
From the 1Department of Rehabilitation Medicine, Yue Bei People’s Hospital, ShaoGuan, 2Department of Hyperbaric Oxygen, Sun Yat-Sen Memorial Hospital, Sun Yat-Sen University, GuangZhou, China, and 3Department of Physical Therapy, University of North Texas Health Science Center, Fort Worth, TX, USA
#These authors contributed equally and should be considered as first authors.
Objective: To study the effect of therapeutic exercise on knee osteoarthritis after injection of botulinum toxin type A, hyaluronate or saline.
Methods: Sixty participants with knee osteoarthritis were randomly assigned to 3 groups: injection of saline (control) (group A), botulinum toxin type A (group B), or hyaluronate (group C). All participants received therapeutic exercise. Western Ontario and McMaster Universities Osteoarthritis Index questionnaire score, visual analogue scale pain scale, and Medical Outcomes Study 36-item Health Survey were conducted at baseline, and at the end of the 4th and 8th weeks.
Results: At end of the 4th and 8th weeks, the scores on the Western Ontario and McMaster Universities Osteoarthritis Index questionnaire and visual analogue scale were higher in the control group. There were significant differences in Physical Component Summary-36 and Mental Component Summary-36 scores between the 3 groups (p < 0.05) at the end of the 4th and 8th weeks, but not between groups A (control) and C (hyaluronate) at the end of the 4th week. No changes were seen on magnetic resonance imaging and X-ray images of the affected knees after the intervention.
Conclusion: Therapeutic exercise plus botulinum toxin type A or hyaluronate injection can significantly reduce pain and improve knee functioning. Botulinum toxin type A plus therapeutic exercise appears to be more effective.
Key word: botulinum toxin type A; hyaluronate; knee osteoarthritis; therapeutic exercise; dysfunction.
Accepted Mar 7, 2018; Epub ahead of print Apr 17, 2018
J Rehabil Med 2018; 50: 00–00
Correspondence addresses: Howe Liu, Department of Physical Therapy, University of North Texas Health Science Center, 3500 Camp Bowie Blvd, Fort Worth, TX, USA. E-mail: Howe.Liu@unthsc.edu; Hui-Yu Liu, Department of Rehabilitation Medicine, Yue Bei People’s Hospital, No. 133 HuiMin Road, 512025 ShaoGuan, China. E-mail: liuhuiyudoctor@sohu.com
Patients with knee osteoarthritis often have pain and joint dysfunction, which are not easy to treat using conventional therapy. The effect of a new therapy for relieving pain in patients with knee osteoarthritis was studied. This therapy involves ultrasound-guided injection of botulinum toxin type A, followed by therapeutic exercise. We compared this treatment with conventional therapy using injection with hyaluronate (a component of the synovial fluid), and a control treatment using saline injection, followed by the same exercises. The results showed that injection of botulinum toxin type A followed by therapeutic exercises resulted in greater improvements in knee pain and function in patients with knee osteoarthritis. Combined treatment with botulinum toxin type A, followed by therapeutic exercise is therefore recommended for people who have knee pain that does not respond well to conventional therapy.
Knee osteoarthritis (OA) is a chronic and progressive disease that is the most common joint disorder in China. Knee OA is characterized by articular cartilage degeneration, bony changes and osteophyte formation. It often causes joint pain, swelling and dysfunction, which can affect patients’ quality of life, and may lead to depression (1).
Conservative treatment for knee OA usually includes medication, physical therapy and other alternative medical interventions. Although oral analgesics, such as non-steroidal anti-inflammatory drugs (NSAIDs), can achieve moderate reduction in pain and slight functional improvement, they have substantial limitations. NSAIDs may not provide sufficient relief from joint pain, they often induce gastrointestinal discomfort, and can adversely interact with other drugs (2). Physical therapy and other alternative medical interventions are effective most of time, but the effects are not long-lasting (3, 4). Surgical interventions with arthroscopic lavage and debridement may be offered for refractory joint pain when medical therapies fail, but the benefits of these procedures are debated (5). However, patients are also not always willing to consider joint replacement surgery when symptoms of knee OA persist. Under such conditions, a potential treatment may be to switch to therapeutic exercise plus intra-articular (IA) injection of botulinum toxin type A (BoNT-A) or hyaluronate.
