
From the 1Cheokbareun Rehabilitation Clinic, Pohang-si, Gyeongsangbuk-do, 2Department of Medical Statistics, College of Medicine, Catholic University of Daegu, Daegu, and 3Department of Physical Medicine and Rehabilitation, College of Medicine, Yeungnam University Republic of Korea
Objective: Central pain can occur following traumatic brain injury, leading to poor functional recovery, limitation of activities of daily living, and decreased quality of life. The aim of this study was to determine whether high-frequency (10 Hz) repetitive transcranial magnetic stimulation, applied over the primary motor cortex of the affected hemisphere, can be used to manage chronic central pain after mild traumatic brain injury.
Design: Prospective randomized feasibility study.
Methods: Twelve patients with mild traumatic brain injury and chronic central pain were randomly assigned to transcranial magnetic stimulation (high-frequency stimulation, 10 sessions) or sham groups. Diffuse tensor tractography revealed partially injured spinothalamocortical tracts in all recruited patients. A numerical rating scale (NRS) was used to evaluate pain intensity during pre-treatment and immediately after the 5th transcranial magnetic stimulation session (post1), 10th transcranial magnetic stimulation session (post2), and 1 (post3), 2 (post4), and 4 weeks (post 5) after finishing treatment. Physical and mental health status were evaluated using the Short Form 36 Health Survey (SF-36), including physical and mental component scores (PCS, MCS).
Results: The NRS score of the repetitive transcranial magnetic stimulation group was significantly lower than the sham group score at all clinical evaluation time-points during and after transcranial magnetic stimulation sessions. The transcranial magnetic stimulation group’s SF-36 PCS score was significantly higher at post2, post3, post4, and post5 compared with the sham group.
Conclusion: High-frequency transcranial magnetic stimulation may be used to manage chronic central pain and improve quality of life in patients with mild traumatic brain injury. However, this is a pilot study and further research is needed.
Key words: central pain; traumatic brain injury; repetitive transcranial magnetic stimulation; high-frequency; spinothalamocortical tract; diffusion tensor tractography.
Accepted Dec 21, 2017; Epub ahead of print Jan 31, 2018
J Rehabil Med 2018; 50: 00–00
Correspondence address: Min Cheol Chang, Department of Physical Medicine and Rehabilitation, College of Medicine, Yeungnam University 317-1, Daemyungdong, Namku, Daegu, 705-717, Republic of Korea. E-mail: wheel633@gmail.com
Traumatic brain injury (TBI) is defined as damage to the brain resulting from external mechanical force. TBI can cause various types of disability, and is classified as mild, moderate, or severe on the Glasgow Coma Scale (GCS) (1). A GCS score of 13–15 is defined as mild, 9–12 as moderate, and 3–8 as severe (2). Of the total number of cases of TBI, 70–90% are classified as mild (3, 4). Chronic pain is a frequent occurrence in patients with mild TBI; prevalence is reported to be up to 75% (5, 6). Chronic pain is defined as persistent or recurrent pain lasting longer than 3 months and is associated with significant emotional distress or significant functional disability (7). Chronic pain after TBI leads to poor functional recovery, limited activities of daily living, and decreased quality of life (6). Central pain, one of the various types of pain following TBI, is caused by a lesion or dysfunction of the somatosensory nervous system in the central nervous system. It presents as neuropathic pain, which is characteristically described as burning and hyperpathic (8, 9). Patients with central pain usually experience sensations of chilling, itching, tingling, and numbness, in addition to pain. They can also experience abnormal sensations that feel like electrical shocks or burns, and that worsen when numb areas are touched (10, 11). Central pain is caused by an injury to the lamina I spinothalamocortical pathway. It was suggested that central pain is a release phenomenon that results from loss of the inhibitory effect of pain processing on the emotional aspects of pain (12). The spinothalamocortical tract (STT) is a major component of the lamina I spinothalamocortical pathway, and several studies have demonstrated that injury of the STT is one of the primary pathogenetic mechanisms of central pain following TBI (13–15). Various medications and techniques have been applied to manage central pain, but many patients with central pain continue to report uncontrolled pain after application of these therapeutic tools (16).
