
From the 1Department of Rehabilitation Medicine, 2Australian Rehabilitation Research Centre, Royal Melbourne Hospital, 3Department of Medicine (Royal Melbourne Hospital), The University of Melbourne, Parkville, Victoria, Australia, 4Department of Physical and Rehabilitation Medicine, St Jozef, Bornem, 5CBR team international, Gent Area, Belgium, 6Center for Genomic and Precision Medicine, College of Medicine, University of Ibadan, and WFNR-Blossom Specialist Medical Center, Ibadan, Nigeria, 7Paraplegic Center, Hayatabad, Peshawar, Pakistan, 8Laboratory of Clinical Neurosciences, Faculty of Medicine, University Sidi Mohamed Ben Abdellah; and Department of Physical and Rehabilitation Medicine, University Hospital Hassan II, Fez, Morocco, 9ISRA Institute of Rehabilitation Sciences, Islamabad, 10Armed Forces Institute of Rehabilitation Medicine, Rawalpindi, 11Akbar Kare Institute, Hayatabad, Peshawar, Pakistan, 12Rehabilitation Medicine Unit, Department of Orthopedics and Traumatology, Hospital University Kebangsaan Malaysia, Kuala Lumpur, Malaysia, and 13Department of Physical and Rehabilitation Medicine, University Mohammed Premier, Oujda, Morocco
Objective: Despite the prevalence of disability in low-and middle-income countries, the clinical skills of the rehabilitation workforce are not well described. We report health professionals’ perspectives on clinical skills in austere settings and identify context-specific gaps in workforce capacity.
Methods: A cross-sectional pilot survey (Pakistan, Morocco, Nigeria, Malaysia) of health professionals working in rehabilitation in hospital and community settings. A situational-analysis survey captured assessment of clinical skills required in various rehabilitation settings. Responses were coded in a line-by-line process, and linked to categories in domains of the International Classification of Functioning, Disability and Health (ICF).
Results: Respondents (n = 532) from Pakistan 248, Nigeria 159, Morocco 93 and Malaysia 32 included the following: physiotherapists (52.8%), nurses (8.8%), speech (5.3%) and occupational therapists (8.5%), rehabilitation physicians (3.8%), other doctors (5.5%) and prosthetist/orthotists (1.5%). The 10 commonly used clinical skills reported were prescription of: physical activity, medications, transfer-techniques, daily-living activities, patient/carer education, diagnosis/screening, behaviour/cognitive interventions, comprehensive patient-care, referrals, assessments and collaboration. There was significant overlap in skills listed irrespective of profession. Most responses linked with ICF categories in activities/participation and personal factors.
Conclusion: The core skills identified reflect general rehabilitation practice and a task-shifting approach, to address shortages of health workers in low-and middle-income countries.
Key words: disability; rehabilitation; skills; low- and middle-income countries.
Accepted Nov 17, 2017; Epub ahead of print Feb 28, 2018
J Rehabil Med 2018; 50: 00–00
Correspondence address: Fary Khan, Department of Rehabilitation Medicine, Royal Melbourne Hospital, 34-54 Poplar Road Parkville, Melbourne VIC 3052, Australia. E-mail: fary.khan@mh.org.au
The worldwide prevalence of disability is escalating, due to an ageing population, an increase in non-communicable diseases (NCDs) and natural/man-made disasters (1, 2). The World Report on Disability estimates that there are over 1 billion people with disabilities, equating to 15% of the world population (2). Of these, 110–190 million have significant difficulties, such as inability to walk, perform self-care, communicate or participate in education or employment (2). An estimated 80% of persons with disability (PwD) live in low- and middle-income countries (LMICs) (1).
In most developing countries, healthcare is directed primarily at the curative/preventive aspects of disease, whilst rehabilitation is a lesser priority (3). Usually PwD in LMICs are more dependent on rehabilitative care, often economically deprived, and affected by constraints in provision of sustainable healthcare systems (1). Globally, only 3% of individuals in LMICs who need rehabilitation receive the service (2, 4) and an estimated 30 million people require over 180,000 rehabilitation professionals (5, 6). A global survey of government action (n = 114 countries) on the implementation of United Nations Standard Rules on Equalization of Opportunities for PwD reported that rehabilitation policies were not adopted in 48 countries (42%), legislation on rehabilitation not passed in half (50%) of the member states, and rehabilitation programmes not established in 46 countries (40%) (4). Furthermore, a third of countries globally did not allocate specific budgets towards rehabilitation services (2).