The effect of original BoNT-A is the inhibition of the exocytotic release of acetylcholine from motor nerve terminals, which makes it useful in the treatment of local muscle spasm, such as limb spasm after stroke, facial spasm and spasmodic torticollis (6). Recently, the effects of BoNT-A in pain modulation have been studied. BoNT-A is often reported for use in low-back pain, myofascial pain, and joint pain caused by arthritis. Such treatment has been shown to lead to significant improvements in pain and function and is safe to use (7–12). Some advantages of therapeutic exercise for knee OA are its non-invasive nature, being preferred by both patients and physicians, and that it can strengthen muscles and improve balance in the lower limbs (13). To date, no published studies have prospectively evaluated the efficacy of IA BoNT-A plus therapeutic exercise for treatment of knee OA.
Hyaluronate, a major component of the synovial fluid, acts as a lubricant and shock absorber to help maintain the structural and functional characteristics of the cartilage matrix. Hyaluronate plays many key roles in the trophic status of the cartilage and regulation of the IA environment. It inhibits the formation and release of prostaglandins, induces proteoglycan aggregation and synthesis, and modulates the inflammatory response (14, 15). Previous studies have shown that 3 or 5 weekly injections of hyaluronate (16) or hyaluronate injection plus therapeutic home exercise (17) may reduce pain and improve physical functioning in patients with knee OA.
The current study hypothesized that pain and dysfunction due to knee OA could be alleviated by the combined effect of medicine and therapeutic exercise, without changing the structure of the knee joint. Such therapy could provide a new choice for patients with knee OA. The study therefore evaluated the effects of therapeutic exercise after injection of BoNT-A or hyaluronate using ultrasound-guided methods in patients with knee OA. Structural changes in the knee joints were evaluated by MRI and X-ray before and after the interventions.
This was a prospective, single-blinded randomized controlled trial with an 8-week follow-up period. The protocol was approved by the ethics committee of Yue Bei People’s Hospital (2015CX/K025) and the trial was retrospectively registered with the ISRCTN registry (study IDISRCTN13172678).
The study was conducted in a rehabilitation department of Yue Bei People’s Hospital in Shao-Guan. All patients were recruited via posters. They were divided randomly into 3 groups based on different injections (group A: saline as control; group B: BoNT-A; group C: hyaluronate) and received therapeutic exercises after injection. Randomization was conducted using a computerized sample of convenience after a subject was screened, recruited, and signed an informed consent statement. Assessments were conducted at baseline, and at the end of the 4th and 8th weeks by a physiotherapist blinded to the subjects’ interventions.
From an initial total of 86 patients with knee OA visiting the acute comprehensive hospital in China, 60 patients fulfilled the selection criteria (below) from January to December 2016 and were admitted to the study. The subjects’ age range was 59–72 years (mean age 65.9 (standard deviation (SD) 3.19) years). Inclusion criteria were: (i) mentally intact, i.e. able to follow 2-step commands; (ii) radiographic OA severity grade 2 or above for the knee joint on the Kellgren-Lawrence scale (18) and pain visual analogue scale score ≥ 6 after walking a distance of 100 m continuously on level ground; (iii) failure of physical therapy and/or medical treatment in the last 3 months; (iv) involvement of unilateral knee joint through clinical check and bilateral X-ray of the knees. Exclusion criteria were: (i) patients who had received an IA injection in the affected knee within 3 months prior to the initial evaluation; (ii) disease complications, such as rheumatoid arthritis, tumours and any non-arthritic trauma to the affected knee, in the last 3 months; (iii) severe cardiac, liver or kidney dysfunction that had caused hospitalization in the last 3 months. All patients provided written informed consent.
All patients received injections and therapeutic exercise as outpatients. The procedure for group B was 100 U BoNT-A (Botox; Allergan Inc., Irvine, KY, USA) diluted with 2.5 ml preservative-free 0.9% saline solution. A single injection was given by an experienced rehabilitation physician with the patients in the supine position. Colour Doppler ultrasound (GE, Fairfield, CT, USA) was used to identify the articular cavity of the knee at the level of the suprapatellar bursa using sterile ultrasound gel and a lateral approach. A linear array musculoskeletal ultrasound probe and a frequency of 5 MHz were used. The patient’s knee joint was fixed in the straight position. The injection site was sterilized using iodophor. A 22-gauge needle was inserted directly into the articular cavity at the above-mentioned location under ultrasound guidance using an in-plane approach. Groups A and C were given injections of saline (2.5 ml) or sodium hyaluronate (ARTZ, Seikagaku Corporation Takahagi Plant, Ibaraki, Japan), respectively, using the same injection method as group B. Group C received a hyaluronate injection once a week for 5 weeks. For patients with a lot of effusion in the knee articular cavity, the effusion was aspirated via a needle before giving the treatment injection.
