering of direct experiences from PWH and does not just use the objective measures that might otherwise provide an indication of activity ability. In combination with the objective measures, HAL provides a more nuanced picture of the ability of PWH to perform activities.
A study evaluating 2 medical models for PWH showed a nearly maximum medium score (99 of 100) in HAL for a young Swedish PWH population born in 1970–1994 (23), and our study also showed a ceiling effect in the early treatment onset group using HAL. Many PWH in the ET group reported the best value of “never had difficulties” due to haemophilia in the asked about activities. This could be because prophylactic treatment is also commonly used in the adult haemophilia population in Sweden (6) and not only in children, as may be the case in other parts of the world.
Approximately 80% of PWH in both groups that answered the HAL questionnaire also stated that they had some regular form of prophylactic treatment. However, some of these PWH reported many bleeds during the period between the 2 time-points. Some of the PWH have, or have had, inhibitors of the clotting factor, and can therefore not have ordinary prophylactic treatment. This presents a risk for more bleeds. In this survey, only 3 PWH of those who reported “no prophylactic treatment” also reported “had or had had inhibitors”. Therefore, the reported high bleed rate could be caused by PWH not initially being able to recognize the difference between pain and swelling due to arthropathy and pain and swelling due to bleeding.
The LT group reported more bleeds and greater difficulties than the ET group. However, it is worth considering that, due to their older age, there are some difficulties that arise from the normal ageing process. These difficulties from ageing can be easily confused for symptoms from haemophilia, which can make it difficult to determine what is the primary cause of these particular difficulties.
In recent years the ageing comorbidities for the adult population of PWH have been highlighted, and rehabilitation and physical activity have been mentioned as important, and even necessary, due to arthropathy and pain (24, 25). Pre-existing geriatric comorbidities, such as hip arthrosis, together with haemophilia arthropathy, might have influenced the results of this study, especially with regards to self-care and walking distance.
Orthopaedic surgeries were more common in the LT group compared with the ET group. This is consistent with a study evaluating treatment comparing Dutch and Swedish PWH born in 1970–1994, in which 8% of the Swedish PWH had undergone orthopaedic surgery (23).
HAL has been suggested for use in identifying problem areas (24). To the best of our knowledge this is the first published longitudinal investigation using HAL. In healthcare it is essential to show consideration for the patients’ own perception of their health, and therefore it is important to know how commonly used questionnaires function and how sensitive they are over time to evaluate the result of an intervention or ongoing medical treatment, such as during the annual check-up at Haemophilia Treatment Centers (HTC). Since the data is ordinal, a feasible statistical method has been used. Of the 42 questions, many deal with joint-related limitations from lower extremities, and it could be possible to reduce the number of questions and still capture the difficulties from the lower extremities. Worldwide, HTCs use many kinds of instruments classified in the ICF as impairment and activity assessments, such as the Haemophilia Joint Health Scores (HJHS) to evaluate joint status and global gait (walking, running, climbing stairs and jumping on one leg) (26), assessing performance in activities of daily living (ADL) using the Functional Independent Scale of Haemophilia (FISH) (27) and different questionnaires measuring HRQoL (28). Also, national registries are more and more commonly used to evaluate medical treatment, and require patient input and views around activity and participation as well as QoL to be considered when evaluating treatment options. HAL could be a great complement to the QoL questionnaires and the joint status, HJHS, when evaluating PWH at their annual check-up and in research.
The study has mostly self-reported information, which might be a limitation; the reported bleed rate and background data has not been validated through checking medical records. In addition, the bleeding rate among persons with haemophilia arthropathy could be overestimated because of the difficulty of differentiating between pain due to haemophilia arthropathy and an acute bleed.
When comparing the results of HAL, the population were divided into 2 groups, ET and LT, according to approximate access to clotting factors (8). Of course, the dividing line has been decided by the authors as an approximation and some of the participants could be borderline. This could be one of the reasons that the ranges in almost every domain of HAL, and individual questions within it are wide. Another reason could be the presence of inhibitors against clotting factor in some individuals. Even in the ET group there are persons who reported histories of inhibitors, which can explain some of this group’s limited ability. One could speculate that if the persons with or with a history of inhibitors were excluded the results may have been more consistent.