Repetitive transcranial magnetic stimulation (rTMS) is a safe, non-invasive, effective therapeutic intervention that uses an electromagnetic coil applied to the scalp to produce a magnetic field. This induces changes in cortical excitability at the stimulation site and transsynaptically in distant areas (17, 18). High-frequency (≥ 5 Hz) stimulation increases cortical excitability, whereas low-frequency stimulation (1 Hz) decreases it (19, 20). Application of high-frequency unilateral rTMS to the motor cortex in patients with chronic pain has been shown to have long-term analgesic effects (21–23). Several previous studies have demonstrated the effectiveness of managing various chronic pain conditions, including neuropathic pain, fibromyalgia, complex regional pain syndrome, and myofascial pain syndrome (21–23). However, no study has evaluated the effect of rTMS on central pain following TBI.
The current study investigated the effects of high-frequency (10 Hz) rTMS applied over the primary motor cortex (M1) for the management of medically intractable chronic central pain after mild TBI.
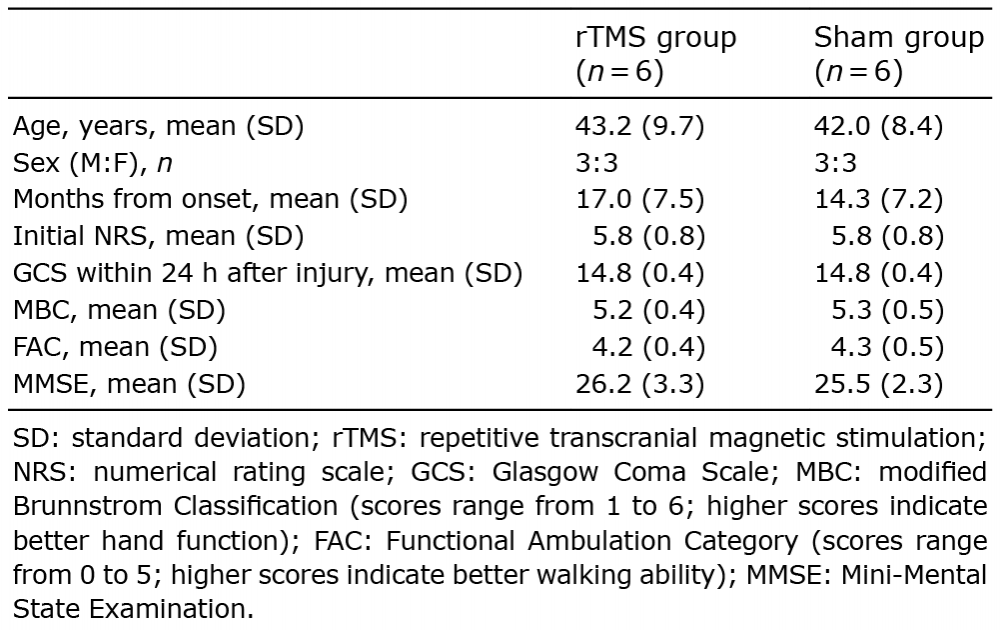
Twelve consecutive patients with mild TBI were prospectively recruited to the study (6 males, 6 females; mean age 42.6 (standard deviation (SD) 8.7) years; age range 30–56 years; 15.7 (SD 7.1) months from onset) who received comprehensive rehabilitation management in the Department of Physical Medicine and Rehabilitation at Department of Physical Medicine and Rehabilitation at Union hospital (Table I). Patients were recruited according to the following criteria: (i) first ever TBI; (ii) loss of consciousness for less than 30 min, initial GCS score 13–15, and post-traumatic amnesia for ≤ 24 h; (iii) no brain lesion on conventional magnetic resonance imaging (MRI); (iv) ≥6 months after TBI onset; (v) age 20–70 years; (vi) significant central pain (shooting, lancinating, burning, electric shock-like pain) accompanied by sensory deficit in the unilateral body with a minimum score of 4 on the NRS (0 indicating no pain and 10 indicating the most severe pain) lasting at least 6 months; (vii) no change in NRS pain score over 4 weeks despite pain medication (pregabalin and tramadol/acetaminophen); (viii) injury of STT corresponding to the painful side (i.e. injury of STT on the hemisphere contralateral to the painful body) on diffusion tensor tractography (DTT) (14, 15) performed after 1 month from onset of TBI; (ix) no evidence of radiculopathy or peripheral neuropathy on electromyography or peripheral neuropathy; (x) no evidence of other possible causes of neuropathic pain, including radiculopathy, myelopathy, and peripheral neuropathy; and (xi) absence of contraindications for TMS, such as a history of epileptic seizure, the presence of metal in the skull, or pacemaker placement. All subjects provided written informed content prior to the study, and the local ethics committee approved the study protocol. Patients were informed of the goals of the study.