Ice bags were used to relieve transient pain or swelling after the injection in some patients. If the patients could endure transient pain, they began therapeutic training following the injection. The training was conducted in an activity room at the outpatient clinic, which had parallel bars and a well-lighted, carpeted hallway with handrails on the wall for participants to hold as needed during walking. Strengthening and balance exercises were taught to all subjects, to perform 30–45-min per session, 5 times a week for 8 weeks. Patients were provided with instructions and exercises were demonstrated. During these 8 weeks, the subjects received instruction and consultations on therapeutic exercises from a licensed physical therapist who was blinded to the subject grouping in the study. All patients received group exercises. In accordance with the individual’s functional level, the resistance of the strength exercises was increased gradually, and balance exercises were initially performed within the parallel bars to increase stability and prevent falls during training. Walking was included to address dynamic balance and endurance (walking distance). During the entire exercise session, each subject in all groups received the same exercise protocol; however, the resistance for strengthening was individualized according to each person’s functional level and tolerance. Progression occurred when the subject was able to perform an exercise for 2 sets of 10 without pain on 5 consecutive days. The initial amount of resistance (poundage) was determined when a person was able to perform 1 set of 5–10 of each exercise with minimal resistance (from 0 to 1 kg in this study) without exacerbation of symptoms (worsening of pain, shortness of breath, pale face, dizziness). The maximum weight for resistance exercise was 3 kg on each knee or 5 kg on the waist (see Table SI1).
If the results from groups B or C coincided with our speculation that BoNT-A was more effective than hyauronate for releasing knee pain, BoNT-A injection would be given to the subjects in group A in order to relieve knee pain and functioning.
Baseline information included age, sex, and time of onset. Data from the Western Ontario and McMaster Universities Osteoarthritis Index questionnaire score (WOMAC), visual analogue scale (VAS) pain scale, and the Medical Outcomes Study 36-item Health Survey (SF-36) were collected at 3 time-points (baseline, and at the end of the 4th and 8th weeks). The WOMAC is a commonly-used measure of knee joint dysfunction, which includes 24 questions (5 questions associated with pain, 2 with joint stiffness and 17 with knee joint function). The lower the score, the better the knee joint function (4). Reliability for the pain, stiffness and physical function subscales was 0.68, 0.48 and 0.68, respectively (19).
Pain was measured by means of a VAS, with 0 indicating no pain and 10 indicating unbearable pain. The VAS is a valid and reliable measure for pain, and changes of 2 or more were considered clinically relevant (20). Reliability for the VAS was 0.97 (21).
SF-36 was measured in 8 different domains of patients’ health: physical functioning (PF), role-physical (RP), bodily pain (BP), general health (GH), vitality (VT), social functioning (SF), role-emotional (RE) and mental health (MH). In addition, the Physical Component Summary (PCS) encompasses PF, RP, and BP, whereas the Mental Component Summary (MCS) includes SF, RE, and MH. Scores range from 0 to 100, with 0 corresponding to low health-related quality of life (HRQL) and 100 corresponding to high HRQL (22). Scores were recorded from each domain in order to assess a subject’s quality of life. Reliability for the SF-36 was 0.87 (23). Medical imaging of the knee joint was examined by X-ray and MRI to evaluate the structure of the knee joint at baseline, and at the end of the 4th and 8th weeks.
The data were analysed using SPSS for Windows version 20. Continuous data were expressed as means and standard deviations. The comparison of baseline with each follow-up point (weeks 4 and 8) within each group was performed by one-way analysis of variance (ANOVA) for continuous data and McNemar’s test for discrete data. Comparisons between groups at each follow-up point were conducted using repeated measures analysis of variance for continuous data and χ2 tests for discrete data. The significance level was set at p < 0.05.