Another limitation is the number of participating persons with haemophilia (PWH). We do not know anything about the ability of the more than 50% of the Swedish adult PWH who did not answer the HAL questionnaire at the time of the survey. Haemophilia is a rare bleeding disorder and it is difficult to find a study population large enough, especially when the context where the subjects live is important for the research questions.
In conclusion, the ET group reported a significantly better ability overall compared with the LT group in activities investigated using HAL. The most prominent changes over time were seen in the domain “leisure activities and sport”, where the LT group’s ability had changed to being worse in some of the activities. This could be a result of difficulties to do with ageing in combination with haemophilia arthropathy. The HAL questionnaire had a ceiling effect for the ET group of adult PWH living in Sweden. Except for a few activities investigated, there were no significant changes over time assessed with HAL for the ET group.
This study received unrestricted grants from the Local Research and Development Board for Gothenburg and Södra Bohuslän, the Region Västra Götaland, Renee’ Eander’s Foundation for Research, Felix Neubergh Foundation for Research, Hjalmar Svensson’s Foundation for Research, Greta and Einar Asker’s Foundation and the Arosenius Foundation. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. The authors would like to thank Dr Kate Bramley-Moore for English language proofreading assistance.
The authors have no conflicts of interests to declare.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize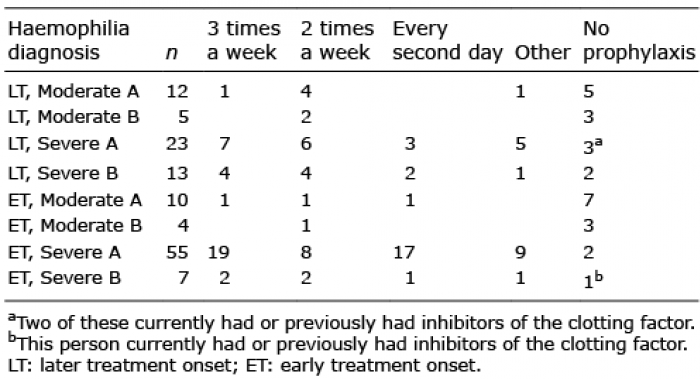 Click to show fullsize
Click to show fullsize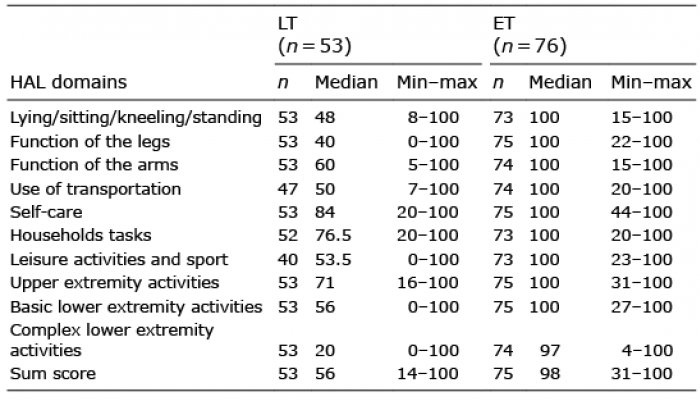 Click to show fullsize
Click to show fullsize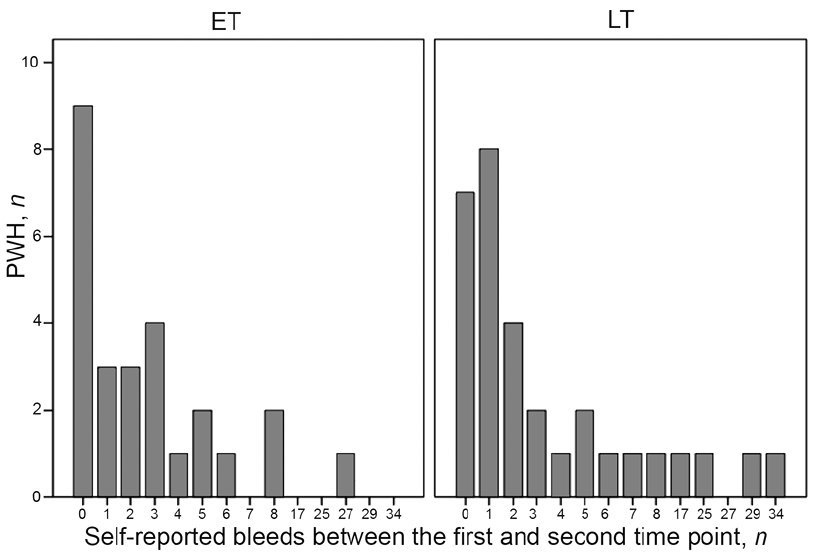 Click to show fullsize
Click to show fullsize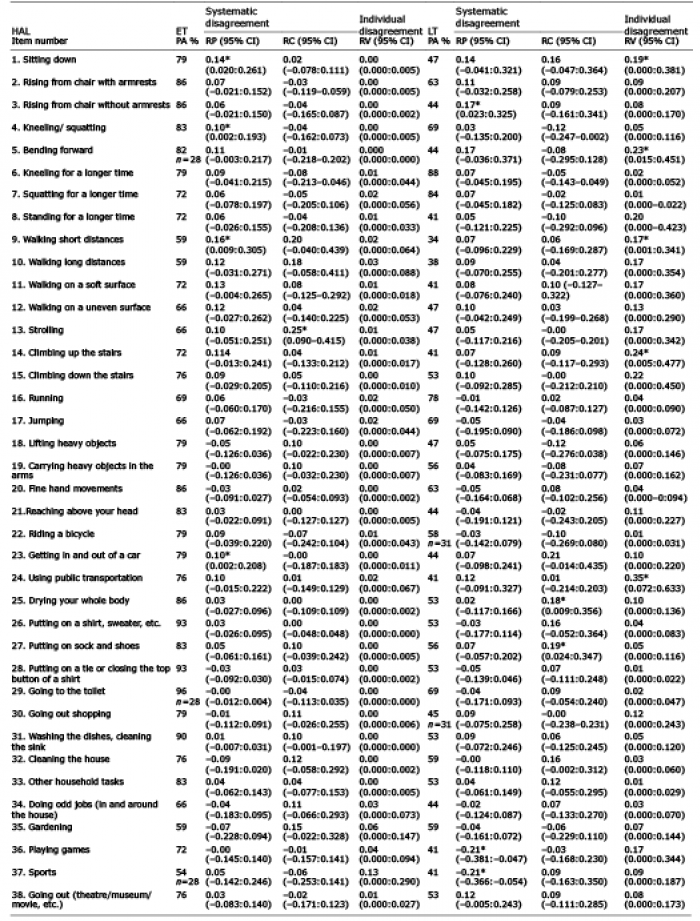 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize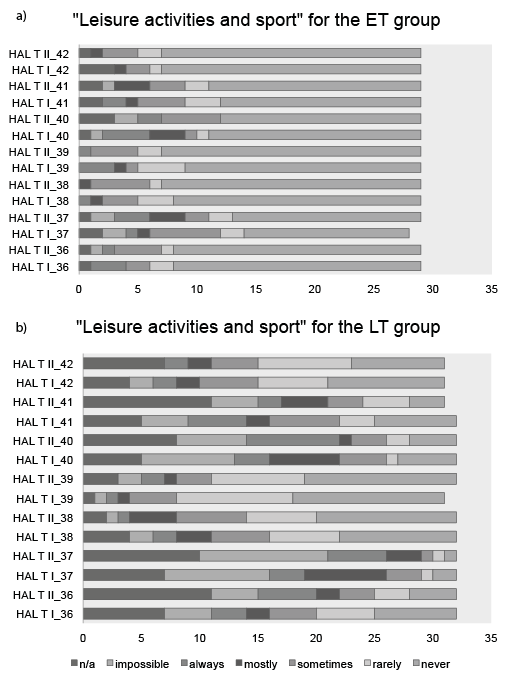 Click to show fullsize
Click to show fullsize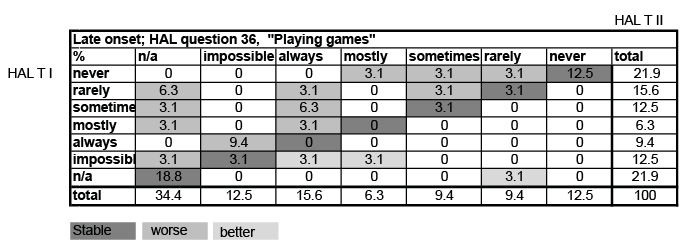 Click to show fullsize
Click to show fullsize