The WHO’s “Global Disability Action Plan 2014–2021: Better health for all people with disability” (GDAP) lists specific actions for strengthening rehabilitation, including access, workforce capacity, community-based rehabilitation and research (7). The WHO defines rehabilitation as “a set of interventions that optimize functioning and reduce disability in individuals with health conditions (disease (acute or chronic), injury or trauma) in interaction with their environment” (8). Primary goals of medical rehabilitation are to address impairments, and improve activity/participation within contextual factors (9), as per the International Classification of Function, Disability and Health (ICF) (10).
Rehabilitation workforce and capacity-building initiatives in LMICs have been prioritized by the International Society of Physical and Medical Rehabilitation (ISPRM), in line with the WHO directive. It is recognized that the role of the rehabilitation professional is a complex mix of skill and training. In many LMICs, there is a shortage of workers with appropriate rehabilitation skills, resulting in task-shifting practices. This approach can strengthen health workforce teams, where appropriate, from highly qualified health personnel to those with lesser qualifications and training for a more efficient use of available human resources (11). For rehabilitation services in many LMICs, there are challenges within operational healthcare systems in terms of policy, funding structure/infrastructure, capacity, human and physical resources, and technology (12–14). The models of care are diverse, as are interventions, modalities and skill-sets amongst the rehabilitation workforce (12, 15). The skills (and competencies) of rehabilitation personnel are pivotal to effective delivery of care (16). In current environment of increasing demand and changing models of service delivery, enhancing and maintaining workforce skills is imperative (11, 16).
Although limitations associated with infrastructure and human resources (including “required” skills) have been identified, there are, to date, no instruments designed to evaluate health system capacity and/or skills of rehabilitation professionals working in LMICs (17). The estimation-based data for rehabilitation service provision (skills/competencies of rehabilitation personnel) are sparse, especially in LMICs (17). Specific data about the skill-base of the rehabilitation workforce and capacity will determine the adequacy of current levels of care provided, and for future planning of services and training the workforce to meet demands of the disabled population. This pilot study used a survey tool to obtain information from health professionals working in the rehabilitation field in LMICs, with a focus on the clinical skills required in such settings, and to identify context-specific gaps in rehabilitation for skills and capacity building.
An exploratory descriptive study with a cross-sectional survey design.
The survey was distributed in various healthcare settings in LMICs (urban/rural, primary/secondary/tertiary level healthcare and community settings, military/civilian establishments, government/non-governmental organizations (international non-governmental organizations (INGOs) and non-governmental organizations (NGOs)) in Pakistan, Nigeria, Morocco and Malaysia in February–March 2017. This exercise was approved by the Royal Melbourne Hospital (HREC number: QA2017083). Written approval was obtained from each institution distributing the surveys prior to commencement.
The participants were healthcare professionals currently working in rehabilitation-related healthcare institutions in LMICs, including rehabilitation physicians, other medical practitioners (general practitioners, neurologists, etc.), nurses, allied health professionals, community workers, health managers or policy-makers and those working in austere and community settings. Since no list of potential survey participants was available in these LMICs, existing rehabilitation service contacts were utilized for snowballing/respondent-driven sampling within a range of rehabilitation networks. This technique uses a referral system whereby the initial respondents identify and/or suggest further relevant participants in the field known to them (18). The survey was distributed by the local healthcare institution, which invited the eligible participants. Completion of the survey was voluntary, and return of the survey itself implied consent.
For the purpose of this study a clinical skill was defined as “an act with the aim of improving health or quality of life for an individual. This can be across any domain of examination – physical, therapeutic, communication or management” (19).
As no previous comprehensive survey instruments were available to obtain the required information, a situational-analysis survey tool (Appendix SI) specific for rehabilitation was modified from a previously published tool (17). This pilot survey was designed to provide a cross-sectional assessment of clinical skills required in various rehabilitation settings, human resources and types of rehabilitation interventions provided. The survey content was organized into subsections, namely: human resources, skills and competencies of personnel available, rehabilitation interventions provided, and gaps in service provision in local settings. The survey was translated into the local language, where necessary. Various open-ended sections of the questionnaire provided respondents with an opportunity to supply information on their skills and competencies, as well as comments about the state of rehabilitation services and gaps relevant to their setting. Each of the skill categories was named and defined based on previous studies (17). The respondents’ words or sentences explaining their clinical skills were then sorted into the relevant skill categories.