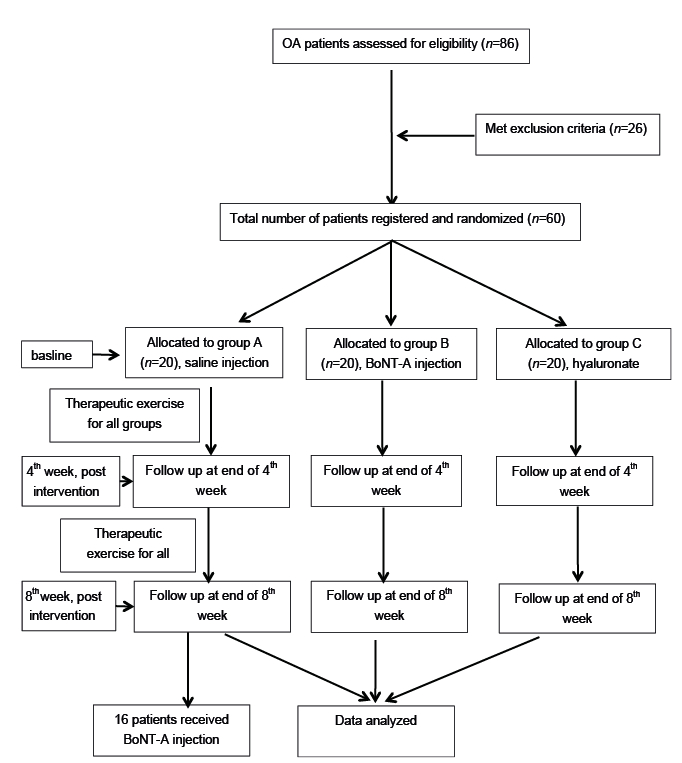
Fig. 1 shows the flow diagram of eligible patients in the study. A total of 86 participants were admitted to the study at the beginning and 26 patients were excluded for several reasons (details shown in Fig. 1). Of these, 60 patients met the inclusion criteria and consented to receive intervention and follow-up assessment. A final total of 60 patients (26 males and 34 females) completed the study without dropout.
Fig. 1. Flow diagram of patients in the trial.
Time since onset ranged from 18 to 48 months (mean 31.9 months SD 8.18). There was no drop-out during the whole 8-week follow-up. There was no significant difference among groups in terms of sex, age or onset time. Demographic data for the recruited patients are shown in Table I.
Table I. Clinical data
The comparisons within groups for WOMAC, VAS and SF-36 are shown in Table II. Both WOMAC and VAS scores decreased within group B and group C, but not in group A at the end of the 4th and 8th weeks. There were significant differences between the 4th and 8th weeks in group B in WOMAC and VAS scores (p < 0.05), but not in group A and group C (p > 0.05). PCS-36 and MCS-36 were improved in group B and group C patients at the end of the 4th or 8th week compared with baseline (p < 0.05), but not in group A (p >0.05). There were significant differences between the 4th and 8th weeks in group B and group C in PCS-36 and MCS-36 (p < 0.05), but not in group A (p >0.05).
Table II. Comparison of WOMAC, VAS and SF-36 within groups at 4 and 8 weeks
The comparisons of all measurements between the 3 groups are shown in Table III. There were significant differences in WOMAC and VAS between group A and group B, group B and group C (p < 0.05), but not between group A and group C (p >0.05) in the end of the 4th week. The comparison between group A, group B and group C revealed differences on VAS and WOMAC at the end of the 8th week, respectively (p < 0.05). There were significant differences in PCS-36 and MCS-36 between group A and group B, group A and group C, group B and C (p < 0.05) at the end of the 4th and 8th weeks, but not between group A and group C in MCS-36 at the end of the 4th week.
Table III. Comparison of the WOMAC, VAS and SF-36 between groups at 4 and 8 weeks
The major purpose of the MRI and X-ray examinations was to evaluate the structure of the knee joint and understand whether the improvement in knee function and pain is related to the structure of the knee joint. There were no changes after intervention on the MRI and X-ray images of the affected knee according to the Kellgren-Lawrence (KL) scale at the end of the 4th and 8th weeks (p > 0.05).
No adverse events, such as death, new lower limb motor or sensory dysfunction, anaphylactic reaction to the injection, or inflammation of injection site, occurred during the study. No transient muscle weakness was found in any of the groups.
This prospective study in patients with knee OA revealed that therapeutic exercise after IA injection of BoNT-A or hyaluronate resulted in improvements in pain and knee functioning.
A novel use of a well-known drug (BoNT-A) was compared with a treatment that is the current standard of care (IA hyaluronate) and placebo for patients with knee OA. Significant improvement was demonstrated in VAS, WOMAC and SF-36 in groups B and C. The VAS score in group B decreased significantly by the end of the 4th and 8th weeks. PCS-36 and MCS-36 scores showed significant improvement at the end of the 4th and 8th weeks between groups, but not between group A and group C at the end of the 4th week. This may be due to psychological factors in participants, since the SF-36 assessment involved the patients’ subjective feelings.