Table I. Patient demographic and initial clinical data
DTT was used to demonstrate the STT injury. DTT was performed at mean 2.6 (SD 1.2) months after onset in our patients using a sensitivity-encoding head coil on a 1.5-T Philips Gyroscan Intera (Hoffman-LaRoche Ltd., Best, The Netherlands) with single-shot echo-planar imaging and navigator echo. Sixty contiguous slices (acquisition matrix = 96 × 96; reconstruction matrix = 192 × 192; field of view = 240 × 240 mm2; repetition time (TR) = 10,726 ms; echo time (TE) = 76 ms, b = 1,000 s/mm2, number of excitations (NEX) = 1, thickness = 2.5 mm) were acquired for each of the 32 non-collinear diffusion-sensitizing gradients. Fibre tracking was performed using the Oxford Centre for Functional Magnetic Resonance Imaging of the Brain (FMRIB) Software Library (FSL; www.fmrib.ox.ac.uk/fsl). Affine multi-scale 2-dimensional registration was used for correction of head motion effects and image distortion due to eddy current. Fibre tracking was performed using a probabilistic tractography method based on a multi-fibre model and applied in the current study utilizing tractography routines implemented in FMRIB Diffusion (5,000 streamline samples, 0.5-mm step lengths, curvature thresholds = 0.2). The STTs were placed by selection of fibres passing through regions of interest (ROIs). A seed ROI was placed on the posterolateral medulla on an axial slice, and a target ROI was placed on the primary somatosensory cortex on an axial slice. The threshold of one streamline was applied for the results of fibre tracking. Values of fractional anisotropy (FA) and tract volume (TV) of each ROI were measured. DTT was also performed and STT values measured in both hemispheres in 30 healthy control subjects (10 subjects in each age group (30s, 40s, and 50s)) with no history of psychiatric, neurological, or physical illness and no brain lesion on conventional MRI. Participation in the study was voluntary. Values for each patient were compared with those of 30 healthy control subjects. Patients were defined as having STT injury when FA and TV values of the STT were greater than 2 SD lower than those of control patients.
In DTT findings, the STTs corresponding to the painful side showed partial tearing in all recruited patients (Fig. 1). The FA and TV values in the affected STTs were found to be greater than 2 SD lower than those of control patients (Table II).
Fig. 1. (A) Spinothalamocortical tracts (STTs) of a 35-year-old woman with mild traumatic brain injury. The STT in the right hemisphere is partially torn, and is thinner (open blow arrow) than that in the left hemisphere or that of a 35-year-old woman in the control group. (B) STT of a subject in the control group.
Table II. Diffusion tensor image parameter values of injured spinothalamocortical tracts in patients and intact spinothalamocortical tracts in controls
This study was designed and performed as a prospective, randomized, controlled clinical trial. Twelve patients were randomly assigned to 2 groups: the rTMS or sham groups (n = 6 patients per group). Randomization was performed using a random table. The patients were blinded to their group assignment throughout the study. Each patient underwent 10 consecutive sessions (Monday to Friday, 5 times per week for 2 weeks).
The rTMS stimulating location was above the abductor pollicis brevis (APB) muscle area of the precentral gyrus in the affected hemisphere. To confirm the exact location of this area, the optimal scalp site for the affected cortex was determined using TMS. TMS was performed using a Magstim Super Rapid Magnetic Stimulator (The Magstim Co., Whitland, Carmarthenshire, UK), with a 70-mm, air-cooled coil in the shape of a figure-of-eight. A cloth marked with 1-cm spacing and Cz-referenced to the intersection of the midsagittal and interaural lines was placed on the scalp. Subjects were seated in a comfortable chair with foam earplugs during TMS. The motor threshold (MT) was defined as the minimum stimulus required to elicit a motor evoked potential (MEP) with a peak-to-peak amplitude > 50 μV in 3 of 5 consecutive trials in the APB. If the MT was < 80%, the stimulation intensity was set to MT plus 20%; if the MT was > 80%, then intensity was set to 100% of the stimulator output. MEPs were obtained from the APB muscle. Each site was stimulated 5 times at 1-cm intervals, with a minimum of 10 s between stimulations. The optimal scalp site for rTMS stimulation in the affected hemisphere was determined, where the stimuli evoked the motor potentials with maximal peak-to-peak amplitude. MEPs of the affected hemisphere were obtained for all evaluated patients.