All institutional and respondent identification information was removed prior to analysis. The surveys were secured and filed in the Department of Rehabilitation Medicine at the Royal Melbourne Hospital, and opened only at the time of data entry into a special study database by an independent data entry officer. All data were collated using the content analytical technique (17). Two authors (BA, FK) scrutinized each response and coded the information using a line-by-line process, which was further clustered into a common-term based on the ICF (10) to classify the categories of skills in terms of their target. Each term was categorized according to the ICF domains of body structure or function, activity/participation, environmental factors or personal factors. The ICF framework encapsulates the social model of disability, which is core to rehabilitation values (17). Where there were discrepancies in categorization, the final consensus was made by discussion amongst authors. The authors then refined and finalized the content analysis.
Descriptive analyses described the study population. The frequency of terms reported by respondents was calculated as a percentage. The most frequent skills (“high frequency”) for each domain were analysed for comparisons by geographical region, professional groups (such as rehabilitation physicians, physiotherapists, etc.). All data were de-identified, entered twice to avoid errors on data entry and analysed by 1 of the researchers. IBM SPSS Statistics Package Version 21 (Chicago, IL, USA) SPSS 12 for Windows was used for analyses.
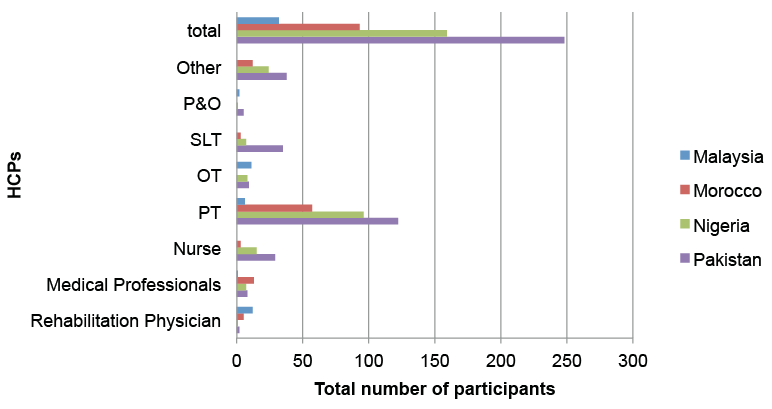
A total of 532 respondents in 4 LMICs completed the survey; these included: Pakistan = 248 (46.6%); Nigeria = 159 (29.9%); Morocco = 93 (17.5%) and Malaysia = 32 (6.0%) (Fig. 1). All worked within a rehabilitation setting (public and/or private) affiliated with a hospital or community setting with PwD in the last 3 months.
Fig. 1. Number of participants by professions from the 4 countries (n=532). OT; occupational therapists; P&O: prosthetics and orthotics; PT: physiotherapists; SLT: speech and language therapists.
Survey participants were from a range of professional backgrounds. The majority were physiotherapists (PT) = 281 (52.8%), nurses = 47 (8.8%), speech therapists (SLT) = 45 (8.5%), medical practitioners (including GPs, neurologists, general physicians) = 29 (5.5%), rehabilitation physicians = 20 (3.8%), occupational therapists (OT) = 28 (5.3%), prosthetists and orthotists (P&O) = 8 (1.5%). (Figs 1 and 2)
Most participants (63.6%) worked in government-funded public institutional services, 22.1% in the private sector, and 7.6% in peripheral community healthcare centres.
Fig. 2. Number of participants by profession (n=532). Numerical shown indicated n (total number), %. OT: occupational therapists; P&O: prosthetics and orthotics; PT: physiotherapists; SLT: speech and language therapists.
Mean (standard deviation) years of experience working within the rehabilitation sector was 7.6 (7.4) years (range 0.2–39 years). Level of education varied, with almost half the participants (48.3%) reportedly completing a Diploma in their profession, 38% a Masters degree and 8% a Doctorate.
Within the 3 months prior to the survey, the majority of participants (94.2%) reported spending their working time with PwD: 33.4% reported spending most of their working hours, 26% half of their working hours and 25% spent one-quarter of their time with PwD. There was a range of types of disabilities (case mix) treated, with half the participants (52.6%) working with PwD who had more than 2 disabilities. Most participants 70.3% (n = 374) focussed on mobility issues, 49.3% (n = 262) on self-care, 37.2% (n = 198) on communication, 30.6% (n = 163) on upper body function and 30.5% (n = 162) on cognitive problems.