We speculate that both BoNT-A and hyaluronate injection improved knee function and relieved pain for following reasons: (i) the treatment reduced knee pain and consequently increased patient compliance with knee joint exercises after injection; (ii) the less pain, the greater the patient’s confidence, and this created positive feedback.
Group B may have had better results than group C due to a different mechanism of medicine effect. The mechanism of BoNT-A-induced pain reduction for knee OA is unclear. It has been reported in the rat model (24) that joint damage or inflammation caused by OA could result in the production of various substances, such as bradykinin, serotonin, K+, H+, histamine, and prostaglandins. These substances could act on nociceptors of the free nerve endings, and then activate the polymodal C-and A- delta fibres in the knee articular tissue (24). It was further found that the afferent signals from these pain fibres could be sensitive to peripheral noxious or non-noxious stimuli (peripheral sensitization) and then be transmitted to the spinal cord to stimulate the dorsal root ganglion neurones for release of nociceptive peptides, such as substance P, calcitonin gene-related peptide (CGRP), and glutamate (central sensitization) (25). It is likely that such sensitizations from damage or inflammation of knee joint increased pain, which was difficult to control with conventional therapy (26, 27). Lately, it was found that BoNT-A was able to block peripheral and central sensitizations by inhibiting releasing neurotransmitters from primary sensory neurones in a rat formalin model, which was produced by injecting formalin into rat paw (28) and reducing c-Fos expression in the dorsal horn of the spinal cord (28, 29). Increased c-Fos expression may indicate increased neuronal activation through harmful stimuli. In addition, data from other investigations showed that BoNT-A might have an anti-nociceptive effect by down-regulating the voltage-gated Na+-channel expression on the rat trigeminal neuralgia (30), or by reducing the peripheral release of neurotransmitters (substance P, CGRP) and pro-inflammatory cytokine IL-1β in rat temporomandibular arthritis (31). Based on this information, a possible explanation of pain-inhibition by BoNT-A is that it reduces the release of neurotransmitters, such as substance P and others, thus blocking the pain signal pathway. Hyaluronate, which is a lubricant, may exert its effect by reducing bone friction and protecting cartilage tissues (32).
In previous studies, triamcinolone or saline have often been used as controls (33). However, in our study, we chose saline as the control injection, because a previous study reported that IA injection of triamcinolone in the knee could result in significant loss of cartilage volume and no significant pain reduction in the knee after 2 years (33).
Furthermore, for the BoNT-A dosage, we chose 100 U BoNT-A on the basis of published studies of IA BoNT-A, showing that a high-dose BoNT-A group did not show any increase in curative effects in comparison with a standard dose of BoNT-A (34). No adverse effects were found in any of the patient groups. These results confirm that the dose of 100 U BoNT-A was safe, similar to the results of a recent study using the same dosage (35).
IA injections are performed using various methods. Some researchers use landmark guidance or surface electromyography (36, 37); however, these techniques are not accurate because the needle tip can easily hit the bone spur or fat pad, and the vessels and nerve can be hit by the needle.
Tresley & Jose (38) found that it is easy to perform sonographically guided IA injections of the knee joint with 100% accuracy and no complications in a consecutive series of 67 patients with OA of the knee. This is a safe, economical, and well-tolerated form of treatment compared with other methods. This method can help physicians to visualize the direction and depth of injection, and thus avoid possible injury to surrounding structures.
Muscle strength, balance, and functional mobility are important components of performance in standing, walking and many activities of daily living. Patients with knee OA could benefit from exercises to increase the muscle strength of the knee joint and improve balance in the lower limbs. Pain associated with knee OA often results in reduced activity and weakening of the muscles, resulting in a secondary increase in knee instability.
The current study showed that therapeutic exercises after injection of BoNT-A or hyaluronate were associated with improvements in pain, disability and activities of daily living, similar to the results of a previous report (39). Interestingly, group B improved more in terms of pain, dysfunction and activities of daily living than did the other groups, especially by the end of 8 weeks. However, there were significant improvements in WOMAC and VAS in group C compared with the controls up to the end of the 8th week. This may be due to the effect of BoNT-A on inhibiting the release of pain neurotransmitters, which was the key factor in inducing pain.