For the patients in the rTMS group, treatment was administered over the optimal scalp site at 10 Hz, with an intensity of 90% of the MT and duration of 5 s, for a total of 20 trains separated by 55-s intertrain pauses (a total of 1,000 pulses) (24). The coil was placed tangentially to the scalp at an approximate angle of 45° backward and laterally. The sham stimulation was administered using the same protocol, but the angle of the coil was at 90º, perpendicular to the skull rather than tangential to it. Thus, the magnetic field could not penetrate the brain, although the subjects could hear the sound that was produced. The researcher who applied the rTMS or sham stimulations were different from the investigator who performed the clinical evaluation. The researcher who applied the rTMS or sham stimulation was aware of the goals of the study, but the investigator who measured the clinical outcome was not informed of the goals.
The assessment of therapeutic effects was performed prior to the start of the study (pre), immediately after the 5th rTMS session (post1) and 10th rTMS session (post2), and at 1 (post3), 2 (post4), and 4 weeks (post5) after finishing the rTMS sessions (Fig. 2). One investigator assessed clinical outcomes at pretreatment and follow-up periods. The investigator was blinded to the grouping of the patients and did not participate in rTMS stimulation. The intensity of the central pain was rated by the patients using the NRS, with values between 0 and 10, set as “no pain” and “the most intense pain imaginable,” respectively (25).
The secondary outcome measurement was performed using the Short Form 36 Health Survey (SF-36), which is a well-known generic measure of health-related quality of life (26). The SF-36 includes 2 separate subscales; the physical component score (PCS) and the mental component score (MCS). The PCS and MCS, reflecting overall physical and mental health status, respectively, are derived from the 8 original scales of the SF-36. The PCS and MCS of SF-36 were measured at pretreatment and follow-up periods.
Fig. 2. Study design, depicting the treatment protocol and assessment time-points for the 2 subject groups. rTMS: repetitive transcranial magnetic stimulation.
Data were analysed using the Statistical Package for Social Science (SPSS, v. 22.0, IBM Corporation, Armonk, NY, USA). A summary of the characteristic variables was performed using descriptive analysis; the values for quantitative variables were presented as mean and SD. Demographic data were compared between the 2 groups using a Mann–Whitney U test and χ2 test. A generalized linear model analysis was used to compare changes in clinical data between groups over time. A normal distribution was used for the link function. Bonferroni corrections were used to compensate for multiple comparisons. The level of statistical significance was set at p < 0.05.
All patients completed their rTMS sessions. No adverse side-effects of rTMS therapy were reported during the course of the experiment. There were no significant intergroup differences in demographic data (p>0.05) (Table I). The mean modified Brunnstrom Classification and Functional Ambulation Category (FAC) scores were 5.3 (SD 0.5) and 4.3 (SD 0.5) (indicating that patients had minimal to mild motor weakness).
The changes in the NRS score over time were significantly different between groups (p < 0.001) (Fig. 3A). The NRS score was significantly lower in the rTMS group than in the sham group at post1, post2, post3, post4, and post5 (pre vs. post1: p = 0.003, vs. post2: p < 0.001, vs. post3: p < 0.001, vs. post4: p < 0.001, vs. post5: p < 0.001) (Fig. 3A). In addition, changes in the SF-36 PCS score over time were significantly different between the 2 groups (p < 0.001) (Fig. 3B). A significantly higher increase in SF-36 PCS score in the rTMS group was observed at post2, post3, post4, and post5 compared with that in the sham group (pre vs. post1: p = 0.408, vs. post2: p = 0.006, vs. post3: p < 0.001, vs. post4: p < 0.001, vs. post5: p < 0.001) (Fig. 3B). In contrast, the SF-36 MCS scores did not change significantly over time. However, the scores of the rTMS group tended to be higher than those of the sham group (p = 0.100) (Fig. 3C).