Participants provided multiple responses and a range of terms for clinical skills with significant overlap, indicating a task-shifting approach. Overall, a total of 488 terms were used, which were categorized into common terms, based on consensus amongst authors. All these terms were content-analysed and a final set with 20 categories was formulated collating all terms (Table II).
Fig. 3 lists the 10 most often used skills by participants from the 4 countries. Table I summarizes the 10 most often used skills according to profession.
Fig. 3. Ten most-often used skills reported by the participants from the participating countries (n=532).
Table I. Ten most often used skills reported by participants according to profession (n = 532)
Prescription of physical activity programmes was the most frequently used skill reported (24.6%). This category included various terms for physical activity: exercise, physical training, mobilization/mobility, gait training, motor learning, strengthening exercise, passive exercise, range of motion, proprioceptive neuromuscular facilitation, stretching etc. Participants reported other skills such as: teaching activities of daily living (ADLs) and transfer techniques (13%); prescribing other allied health interventions (12.6%) (e.g. SLT interventions, hydrotherapy, prosthetic and orthotic interventions, thermotherapy, ultrasound, massage, cardio-respiratory interventions, electro-magnetic therapy, diet/nutrition); and patient and carer/family education (9.3%). Further analyses of these skills, based on the professional groups (PT, OT, rehabilitation physicians, other medical practitioners) showed these were consistent amongst all groups, irrespective of profession (Table I).
Although participants (65.2%) reported having sufficient training and/or knowledge to carry out these skills, they also reported a need for further knowledge. These related specifically to the need for regular professional skills-development programmes, more opportunity and access for training and to standardized assessment tools.
The 5 most consistent core skills included: prescribing physical activities and ADL training; other allied health interventions, comprehensive patient care, patient and carer/family education (Fig. 4).
Box 1 shows differences in participant responses regarding the core skills, treatment or methods, based on professional groups.
Fig. 4. Five core skills, treatment, methods for practice reported by the participants from the participating countries (n=532). ADLs: activities of daily living.
Box 1. Core skills/treatment/methods reported by different professional groups
Skill categories were matched with appropriate ICF categories (second level) based on the ICF-linking rules (20), (Table II). There was full agreement between reviewers. Skills grouped as “miscellaneous” (such as laboratory tests, repetitions, activity rescheduling, etc.) are not able to be linked to the standardized ICF checklist. As expected, the majority of skill categories linked with more than 1 ICF domain. Interestingly, 20 skill categories reported by participants linked with “personal factors” (12 categories), while 9 categories each linked with “activity and participation” and “environmental factors”.
Table II. Participant-reported skill categories linked to the International Classification of Functioning, Disability and Health (ICF) domains
Training and professional development were highlighted by participants as most helpful in current practice. Other most helpful factors identified included: good team work, a dedicated team, good communication skills, raising awareness and/or education regarding rehabilitation and disability amongst public and healthcare professionals, and a good working environment (Fig. 5).
Fig. 5. Five helpful factors in current practice reported by the participants from the participating countries (n=532).
There were many similarities in the barriers reported by participants, such as: marginalization of PwD, limited disability-inclusive policy and practice, and lack of sustainable long-term support programmes for PwD. Despite participants working with PwD, a quarter (27%) were not aware of the rights of PwD, and half (52.5%) did not understand the meaning of clinical governance. The key 5 barriers reported by participants are summarized in Fig. 6. Other themes included lack of: training in rehabilitation models of care, professional development, standardized outcome assessment, opportunities for career path and putting training into practice.
Fig. 6. Five key barriers in current practice reported by the participants from the participating countries (n=532). HCPs: healthcare professionals.
Many services lacked a multidisciplinary team approach. Some collaborated with other healthcare providers, such as primary care and/or community-based NGOs, where there was limited knowledge and/or training on disability issues and rehabilitation. Based on professional groups, the largest proportion of the participants (44.3%) reported preference for a rehabilitation specialist in their service, 32.1% preferred to have an OT, 16. 4% a PT, and 4.2% an SLT, as these were lacking in their respective services. The level of interest expressed by participants in research and networking activities was high across all disciplines.
