
From the Department of Orthopedics, Traditional Chinese Medicine Hospital of Shaoyang City, Hunan Province, China
Background: Balance training may be beneficial for patients with osteoporosis, although current results are inconclusive. The aim of this systematic review and meta-analysis was to explore the effect of balance training on falls in patients with osteoporosis.
Methods: PubMed, Embase, Web of Science, EBSCO, and Cochrane Library databases were systematically searched. Randomized controlled trials (RCTs) assessing the effect of balance training vs usual activities on falls in patients with osteoporosis were included. Two investigators independently searched articles, extracted data, and assessed the quality of included studies. The primary outcome was fall frequency. This meta-analysis was performed using the fixed- or random-effect model when appropriate.
Results: Six RCTs were included in the systematic review and 3 in the meta-analyses. Compared with control groups, a balance training intervention was found to significantly reduce the frequency of falls (risk ratio = 0.63; 95% confidence interval (95% CI) 0.42–0.95; p = 0.03) in patients with osteoporosis, but demonstrated no remarkable influence on the results of the Berg Balance Scale (mean difference –3.66; 95% CI –12.04–4.72; p = 0.39) and Timed Up and Go test (mean difference –1.79; 95% CI –6.05–2.47; p = 0.41).
Conclusion: Balance training may significantly reduce the frequency of falls in patients with osteoporosis.
Key words: balance training; usual activities; falls; osteoporosis; meta-analysis.
Accepted Feb 23, 2018; Epub ahead of print May 16, 2018
J Rehabil Med 2018; 50: 00–00
Correspondence address: Hui Deng, Department of Orthopedics, Traditional Chinese Medicine Hospital of Shaoyang City, No. 115 Dongfeng Street, Shaoyang City, Hunan 422000 China. E-mail: 1788125530@qq.com
Balance training may be beneficial for patients with osteoporosis, although current study results are inconclusive. A systematic review and meta-analysis were carried out to explore the effect of balance training on falls in patients with osteoporosis. Six randomized controlled trials were included in the meta-analysis. Balance training intervention was found to significantly reduce the frequency of falls in patients with osteoporosis.
Osteoporosis increases the risk of fractures, commonly caused by falls (1, 2). Approximately 30% of people over 65 years of age experience a fall every year and almost 20% of them require medical care, which places a large burden on public health (3). Postural control refers to control of the body’s position in space for the purposes of stability and orientation (4). Falls and fractures are commonly caused by deficient postural control (5, 6). Patients with osteoporosis have an increased risk of falls, due to muscle weakness, spine kyphosis, and decreased postural control (7, 8). Falls in older people are associated with high mortality rates (33% in the first year) and morbidity (9–11).
Physical therapy interventions, including strength training, balance training, endurance, agility and muscular stretching, have been shown to be effective in decreasing the incidence of falls in elderly people (12, 13). Interventions that aim to improve the balance and posture of osteoporotic patients reduce the risk of falling and prevent fatal events or hospitalization. One study evaluating a balance training programme reported improved functional balance and decreased the number of falls in patients with osteoporosis after 12 months of intervention (14). In addition, a previous study demonstrated that a 12-month sensorimotor balance exercise programme could significantly increase static and dynamic postural balance, as well as reduce the number of falls, in osteoporotic women (3).
In contrast to these promising findings, no significant improvement in postural control was found after 10 weeks of balance and coordination exercises in osteoporotic patients (15). It has also been reported that a balance training programme had no influence on the Berg Balance Scale (BBS) and Timed Up and Go test (TUG) in patients with osteoporosis (14). Considering these inconsistent effects, we therefore conducted a systematic review and meta-analysis of randomized controlled trials (RCTs) to evaluate the effectiveness of balance training programmes on falls in patients with osteoporosis.
This systematic review and meta-analysis were conducted according to the guidance of the Preferred Reporting Items for Systematic Reviews and Meta-analysis statement (16) and the Cochrane Handbook for Systematic Reviews of Interventions (17). All analyses were based on previously published studies, and thus no ethical approval or patient consent was required.