Fig. 3. Change in (A) numerical rating scale (NRS), (B) physical component score (PCS) and (C) mental component score (MCS) of the Short-Form 36 (SF-36) health survey in the repetitive transcranial magnetic stimulation (rTMS) and sham groups. The NRS score at post1, post2, post3, post4, and post5 was significantly lower in the rTMS group than in the sham group. A significantly higher increase in the SF-36 PCS score in the rTMS group was shown at post2, post3, post4, and post5, compared with the sham group. In contrast, the score of the SF-36 MCS did not change significantly over time. However, the rTMS group score tended to be higher than that of the sham group. *p < 0.05: intergroup comparison at each time-point (generalized linear model analysis).
In the current study, we evaluated the effect of high-frequency (10 Hz) rTMS on the M1 for the management of central pain in patients with chronic TBI. Our results showed that the severity of pain, as measured with the NRS, decreased significantly after high-frequency rTMS on the M1, and the decrease in pain persisted for at least 4 weeks after completion of rTMS treatment. In addition, the SF-36 PCS scores were significantly increased after completion of rTMS sessions compared with the sham group, and the increase was sustained for at least 4 weeks after finishing rTMS treatment. The SF-36 MCS scores tended to be higher after rTMS sessions. Higher SF-36 PCS and MCS scores are indicative of higher physical and mental quality of life, respectively. Therefore, our results indicate that rTMS treatment can provide better physical and mental quality of life in patients with chronic central pain following mild TBI. rTMS could be a beneficial treatment option for management of chronic central pain due to mild TBI and for improvement in the quality of life.
In 2006, Hirayama et al. (27) recruited 20 patients with intractable neuropathic pain and conducted high-frequency rTMS stimulation on M1, postcentral gyrus, premotor area, and supplementary motor area. They concluded that M1 is the sole target that can alleviate neuropathic pain. The mechanism of pain reduction after rTMS stimulation has not been clearly elucidated, but there are several possible mechanisms of central pain-reducing effects of rTMS on the M1. Previous fMRI studies showed that rTMS applied to the M1 induces alterations in the activity of cortical and subcortical structures related to pain processing and modulation, such as the medial thalamus, anterior cingulate, orbitofrontal cortices, and periaqueductal grey matter (28, 29). We believe that rTMS can modify abnormal thalamocortical excitation of the sensory system, triggering cascades of analgesic synaptic events in several pain-related structures. Moreover, rTMS of the M1 was thought to reduce neuropathic pain by triggering descending inhibitory pathways to act at the dorsal horn level (30). Another possibility is that rTMS relieved pain by improving blood flow in the affected area. It is known that there is a decrease in cerebral blood flow during chronic pain (31), and rTMS of M1 increased cerebral blood flow in patients with neuropathic pain on positron emission tomography (31, 32). In addition, in an animal study, the anti-nociceptive effects of cortical stimulation were found to change neuronal activities in the periaqueductal grey matter associated with pain processing (33). In addition, de Andrade et al. (21) reported that rTMS applied to the M1 influences the endogenous opioid system, which can subsequently control various types of pain.
In addition, DTT analysis was performed for the accurate diagnosis of central pain. Patients who showed decreased FA and TV values of STT corresponding to the painful side were recruited. The decrease in FA values resulted from deterioration in directional microstructures, such as the axon, myelin, and microtubules (34). Deterioration in neuronal microstructures in a neural tract can result in TV reduction (34). A decrease in FA and TV values in our patients indicated damage to the STT. It is known that an STT lesion is a necessary condition of central pain after stroke (35–37). Likewise, several previous studies reported that development of central pain after TBI is ascribed to injury of the STT (13–15). In our patients, injury of the STT seems to have caused central pain. In addition, because no abnormality was found in conventional brain MRIs of any of the patients, traumatic axonal injury was the most likely pathogenic mechanism for this injury (38, 39).
Several previous studies have demonstrated the positive effects of rTMS on the motor cortex (M1 or dorsolateral prefrontal cortex) for control of central pain after a stroke (24, 40–49), and its effect persisted for approximately 2–4 weeks (24, 40, 42, 44, 49). However, thus far, no study has examined the effectiveness of rTMS for management of central pain following TBI.