This pilot study used a structured survey tool to gain insight from health professionals working in the rehabilitation field in LMICs, with a focus on clinical skills required in such settings. This survey tool provides valuable information about the nature of existing core skills used by professional groups and skills that participants reported as “a must” for rehabilitation in LMICs. Despite variation amongst the participating countries in terms of healthcare delivery, financing mechanisms and range of participant disciplines, the findings clearly highlighted a need for capacity-building, infrastructure, human resources, funding, training and awareness. Al-though previous reports suggest the existence of various rehabilitation programmes in LMICs (17, 21–23), many are yet to be evaluated, and it is unclear who runs, and/or what skills are needed to run these programmes. The findings indicate a need for a whole system approach, which more appropriately accommodates the capacity-building needs in rehabilitation.
The survey tool provides an efficient way of obtaining information on skills and identified gaps. The responses showed that key skills most frequently used were mostly of a generalized nature rather than discipline-specific (Box 1). This indicates that task-shifting was being implemented as a pragmatic response to heath workforce shortages to various degrees in each of the 4 countries. It was also understood that task-shifting is an efficient process, but is not a substitute for other investment in human resources in rehabilitation (11). The reported core skills overlapped amongst participants: capacity, team work, strong leadership, opportunities for upskilling and/or workforce development, implementation of evidence-based practice and tools, service delivery, funding and strategic investment in rehabilitation services. Likewise, reported barriers to current practice were specific to the setting and environment. These findings support other published reports (17, 23).
The participant reports of the skill categories used in austere settings, linked with the ICF checklist, reflect the complexity in management of PwD in the domains of “activities and participation”, “personal” and “environmental” factors. These indicate potential problems in mobility, domestic life, inter-personal and intimate relations, and major life areas (economic self-sufficiency, employment). The findings provide insight into the required skills in the course of functioning and health (over a longer time period), related to contextual factors and the overall effect on everyday activities and involvement in life situations of PwD.
With the rising costs of healthcare for PwD (and NCDs), the emerging role of rehabilitation (8, 24), the investment in development and/or training of the rehabilitation workforce in LMICs is critical. To develop a skilled rehabilitation workforce it is also important to examine the currently available healthcare systems (and rehabilitation services) and juxtapose these against the environment in which they are operationalized. The recommendations from the healthcare professionals in this report will assist in development of rehabilitation programmes in LMICs.
The strengthening of rehabilitation-inclusive healthcare systems in LMICs has been the focus of key organizations, such as the WHO (8), and by all member states (8, 24). There is increasing attention being given to the importance of healthcare systems, which encompass infrastructure, human resources, and financial resources to deliver healthcare services for PwD. Although healthcare systems in LMICs may have external funding provided by various international and charitable organizations for specific disability programmes, there is relative underfunding of the broader healthcare infrastructure in these countries (15). A functioning healthcare system is vital for the achievement of universal healthcare for populations in need, including PwD. The WHO also emphasizes developing healthcare systems both horizontally (e.g. assessing the elements needed for effective service delivery at all levels) and vertically (e.g. accounting for the support functions in a system) (8, 24); and advocates for rehabilitation as a key priority in the national healthcare agendas in LMICs.
In resource-limited settings, specialized multidisciplinary rehabilitation may not be feasible. Task-shifting and community-based rehabilitation programmes with a skilled workforce can serve as an alternative approach to provide long-term support to PwD (22, 25). Strengthening of public-private partnerships with involvement of local NGOs (and INGOs) will facilitate access to rehabilitation services. Low-cost technology (mobile phones) and tele-rehabilitation in many LMICs (where internet is available) can be effective in reaching PwD, especially in rural and remote areas, and need further investigation (15, 26). Political commitment from governments, more funding and investment in training and skill development of the existing workforce will be required to meet demand (12, 14).