PubMed, Embase, Web of Science, EBSCO, and the Cochrane Library were systematically searched from inception to July 2017, using the following key words: balance training or balance exercise, and osteoporosis or osteoporotic. To include additional eligible studies, the reference lists of retrieved studies and relevant reviews were also hand-searched and the process described above was repeated until no further article was identified.
The inclusion criteria were as follows: (i) study populations were patients with osteoporosis; (ii) intervention treatments were balance training intervention vs usual activities; (iii) studies were RCTs.
The following information was extracted from the included RCTs: first author, publication year, sample size, baseline characteristics of patients, balance training, control, study design, falls frequency, BBS, and TUG. The author would be contacted to acquire the data when necessary. The primary outcome was falls frequency. Secondary outcomes included BBS and TUG.
The Jadad Scale was used to evaluate the methodological quality of each RCT included in this study (18). This scale consists of 3 evaluation elements: randomization (0–2 points), blinding (0–2 points), and dropouts and withdrawals (0–1 points). One point would be allocated to each element if they have been mentioned in the article, and another point would be given if the methods of randomization and/or blinding had been appropriately described. If the methods of randomization and/or blinding were inappropriate, or dropouts and withdrawals had not been recorded, then 1 point was deducted. The Jadad Scale score ranged from 0 to 5 points. An article with Jadad score ≤ 2 was considered to be of low quality. If the Jadad score ≥ 3, the study was considered to be of high quality (19).
Mean differences (MDs) with 95% confidence intervals (95% CIs) for continuous outcomes (BBS and TUG), and risk ratios (RRs) with 95% CIs for dichotomous outcomes (falls frequency) were used to estimate the pooled effects. The value of the I2 statistic was used to select the appropriate pooling method: fixed-effects models were used for I2 < 50% and random-effects models for I2 > 50%. Sensitivity analysis was performed to detect the influence of a single study on the overall estimate via omitting 1 study in turn when necessary. Owing to the limited number (< 10) of included studies, publication bias was not assessed. p < 0.05 in two-tailed tests was considered statistically significant. All statistical analyses were performed with Review Manager Version 5.3 (The Cochrane Collaboration, Software Update, Oxford, UK).
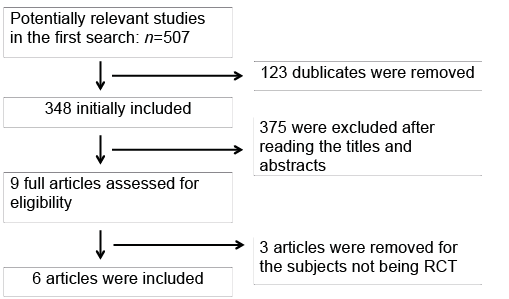
The flow chart for the selection process and detailed identification is shown in Fig. 1. A total of 507 publications were identified through the initial search of databases. Ultimately, 6 RCTs were included in the meta-analysis (3, 14, 15, 20–22).
Fig. 1. Flow diagram of study searching and selection process.
The baseline characteristics of the 6 eligible RCTs in the meta-analysis are summarized in Table I. The included studies were published between 2001 and 2017, and sample sizes ranged from 33 to 100, with a total of 424. There were no significant differences in age, body mass index (BMI) (or body mass), and fall history between the balance training groups and the control groups at baseline. The length of the balance training programmes ranged from 8 weeks to 12 months. Three of the included RCTs involved a 12-month balance training programme (3, 14, 22), and the other 3 included RCTs involved 8-week (21), 10-week (15), and 12-week balance training programmes (20).
Among the 6 RCTs, 2 reported falls frequency (3, 22), 2 reported BBS (3, 14), and 2 reported TUG (3, 14). The data in 3 of the 6 quality-assessed studies were not applicable in our meta-analyses. Jadad scores of the 6 included studies varied from 3 to 5, and all 6 studies were considered to be high-quality according to quality assessment.