Although previous research has shown that BoNT-A and hyaluronate injection could improve knee function and relieve pain, there are differences between previous studies and our research. First, we used injection of BoNT-A or hyaluronate plus 8-week progressive therapeutic exercises to treat patients with knee OA. Secondly, we accurately injected the medicines into the knee articular cavity in all subjects using ultrasound guidance, which minimized potential injury to the knee by avoiding the risk of the needle tip touching a bone spur or infra-patellar fat pad. Thirdly, we examined the MRI and X-ray images of the knees and found bony spur and meniscus injury still existed after injection, and there were no changes between baseline and after intervention, which could be possible evidence for the effect of BoNT-A in inhibiting the release of neurotransmitter rather than changing the structure of the knee joint or repairing the meniscus.
Although these results are encouraging, some study limitations should be noted. First, we did not test the change in neurotransmitter in the affected knee joint at each assessment point. Thus, we cannot confirm a possible correlation between the effect of BoNT-A and the change in neurotransmitter. Secondly, we only evaluated the outcomes of the 4th and 8th weeks after intervention, but we did not perform a longer follow up. Thus, the study did not evaluate the effective length of each intervention after the 8th week. Thirdly, hyaluronate was given as a series of 5 injections, but BoNT-A and saline were each given as a single injection. These different dose and injection frequencies may influence the results of the study.
Therapeutic exercises for patients with knee OA following injection of BoNT-A or hyaluronate can reduce pain and improve recovery of function in such patients, but BoNT-A combined with therapeutic exercises seems to be the more effective of these treatment, and may provide clinicians with a new option for treatment of patients with knee OA.
The authors would like to thank all the professors and co-workers for their tireless assistance in this project. The authors also thank the individuals who participated in this study and all the administrative support staff.
The work presented here is funded by the Yue Bei People’s Hospital, Shaoguan, China.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize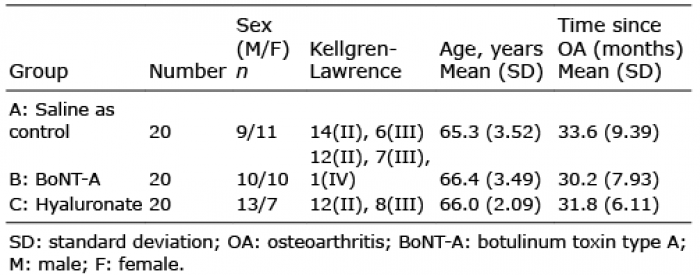 Click to show fullsize
Click to show fullsize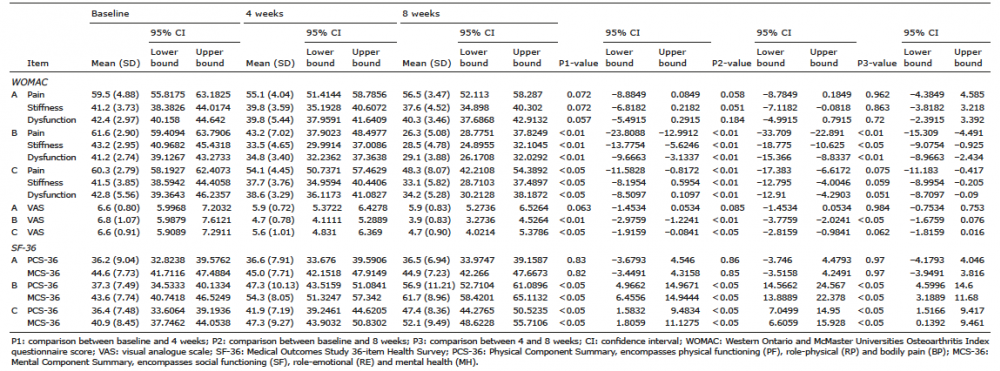 Click to show fullsize
Click to show fullsize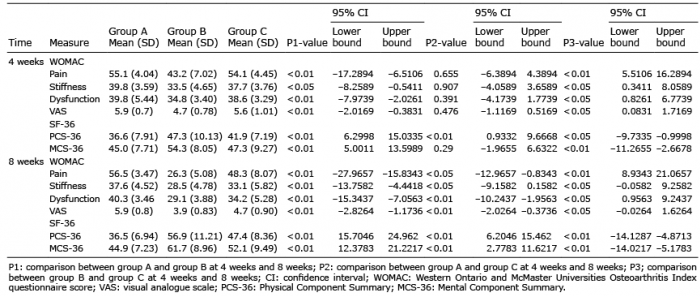 Click to show fullsize
Click to show fullsize