The survey has several methodological limitations. First, this tool was modified by the authors from an existing survey, and has not been validated. However, the authors are experienced healthcare professionals with work experience in LMICs. Second, this is a cross-sectional study and does not test specific hypotheses through systematic analysis. Third, all responses were based on participants’ personal views, rather than objective data. A content-analysis technique, with consensus amongst the authors was used to summarize all responses derived from the survey. Lastly, there is acknowledgement that participants represent only a small proportion of healthcare professionals working with PwD in the 4 countries. Participant selection was by local institutions and beyond the control of authors. The snowballing/respondent-driven sampling methods used in this study, resulted in uneven distribution of professional groups and other relevant stakeholders (such as social work, PwD), and their views may have been missed, which may limit the generalizability and validity of findings. A purposeful random sampling method would have been ideal to minimize the selection bias; however, this was beyond our authority and scope of this pilot study. However, the study cohort included healthcare professionals from a wide geographical population (both urban and rural) and represents the currently available workforce. Participant heterogeneity was reflected in the representation of a variety of professional groups and the broad range of responses. The authors believe that the findings reflect the current situation regarding the skills of rehabilitation professionals (majority of PTs) in LMICs generally. They are unaware of any similar study conducted in these settings that address such issues. Future research will undertake further skills identification by using random or other sampling methods for inclusion of all professionals working (and other relevant stakeholders) in LMIC settings.
This study uses a systematic approach to gather information on current skills from the perspective of healthcare professionals working with PwD in LMICs. The findings highlight core skills and gaps in training, education, and available funding. Investment in capacity-building in rehabilitation will allow professional skills development strategies to meet particular needs described by participants, to deliver high-quality services to all PwD.
The authors thank all participating organizations and healthcare professionals for completing the surveys. The authors also acknowledge members of the Royal Melbourne Hospital Flying Faculty Team, specifically Dr Geoff Abbott, Ms Bronwyn Miller, Ms Lauren Fletcher and Ms Marlena Klaic for their assistance in conducting this survey.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize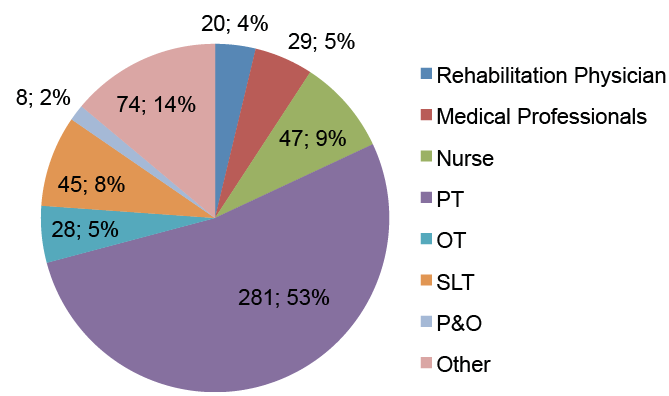 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize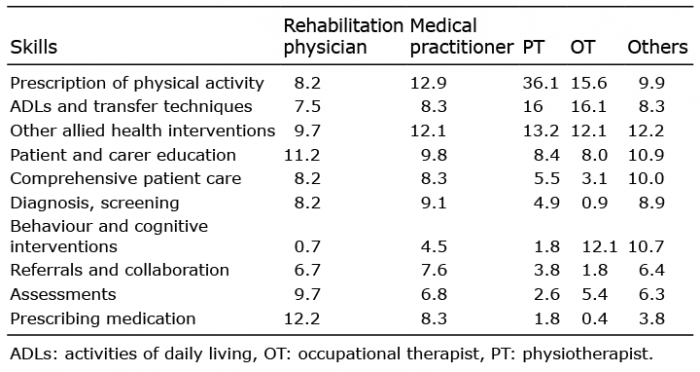 Click to show fullsize
Click to show fullsize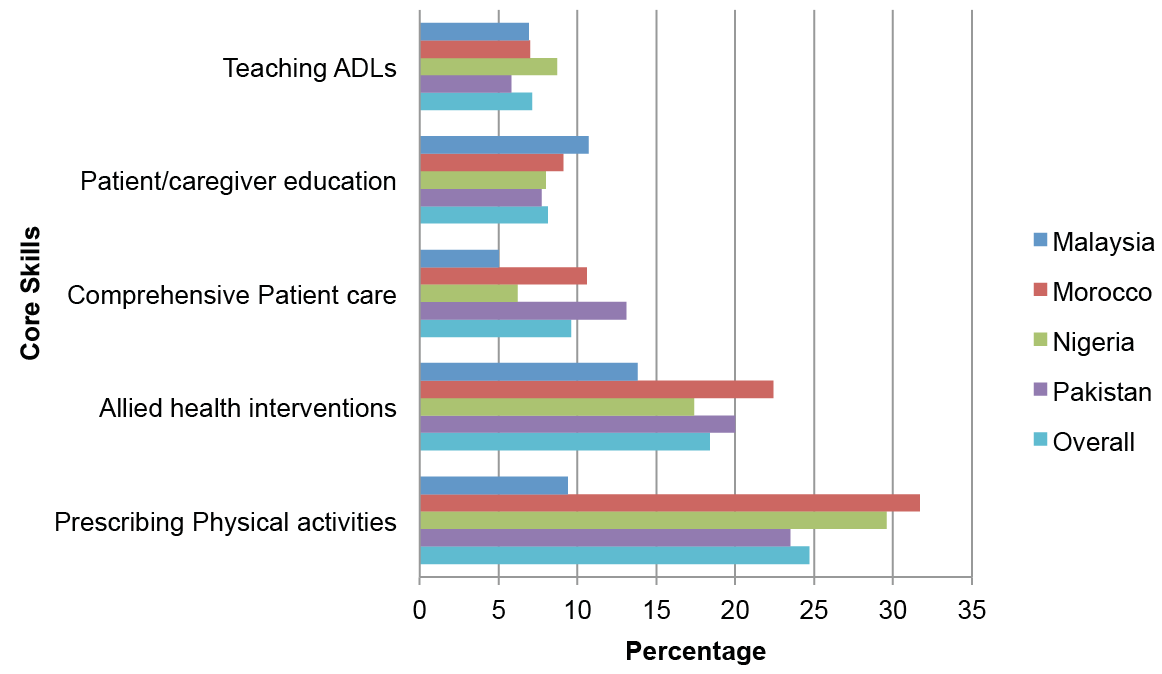 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize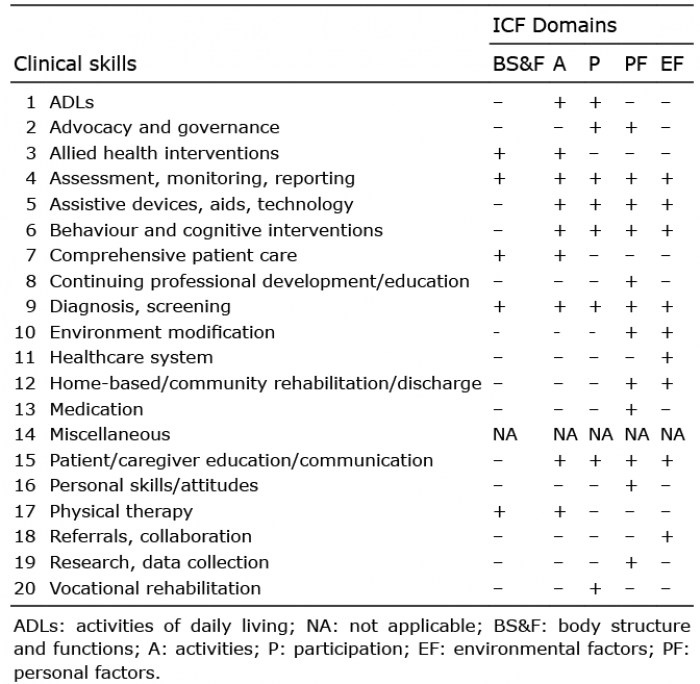 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize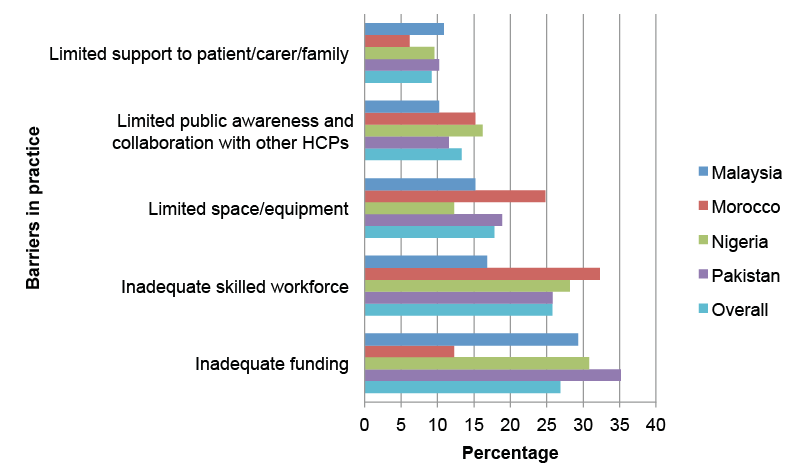 Click to show fullsize
Click to show fullsize