In conclusion, this study found that chronic central pain after mild TBI refractory to oral analgesics was significantly reduced immediately after the fifth and tenth sessions of rTMS, and 1, 2, and 4 weeks after finishing high-frequency rTMS treatment applied over the M1 in the affected hemisphere. Physical quality of life was improved during and after rTMS sessions in the rTMS group. Thus, rTMS would be a useful therapeutic option for patients with chronic central pain after mild TBI. This is the first study to demonstrate the effectiveness of high-frequency rTMS over the M1 in TBI patients with chronic central pain. However, this study has several limitations. First, it did not evaluate serial changes in the clinical data during the 2-week treatment session and the 4-week period after treatment. Secondly, it did not investigate the long-term effects of therapy beyond 4 weeks. Thirdly, the number of recruited patients was small. Fourthly, the sham stimulation mimicked only the sound of the coil discharge, and could not mimic cutaneous sensations or twitches of scalp muscles during rTMS stimulation. Lastly, a placebo effect should have been considered when interpreting the results. Because this is a pilot study designed to guide future research, it is not appropriate to generalize the results. Future studies involving large numbers of subjects and addressing the other limitations of the current study are necessary to confirm the findings.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize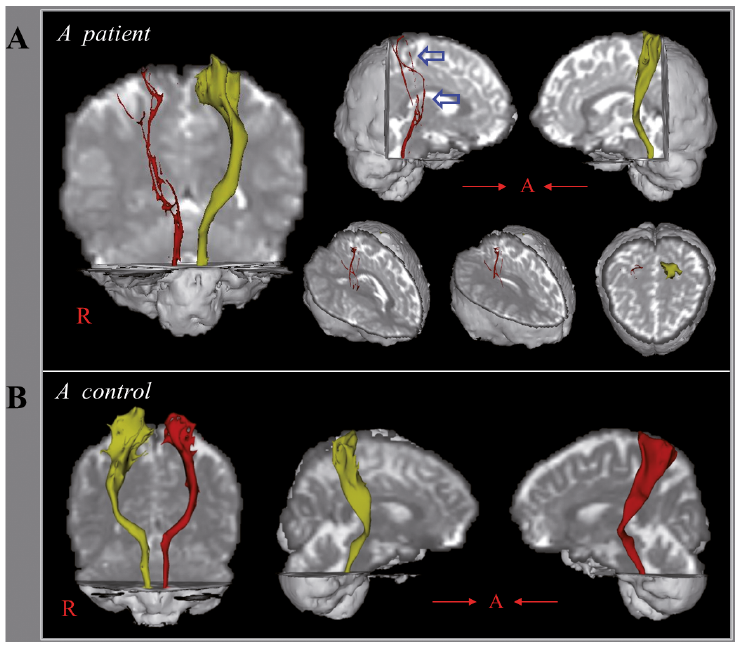 Click to show fullsize
Click to show fullsize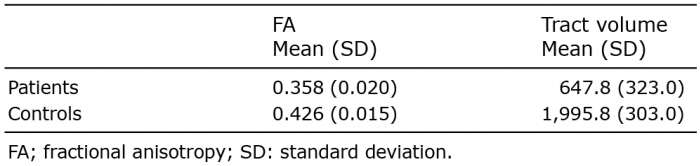 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize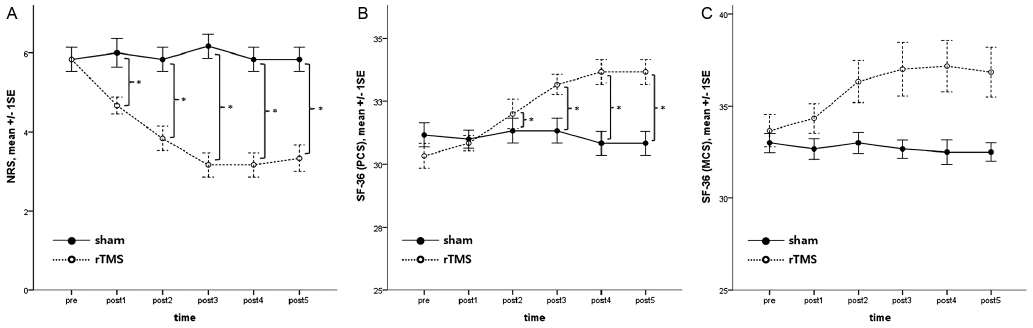 Click to show fullsize
Click to show fullsize