This outcome variable was analysed with the fixed-effects model, and the pooled estimate of the 2 included RCTs suggested that, compared with a control group for osteoporotic patients, balance training intervention was associated with a significantly decreased frequency of falls during the follow-up (RR = 0.63; 95% CI = 0.42–0.95; p = 0.03), with no heterogeneity among the studies (I2 = 0%, heterogeneity p = 0.61) (Fig. 2).
Fig. 2. Forest plot for the meta-analysis of falls frequency.
No heterogeneity was observed among the included studies for the frequency of falls. Thus, we did not perform sensitivity analysis by omitting one study in turn to detect the source of heterogeneity.
Compared with control interventions, balance training interventions had no significant influence on BBS (MD –3.66; 95% CI = –12.04–4.72; p = 0.39; Fig. 3) and TUG (MD –1.79; 95% CI = –6.05–2.47; p = 0.41; Fig. 4) results in osteoporotic patients.
Fig. 3. Forest plot for the meta-analysis of Berg Balance Scale (BBS).
Fig. 4. Forest plot for the meta-analysis of Timed Up and Go test (TUG).
Over 40% of women worldwide will sustain a fracture due to osteoporosis during their lifetime according to the International Osteoporosis Foundation, which may result in remarkably increased morbidity/mortality and reduced quality of life (e.g. restriction of mobility, disability, social isolation, insecurity and fear) (23–25). It is estimated that 90% of all hip fractures are caused by falls and that hip fracture is the sixth leading cause of death among patients aged over 65 years (26, 27). Reducing the incidence of falls is an important approach to decrease health costs and improve quality of life in older patients (28).
One recent review confirmed that a home-based exercise programme was able to reduce the rate of falls and risk of falling (29). In particular, a balance training programme was revealed to effectively prevent falls and improve quality of life in elderly people (22, 30). Altered balance was the greatest contributor to falls in elderly people (31). Good postural balance could reduce the risk of fractures through improving postural stability, mobility and diminishing the risk of falls (32). The current meta-analysis clearly suggests that, compared with control interventions, balance training programmes are associated with a significantly reduced frequency of falls in osteoporotic patients.
The BBS, consisting of 14 items in activities of daily living, was used to evaluate functional balance, and each item possessed an ordinal scale of 5 alternatives, ranging from 0 to 4 points (33). The TUG was applied to assess the functional mobility and recorded the time an individual took to get up out of a chair, walk 3 m, turn around, walk back and sit down again (34). The TUG and the BBS aimed to evaluate the balance in a functional approach. Postural study using a computerized method was a physiological test to examine the swaying movement of the body. One included RCT concluded that a balance training programme not only improved functional balance, but also increased postural balance based on stabilometric measurements (3). However, the BBS and TUG results in our meta-analysis demonstrated no significant difference in functional balance between balance training programmes and control groups.
Significant heterogeneity was found in the meta-analysis of BBS and TUG. One included RCT reported that there was no significant difference in BBS and TUG scores at the end of follow-up between balance training group and control group, but the change in BBS and TUG from baseline in the balance training group was significantly higher than in the control group, indicating that balance training could significantly improve functional balance. Thus, this significant heterogeneity was caused by the different baseline of the BBS and TUG.
Several limitations should be taken into account. Firstly, our analysis was based on only 6 RCTs, 5 of which had a relatively small sample size (n<100). Overestimation of the treatment effect is more likely in smaller trials compared with larger samples. In addition, only 2 studies were included in each of the meta-analysis and the results should be interpreted with caution. More clinical trials with larger samples are needed to explore this issue. The periods, methods and follow-up of balance training in the included studies were different, which may have an influence on the pooling of results. Next, there was significant heterogeneity in the meta-analysis of BBS and TUG due to their different baselines. Finally, unpublished and missing data might lend bias to the pooled effect.
Balance training may have an important ability to reduce the incidence of falls in osteoporotic patients, and thus can be recommended for patients with osteoporosis.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize